Will the FDA Approve New Alzheimer's Drugs in Late 2026
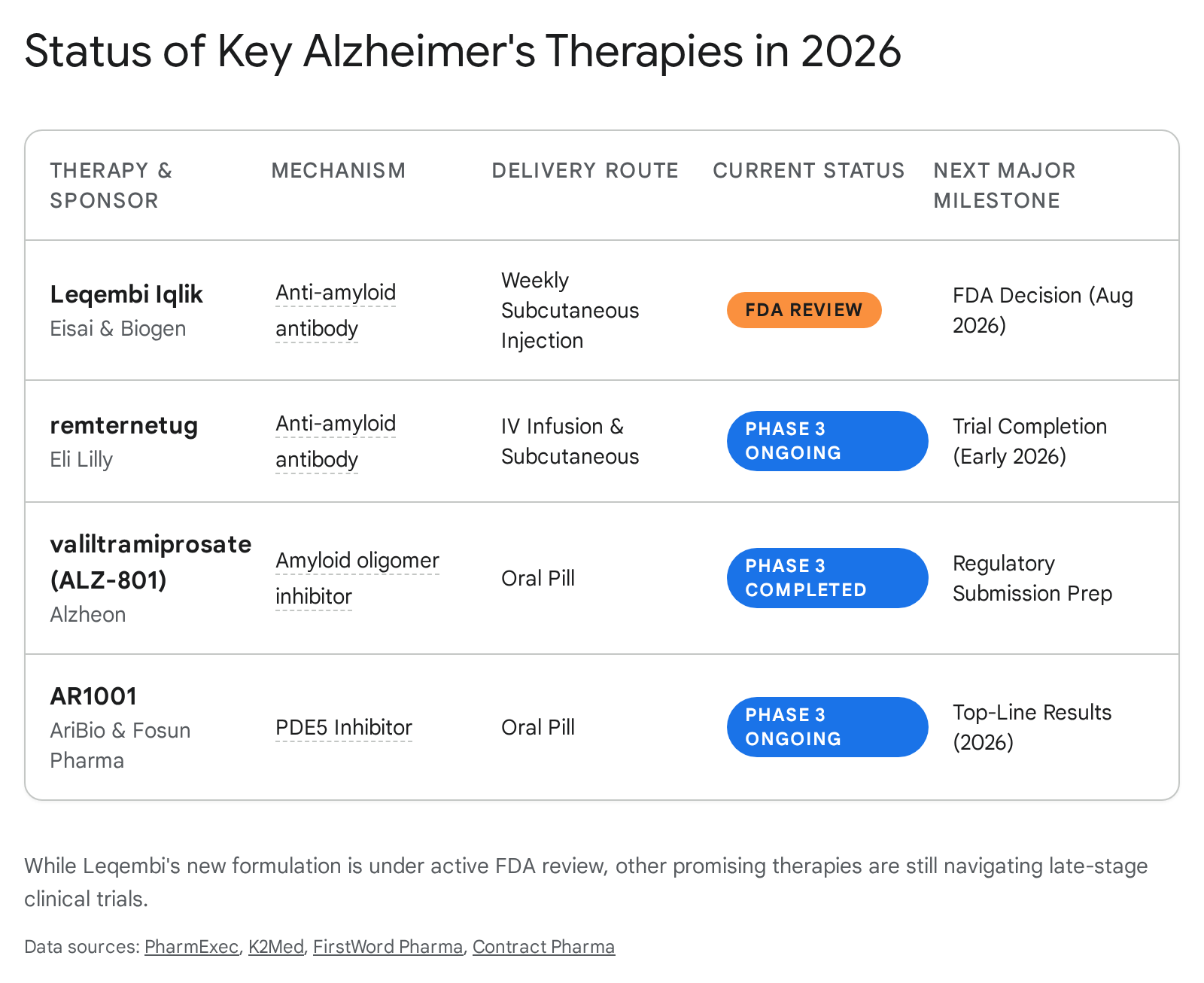
The FDA is not expected to approve any entirely new Alzheimer's disease-modifying therapies in the second half of 2026, as the most promising novel candidates are currently completing late-stage clinical trials. However, the agency is scheduled to make a major regulatory decision by August 24, 2026, regarding a highly anticipated at-home subcutaneous injection form of the already-approved drug Leqembi. While several other innovative therapies - including oral pills and a next-generation antibody - are reporting crucial trial data this year, their actual market approvals remain further down the pipeline.
The 2026 Alzheimer's Treatment Landscape
The treatment of Alzheimer's disease has undergone a paradigm shift over the last three years. For decades, the only available medications were symptom-targeted therapies that temporarily boosted neurotransmitter levels without halting the disease's underlying progression. The field was revolutionized by the FDA approvals of anti-amyloid monoclonal antibodies - specifically lecanemab (Leqembi) in 2023 and donanemab (Kisunla) in 2024 11.
These drugs are true disease-modifying therapies (DMTs). They work by binding to and clearing toxic amyloid-beta plaques from brain tissue, successfully slowing cognitive and functional decline by roughly 27% to 35% in early-stage patients 11.
The success of these first-generation antibodies has catalyzed massive investment in the Alzheimer's research pipeline. As of early 2026, there are 192 active clinical trials assessing 158 different drugs for Alzheimer's disease 23. Disease-modifying treatments now account for 73% of all agents in trials, while cognition-enhancing drugs make up 18%, and therapies targeting neuropsychiatric symptoms (such as agitation) comprise 10% 23.
Despite this booming pipeline, the current anti-amyloid treatments have exposed severe logistical bottlenecks in the healthcare system. The existing generation of drugs requires frequent intravenous (IV) infusions at specialized clinical centers, imposing a massive burden on patients and their caregivers. Furthermore, these drugs carry a distinct risk of amyloid-related imaging abnormalities (ARIA) - brain swelling and micro-hemorrhaging - which necessitates strict, ongoing MRI monitoring 54.
Consequently, the defining narrative for the second half of 2026 is not the introduction of a new drug, but the critical evolution of drug delivery methods and the pursuit of cleaner safety profiles.
The August 2026 Catalyst: Leqembi's Subcutaneous Formulation
For patients, families, and neurologists waiting for a major FDA action in late 2026, the focal point is a supplemental Biologics License Application (sBLA) submitted by Eisai and Biogen for Leqembi Iqlik 7.
Lecanemab (Leqembi) itself is already approved for early Alzheimer's disease. However, the pending application seeks approval for a once-weekly subcutaneous (under the skin) autoinjector intended to serve as a starting dose for treatment initiation 75.
The Burden of Intravenous Administration
Under the current standard of care, initiating Leqembi therapy requires patients to visit an infusion clinic every two weeks for an 18-month induction phase 59. Intravenous administration takes approximately one hour per session, not including travel and clinical wait times 1011. This ties up valuable infusion chairs at medical facilities and creates immense friction for patients experiencing cognitive decline.
In August 2025, the FDA approved a subcutaneous maintenance dose of Leqembi (360 mg) to be used only after a patient completes the initial 18-month IV regimen 57. The current application for Leqembi Iqlik seeks to bypass the IV induction phase entirely. The proposed starting regimen consists of a 500 mg weekly dose, administered by the patient or a caregiver as two 250 mg injections using an autoinjector, which takes about 15 seconds per injection 1011.
If approved, this would allow patients to initiate and maintain their anti-amyloid therapy entirely at home from day one, radically altering the commercial and clinical landscape by shifting care out of the hospital and into the living room 511.
The FDA Review Extension
The FDA originally granted this application a priority review with a target Prescription Drug User Fee Act (PDUFA) action date of May 24, 2026 10. However, in early May, the FDA requested additional information from Eisai and Biogen 75.
The submission of these requested materials was classified by the FDA as a "major amendment," which automatically triggered a standard three-month extension of the review timeline 751213. The new expected decision date is August 24, 2026 71415.
Both pharmaceutical companies have stated that the FDA has not raised any concerns regarding the actual approvability, safety, or efficacy of the subcutaneous starting dose; the delay appears strictly procedural to allow adequate time to review the data 75.
International Regulatory Headwinds
While the FDA deliberates on the delivery method, global regulators have taken a more cautious stance on the drug itself. In mid-2024, the European Medicines Agency's Committee for Medicinal Products for Human Use (CHMP) initially recommended against approving Leqembi, arguing the risk of brain swelling and bleeding outweighed the modest cognitive benefits 16.
In late 2024, the CHMP reversed course, issuing a positive opinion but heavily restricting the drug's use. The EMA recommended Leqembi only for patients who have one or zero copies of the APOE4 gene 4166. Individuals with two copies of this gene (APOE4/4 homozygotes) have a substantially higher risk of experiencing severe ARIA side effects 467. The EMA is currently reviewing further post-opinion safety data, demonstrating the intense, ongoing global scrutiny applied to anti-amyloid therapies 1619.
Comparing Leqembi Delivery Methods
| Feature | Current Standard (Leqembi IV) | Proposed Alternative (Leqembi Iqlik SC) |
|---|---|---|
| Administration Route | Intravenous (IV) infusion | Subcutaneous (SC) autoinjection |
| Location | Clinical infusion center | At home (self or caregiver) |
| Frequency | Every 2 weeks | Once weekly |
| Dose at Initiation | 10 mg/kg biweekly | 500 mg weekly (two 250mg injections) |
| Administration Time | Approx. 1 hour per session | Approx. 15 seconds per injection |
Next-Generation Therapies: Nearing the Finish Line
While the optimization of Leqembi is the immediate focus for late 2026, the broader Alzheimer's pipeline is maturing rapidly. Several highly anticipated drug candidates are wrapping up pivotal Phase 3 trials this year. Because analyzing massive trial data sets and navigating the FDA review process typically takes 6 to 12 months, none of the following novel drugs are expected to receive FDA approval before 2027.
Remternetug: Eli Lilly's Follow-Up Antibody
Following the success of Kisunla (donanemab), Eli Lilly is aggressively developing its next-generation anti-amyloid antibody, remternetug 2021.
Like donanemab, remternetug is engineered to target N3pG-amyloid beta, a specific pyroglutamated form of the protein found in deposited plaques 2223. By binding directly to these plaques, remternetug facilitates microglial-mediated clearance, effectively directing the brain's immune system to scrub the toxic deposits away 238.
What makes remternetug distinct is its delivery strategy. Acknowledging the infusion bottlenecks of earlier drugs, Eli Lilly is testing remternetug concurrently as an intravenous infusion and a subcutaneous injection from the very beginning of its development 2021.
Lilly is currently evaluating the drug in the massive Phase 3 TRAILRUNNER-ALZ 1 trial, which involves 1,667 participants and is expected to conclude the blinded portion in early-to-mid 2026 20222325. Interim Phase 1 and 2 data were highly encouraging regarding plaque removal; by day 169, 75% of participants receiving the highest doses achieved complete amyloid clearance 2627. However, early data also revealed instances of ARIA, confirming that while the drug is potent, it shares the exact same safety liabilities as older anti-amyloid antibodies 2326.
Top-line data from TRAILRUNNER-ALZ 1 is expected in the first half of 2026 2128. If the data is positive, Eli Lilly could file a Biologics License Application later this year, setting up a potential FDA decision in 2027.
Primary Prevention in Young Adults
Beyond treating early symptomatic Alzheimer's, remternetug is being deployed in a fascinating primary prevention trial. The DIAN-TU-002 platform trial, led by Washington University, is administering remternetug to young adults - some as young as 18 - who carry genetic mutations that guarantee they will develop early-onset Alzheimer's in their 30s or 40s 8930. The study aims to determine whether aggressively clearing amyloid before cognitive symptoms ever appear can prevent the disease entirely 930.
Valiltramiprosate (ALZ-801): The Quest for an Oral Disease Modifier
A major long-term goal in Alzheimer's research is developing a disease-modifying therapy that can be taken as a daily pill. Valiltramiprosate (ALZ-801), developed by Alzheon, is currently the furthest along in this quest.
Rather than clearing existing, insoluble plaques like antibody treatments do, valiltramiprosate works further upstream in the amyloid cascade 203132. It is an oral prodrug of homotaurine designed to prevent healthy, free-floating beta-amyloid proteins from misfolding and clumping together into soluble, neurotoxic oligomers 313233. Because these soluble oligomers are increasingly viewed as the primary drivers of synaptic damage, stopping their formation could theoretically halt cognitive decline without triggering the inflammatory plaque-removal process that causes ARIA 73234.
The drug's recent clinical path has been highly nuanced. Alzheon tested the drug in a pivotal Phase 3 trial called APOLLOE4, which exclusively enrolled patients with two copies of the APOE4 gene 313410. This population was chosen because they have the highest genetic risk of aggressive Alzheimer's and, conversely, the highest risk of life-threatening brain bleeding if given standard IV antibody treatments 734.
In early 2025, Alzheon announced that the APOLLOE4 trial failed to meet its primary clinical endpoint of significantly slowing cognitive decline across the overall study population 3637. However, deeper prespecified analyses revealed a powerful silver lining. In patients at the absolute earliest stage of the disease - Mild Cognitive Impairment (MCI) - the drug showed a nominally significant 52% benefit in slowing cognitive decline and doubled their preservation of daily function compared to a placebo 3638.
Furthermore, biomarker data presented at the 2026 AD/PD Conference showed the drug successfully reduced levels of plasma p-tau217 (a key blood biomarker for Alzheimer's pathology) by up to 36% and significantly protected against hippocampal brain shrinkage 3738. Notably, the drug achieved this with a favorable safety profile and no increased risk of brain edema (ARIA-E) 73110.
Due to the missed primary endpoint in the broad population, Alzheon will not be filing for FDA approval in 2026. Instead, based on the robust biomarker correlations and clinical outcomes in the MCI subgroup, the company plans to initiate a new, confirmatory Phase 3 trial specifically targeting MCI APOE4 homozygotes later in 2026 373839.
AR1001: Repurposing PDE5 Inhibitors
Another oral candidate generating significant interest is AR1001 (mirodenafil), currently under development by AriBio 2040.
AR1001 is a phosphodiesterase-5 (PDE5) inhibitor. While this mechanism is most famously utilized by erectile dysfunction medications like Viagra and Cialis, large observational health studies have repeatedly noted that patients taking PDE5 inhibitors exhibit significantly lower rates of Alzheimer's disease 2041.
Researchers hypothesize that PDE5 inhibitors can cross the blood-brain barrier and exert multiple neuroprotective effects, including improving cerebral blood flow, suppressing inflammatory responses, and inhibiting tau protein phosphorylation 4243.
AriBio is currently testing the drug in a massive, 1,535-person Phase 3 global trial known as POLARIS-AD 404143. The trial completed patient enrollment in 2025 and requires a 52-week double-blind treatment phase followed by an extension phase 404243. Top-line results from this pivotal study are anticipated in the latter half of 2026, meaning any potential regulatory submission will likely occur in 2027 4042.
The Evolving Role of Biomarkers and Precision Medicine
The data emerging in 2026 highlights a broader shift in Alzheimer's treatment: the move away from one-size-fits-all medicine toward precision neurology guided by fluid biomarkers and genetics.
Blood-based biomarker testing is rapidly replacing expensive PET scans and invasive spinal taps for diagnosing the disease and determining trial eligibility 111. Assays measuring plasma p-tau217 - which correlates strongly with both amyloid and tau pathology - have gained FDA clearance as reliable diagnostic aids 53839.
This precision allows researchers to stratify patients more accurately. As seen with the EMA's restriction on Leqembi and Alzheon's focus on ALZ-801, a patient's APOE4 genetic status now directly dictates their risk profile and therapeutic options 4734. In the near future, standard clinical practice will likely require concurrent blood biomarker confirmation and genetic testing before any prescription is written.
Systemic Challenges: Trial Diversity and Funding Disruptions
As the pipeline expands, two systemic challenges threaten to bottleneck the development of future Alzheimer's therapies.
The Trial Diversity Deficit
Alzheimer's disease disproportionately impacts Black and Hispanic populations, yet the data generated by the pharmaceutical industry rarely reflects this reality. A systematic review of Alzheimer's trials conducted between 2001 and 2019 found that the median percentage of white participants was 94.7%, with no significant improvement over two decades 12.
Unfortunately, this trend has persisted into the modern era of disease-modifying therapies. In Eli Lilly's TRAILBLAZER-ALZ 2 trial for Kisunla, 90.9% of the treatment group was white, while Eisai's CLARITY AD trial for Leqembi reported a 76.3% white cohort 13. Recent early Phase 3 data for remternetug similarly showed a 91.4% white participant base 26.
This lack of diversity is a scientific liability. Genetic variations, cardiovascular comorbidities, and biomarker thresholds can differ materially across ethnic groups, meaning a drug's safety and efficacy profile might not generalize to the broader population 121347. Regulators are applying increasing pressure on drug sponsors to rectify this. Moving forward, companies are adopting decentralized trial models and partnering with community-based clinics - as seen in AriBio's POLARIS-AD trial - to recruit populations that accurately reflect the disease's demographics 4148.
Macroeconomic Fragility
In addition to demographic challenges, the US clinical trial ecosystem experienced a severe shock in early 2026 due to sudden disruptions in federal research funding. A recent analysis revealed that NIH grant terminations abruptly disrupted 383 active clinical trials, impacting over 74,000 enrolled patients and wiping out $1.81 billion in funding 28.
While infectious disease and prevention trials bore the brunt of the impact, the sheer scale of the disruption has forced pharmaceutical sponsors, contract research organizations (CROs), and academic sites to rapidly redesign their continuity plans 28. For longitudinal studies that rely on years of uninterrupted patient tracking - such as Alzheimer's prevention trials - funding instability poses a structural risk that could delay the pipeline long past 2026.
Bottom line
Readers monitoring the FDA's actions in the second half of 2026 should not expect the approval of a completely novel Alzheimer's drug. Instead, the major catalyst is the FDA's upcoming August 24 decision on Leqembi Iqlik, a subcutaneous formulation that could transform patient care by moving treatments out of infusion centers and into the home. While highly promising experimental therapies - such as the next-generation antibody remternetug and the oral drugs valiltramiprosate and AR1001 - are reporting vital Phase 3 data this year, they remain firmly in the clinical testing phase, meaning their potential market debuts are still a few years away.