The Tau Alzheimer's Pipeline to Watch at AAIC 2026
The 2026 Alzheimer's Association International Conference (AAIC) in London will heavily feature clinical trial data from a new wave of therapies targeting the tau protein, including Biogen's gene-silencing diranersen and Eisai's etalanetug. Because the spread of tau tangles correlates directly with neuronal death and cognitive decline, researchers are increasingly looking to combine these emerging tau inhibitors, antibodies, and vaccines with recently approved amyloid-clearing drugs in an effort to fully halt disease progression.
The Spark and Fire: Why Is Tau the Next Target?
For decades, the pharmaceutical industry's pursuit of Alzheimer's disease treatments was defined by a staggering failure rate. Between 2002 and 2012, Alzheimer's drug development experienced a 99.6% clinical trial failure rate, leading many companies to severely limit their investments in the neurodegeneration space 123. Historically, the vast majority of this research capital was poured into the "amyloid hypothesis" - the premise that clearing extracellular amyloid-beta plaques from the brain would effectively stop the disease 456.
That persistence eventually yielded the first generation of disease-modifying therapies. Monoclonal antibodies such as lecanemab and donanemab, approved in recent years, successfully clear amyloid plaques and have been shown to modestly slow cognitive decline in early-stage patients 578. However, these drugs do not cure the disease, and their clinical benefits remain incremental, prompting researchers to look beyond amyloid to the disease's second major pathological hallmark: the tau protein 489.
In a healthy human brain, tau is a vital protein that helps stabilize microtubules, the internal support structures that transport nutrients within neurons 4610. In Alzheimer's disease, tau undergoes abnormal post-translational modifications, becoming hyperphosphorylated. It detaches from the microtubules and clumps together to form toxic neurofibrillary tangles inside the cells 4610.
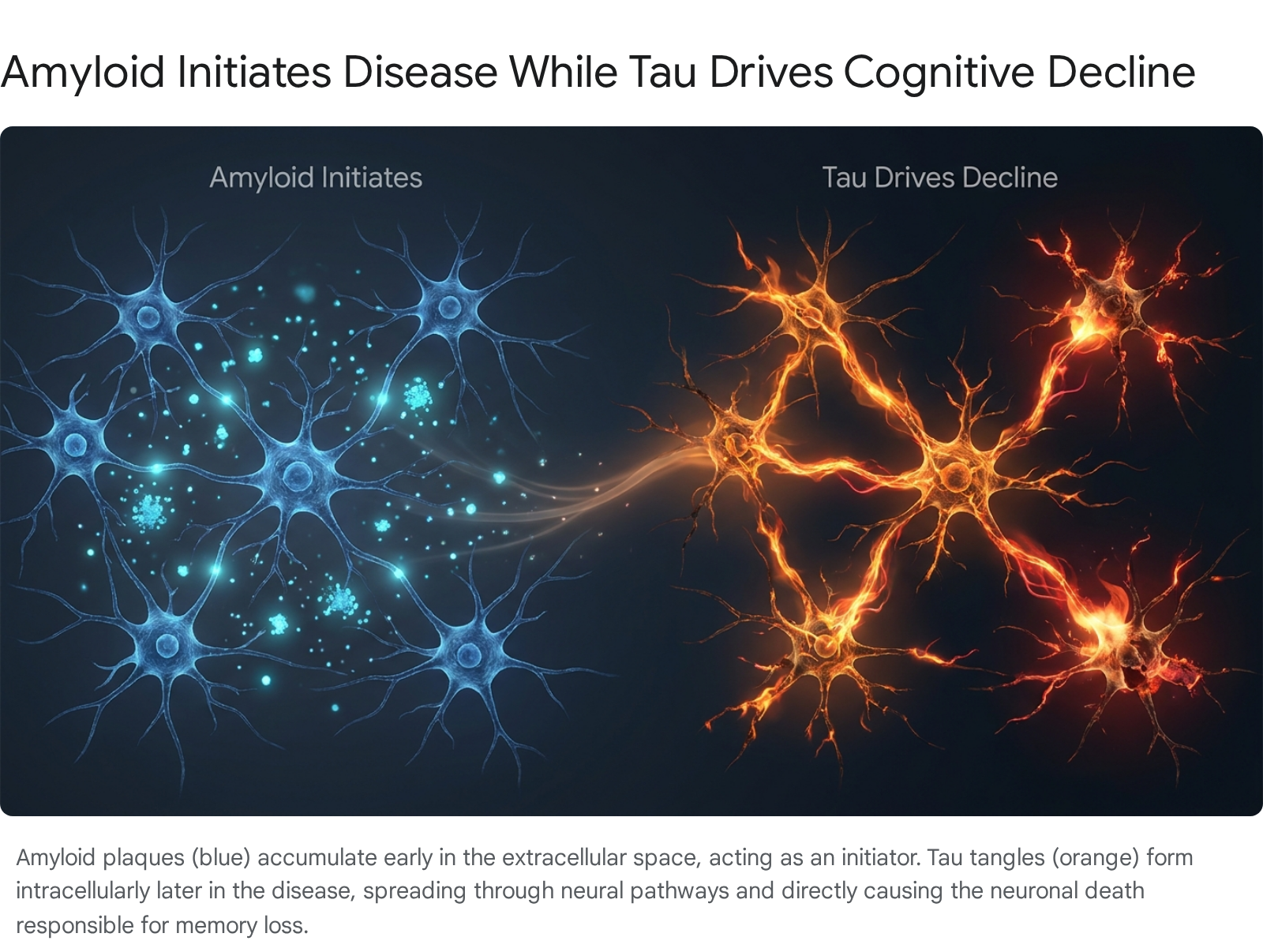
Neuroscientists and drug developers increasingly rely on the "spark and fire" analogy to explain the relationship between these two proteins. Amyloid plaques act as the spark. They often accumulate quietly in the extracellular space of the brain a decade or more before any clinical symptoms appear 51112. In fact, up to 30% of cognitively normal elderly individuals harbor significant amyloid burdens without showing signs of dementia 5.
But tau is the fire. The spread of tau tangles outward from the brain's memory centers correlates tightly with brain cell death, brain shrinkage (atrophy), and the actual onset of memory loss and functional decline 11121314. As researchers have discovered, the presence of cortical amyloid seems to act as an accelerant, creating a permissive environment that dramatically increases the speed of tau propagation to distal brain regions 41116.
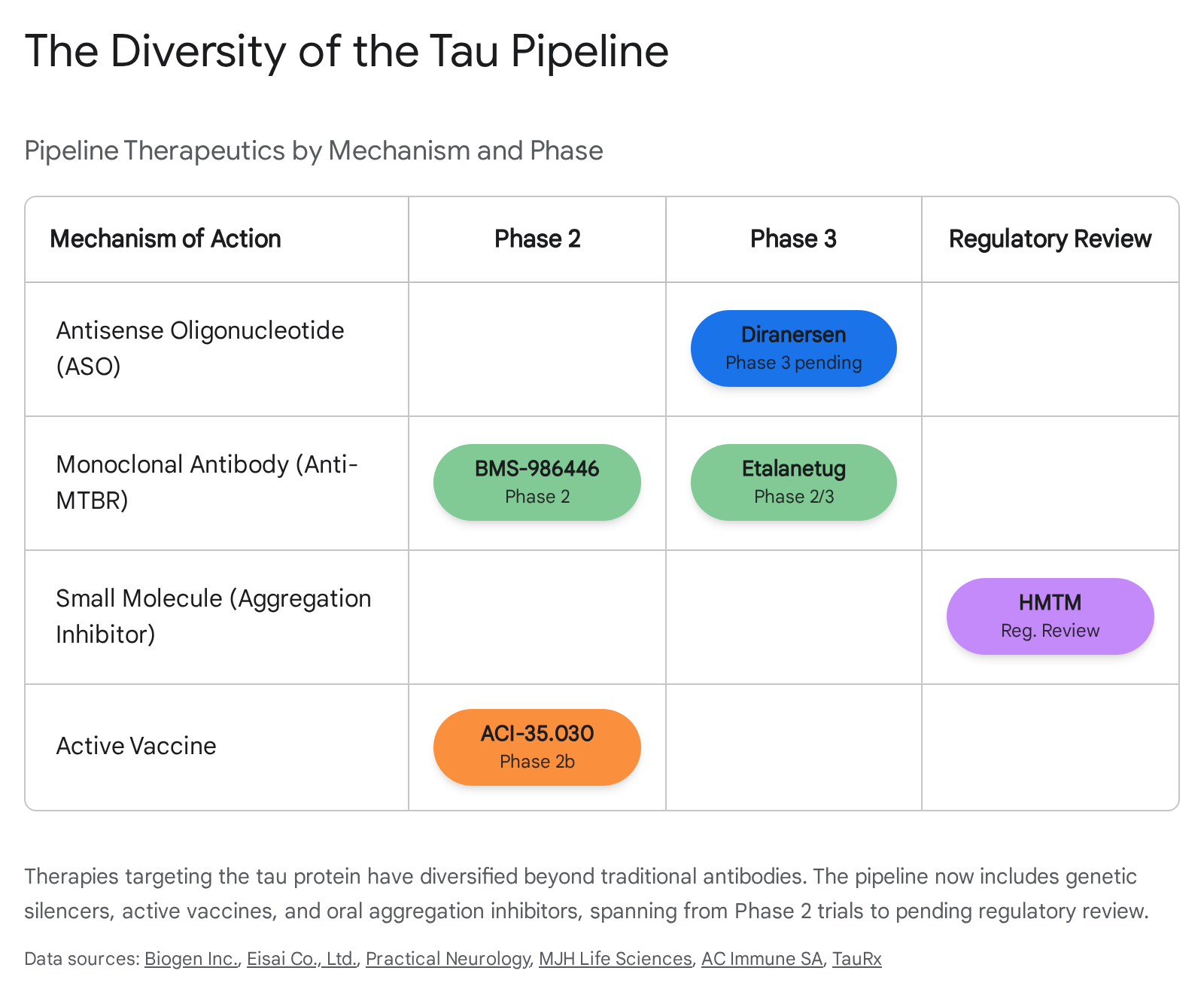
Reflecting this biological reality, the Alzheimer's clinical trial pipeline has undergone a radical transformation. As we look toward the 2026 data readouts, tau-targeted agents now make up approximately 20% of the entire Alzheimer's drug development pipeline - a massive increase from just 6% a decade ago 1516. Concurrently, the percentage of drugs dedicated solely to targeting amyloid has decreased from 33% to roughly 20%, signaling a much more diversified, multi-targeted approach to treating the disease 15.
How Do Tau Therapies Actually Work?
Developing drugs for tau is notoriously complex. Because tau tangles form intracellularly (inside the neuron), traditional large-molecule drugs like antibodies have a difficult time reaching them 5. As a result, the pharmaceutical industry has developed a wide array of modalities to attack tau at different stages of its lifecycle, from genetic production to extracellular spread.
Monoclonal Antibodies: Catching the Spread
Monoclonal antibodies are designed to intercept tau pathology as it spreads. According to the "tau propagation hypothesis," toxic tau seeds are released from dying neurons into the extracellular space, where they are taken up by healthy recipient cells, triggering a chain reaction of tangle formation 101718.
Passive immunotherapies - infusions of laboratory-engineered antibodies - aim to bind to these extracellular tau seeds and neutralize them before they can infect adjacent cells 192021. Early generations of anti-tau antibodies targeted the N-terminus of the protein and universally failed in clinical trials 1922. Today, next-generation antibodies primarily target the mid-region or the microtubule-binding region (MTBR) of tau, which is believed to be the critical domain that drives aggregation and seeding 172223.
Antisense Oligonucleotides (ASOs): Silencing Production
Rather than trying to mop up toxic tau after it has already formed, genetic therapies attempt to stop the brain from producing the protein in the first place. Antisense oligonucleotides (ASOs) are synthetic strands of DNA or RNA that bind to specific messenger RNA (mRNA) molecules 24.
In the case of Alzheimer's, tau-targeting ASOs bind to the MAPT mRNA, preventing the cell's machinery from translating it into tau protein 2425. By lowering the overall concentration of tau in the brain, researchers hope to prevent the cascade of hyperphosphorylation and aggregation 24. Because ASOs cannot cross the blood-brain barrier easily, they are typically administered via intrathecal injection directly into the cerebrospinal fluid 2526.
Active Vaccines: Training the Immune System
Active immunotherapies aim to stimulate the patient's own immune system to generate a durable, polyclonal antibody response against pathological forms of tau 202527.
Unlike monoclonal antibody infusions, which require frequent dosing and only provide one specific type of antibody, a vaccine encourages the body to produce a diverse array of antibodies continuously 2427. Modern tau vaccines utilize liposomal formulations or specific antigen platforms to target only the hyperphosphorylated, neurotoxic forms of tau, deliberately avoiding an autoimmune response against the healthy, physiological tau that neurons need to function 2728.
Small Molecules: Inhibiting Aggregation
Small molecule drugs offer the distinct advantage of oral administration and the ability to easily cross the blood-brain barrier to enter neurons 242529.
These compounds utilize various mechanisms of action. Some are designed as aggregation inhibitors, which bind directly to tau proteins to prevent them from misfolding and clumping together into fibrils 102130. Others function as enzyme inhibitors, targeting the specific kinases responsible for hyperphosphorylating tau or the enzymes involved in its post-translational modification 7102125.
Top Tau Candidates Advancing in 2026
The AAIC 2026 meeting in London will serve as a critical proving ground for several heavily funded tau programs. As the industry shifts away from monotherapies, many of these candidates are being evaluated for their potential to be combined with standard-of-care amyloid drugs.
The table below outlines the most prominent tau-targeting assets currently in late-stage development or regulatory review.
| Drug Candidate | Developer | Modality / Mechanism | Current Phase | 2026 Status & Focus |
|---|---|---|---|---|
| Diranersen (BIIB080) | Biogen / Ionis | Antisense Oligonucleotide | Advancing to Phase 3 | Missed Phase 2 primary endpoint but advancing based on cognitive benefit signals; detailed data expected at AAIC 3132. |
| Etalanetug (E2814) | Eisai | Anti-MTBR Antibody | Phase 2/3 | Being tested in combination with lecanemab; shows dramatic reductions in tau biomarkers 173334. |
| HMTM | TauRx | Small Molecule (Oral) | Regulatory Review | Under accelerated review by the UK MHRA; pending response to regulatory questions 293536. |
| BMS-986446 | BMS / Prothena | Anti-MTBR Antibody | Phase 2 | Granted FDA Fast Track designation; TargetTau-1 trial fully enrolled 233741. |
| ACI-35.030 | AC Immune / Janssen | Active Vaccine | Phase 2b | Testing in 500 preclinical patients to see if it can prevent symptom onset 272838. |
Biogen's Diranersen (BIIB080): The Genetic Approach
One of the most highly anticipated presentations at AAIC 2026 will be the detailed readouts from Biogen and Ionis Pharmaceuticals' Phase 2 "CELIA" trial for diranersen (formerly BIIB080) 3243.
Diranersen is an investigational ASO designed to reduce tau protein at its source by targeting MAPT mRNA 39. In May 2026, Biogen announced topline results from the CELIA study, which enrolled 416 patients with mild cognitive impairment or mild Alzheimer's dementia who had not previously received anti-amyloid therapy 3132. The drug was tested across three intrathecal dosing regimens over a 76-week period 3132.
The topline announcement revealed a complex picture. Diranersen failed to meet its primary endpoint, which was defined as a dose-response change in disease severity measured by the Clinical Dementia Rating Scale Sum of Boxes (CDR-SB) 313240. In drug development, researchers typically expect higher doses to yield more pronounced clinical effects; however, diranersen did not follow this conventional dose-response pattern 40.
Despite missing the primary goal, Biogen announced it will aggressively advance the drug into Phase 3 registrational trials 313239. The company pointed to pre-specified analyses showing that diranersen successfully reduced tau pathology and slowed clinical decline across all tested doses 2631. Surprisingly, the most pronounced cognitive benefit was observed in the lowest dose cohort - 60 mg administered every 24 weeks 263140. The presentation of the full dataset at the London conference will face intense scrutiny, as analysts look to understand where Biogen is drawing its confidence for a Phase 3 investment and whether the cognitive slowing is statistically and clinically robust 3239.
Eisai's Etalanetug (E2814): The Combination Pioneer
Eisai, the company behind the successful amyloid drug lecanemab, is pursuing a sophisticated combination therapy approach with its tau candidate, etalanetug (E2814) 1734.
Etalanetug is a monoclonal antibody specifically designed to bind to the microtubule-binding region (MTBR) of extracellular tau, preventing the seeding and propagation of tau pathology between neurons 171934. Eisai's clinical strategy explicitly acknowledges the "spark and fire" reality of the disease: etalanetug is currently being evaluated in clinical trials added on to a background standard-of-care treatment of lecanemab 193334.
The drug is being tested in the Phase 2/3 "Tau NexGen" trial for dominantly inherited Alzheimer's disease (DIAD) and a Phase 2 global randomized trial (Study 202) for sporadic early Alzheimer's 173334. Early data has been highly encouraging regarding target engagement. Etalanetug has been shown to dramatically reduce levels of eMTBR-tau243 - a highly specific cerebrospinal fluid and plasma biomarker for tau tangles - by 62% at three months and 89% at nine months 1934. AAIC 2026 will likely feature critical updates on whether these profound biomarker reductions are translating into sustained cognitive preservation for patients on the dual therapy 1746.
TauRx's HMTM: The Pending Regulatory Decision
The most immediate regulatory milestone in the tau space belongs to TauRx Pharmaceuticals and its drug hydromethylthionine mesylate (HMTM). Unlike the complex intravenous infusions or intrathecal injections required by antibodies and ASOs, HMTM is a simple oral tablet 303541. It functions as a tau aggregation inhibitor, while also providing a secondary symptomatic benefit by increasing acetylcholine levels in the hippocampus 293041.
HMTM has a long and somewhat controversial history in clinical development, with previous large-scale trials failing to meet primary endpoints 6. TauRx maintains that these historical issues were methodological, stemming from control group complications 42. To rectify this, the company published confirmatory data in early 2026 from its Phase 3 LUCIDITY trial, comparing participants receiving 16 mg/day of HMTM against matched external placebo controls from the FDA-sponsored Critical Path for AD database 424943. This analysis demonstrated that early-stage patients experienced statistically significant cognitive improvement over 18 months, with benefits maintained out to two years 304251. Furthermore, blood tests showed a 95% reduction in neurofilament light chain (NfL), indicating a massive decrease in active brain cell death 293041.
TauRx submitted a Marketing Authorisation Application to the UK's Medicines and Healthcare products Regulatory Agency (MHRA), which is reviewing the drug under a 150-day accelerated assessment pathway 354445. In late 2025, the MHRA requested additional information before making a final determination, and TauRx confirmed it expects to submit this data by late February 2026 3646. Consequently, a landmark regulatory decision could align closely with the July AAIC meeting 46. If approved, HMTM would be the first disease-modifying oral therapy for Alzheimer's disease available in the UK 2945.
ACI-35.030: Moving into Preclinical Prevention
While many companies are targeting patients who already exhibit mild cognitive impairment, AC Immune and its partner Janssen are attempting to move upstream with their active vaccine, ACI-35.030 (also known as JNJ-64042056) 2728.
The vaccine utilizes a liposomal formulation designed to stimulate the generation of antibodies specifically against pathological phosphorylated tau (pTau), while avoiding immune responses against healthy tau 272847. Phase 1b/2a data demonstrated that a single dose induced a rapid, potent, and sustained polyclonal antibody response in 100% of participants, with no clinically relevant safety issues 272847.
Based on this robust immune activation, the vaccine was selected to advance into the Phase 2b "ReTain" trial 2738. This trial represents a major shift in Alzheimer's research methodology: it is enrolling 500 preclinical Alzheimer's patients 272838. These are individuals who are cognitively healthy but have biomarker evidence of amyloid and tau pathology 2838. The goal is to determine if early vaccination can halt the disease process before memory loss ever begins, utilizing a primary endpoint measuring decline on a cognitive composite score over four years 2838.
What Can We Learn from Recent Tau Trial Failures?
Despite the optimism surrounding the 2026 pipeline, targeting tau remains an exceptionally difficult endeavor. The field was recently humbled by the failure of two prominent mid-stage antibody programs, providing critical lessons on trial design and patient selection 720.
Posdinemab and the Diversity Challenge
In late 2025, Johnson & Johnson discontinued the Phase 2b "AuTonomy" trial of its tau-targeted monoclonal antibody posdinemab (JNJ-63733657) 720. Designed as a proof-of-concept study in early-stage Alzheimer's, an interim review revealed that the antibody failed to achieve statistical significance in slowing clinical decline 720.
Beyond the efficacy failure, the posdinemab trial illuminated a severe ongoing problem in Alzheimer's drug development: demographic disparities in trial enrollment 48. Preliminary data showed that out of 2,563 participants screened, nearly 80% failed to meet eligibility criteria 48. Crucially, the screen failure rate was significantly higher among Black/African American individuals (86.4%) compared to White participants (80.5%) and Asian participants (73.3%) 48. The primary reason for exclusion across all groups was a lack of elevated plasma pTau217 concentrations - a strict biomarker requirement 48. Black/African American participants were also nearly twice as likely to fail the clinical inclusion criteria for early disease progression 48. These figures suggest that strict biomarker thresholds may inadvertently exclude diverse populations, reflecting broader, systemic disparities in how and when Alzheimer's is detected across different demographics 48.
Bepranemab and the Search for Responders
Similarly, UCB reported that its anti-tau antibody, bepranemab, failed to meet its primary endpoint (change in CDR-SB) in the Phase 2a "TOGETHER" trial 224950. The readout prompted UCB's partner, Roche, to exit a $120 million licensing agreement for the drug 22.
However, UCB remains encouraged by the drug's target engagement. Bepranemab successfully reduced tau accumulation in key brain regions by 33% to 58% relative to placebo over 80 weeks, and patients demonstrated nominally significant improvements in secondary cognitive measures like the ADAS-Cog14 scale 22495051.
The most vital lesson from the bepranemab trial emerged during subgroup analyses. The data showed that high-dose bepranemab provided a consistent clinical benefit across multiple measures specifically in patients who had a low tau burden at baseline and who did not carry the APOE4 genetic risk variant 224951. In stark contrast, APOE4 carriers with high baseline tau saw no clinical benefit whatsoever from the treatment 4951. This reinforces the theory that anti-tau antibodies may only be effective during a very specific, early window of the disease, and that genetic factors play a massive role in treatment response 51449.
What to Expect at the London Conference
The scientific program at AAIC 2026 (July 12 - 15) is designed to reflect this transitional moment in dementia research 52. Plenary sessions will heavily feature discussions on biomarker integration and the future of combination therapies 53.
Notably, Dr. Takaomi C. Saido of the RIKEN Center for Brain Science will deliver a plenary session exploring the intersection of amyloid and tau, while Dr. Betty Tijms of Amsterdam UMC will present on the proteomic subtypes of Alzheimer's and how identifying these subtypes will influence future drug development 53. Furthermore, dedicated workshops and preconferences (July 10-11) will focus on speech and language biomarkers, as well as the implementation of clinical technologies to refine trial cohorts 54.
The conference will also serve as a critical forum to debate the ethics and mechanics of next-generation clinical trial design 1546. Because the historic 99% failure rate was partly driven by poor patient selection - where up to 30% of enrolled patients lacked actual Alzheimer's pathology - modern trials now mandate PET imaging or fluid biomarkers for enrollment 25. However, as therapies like diranersen and etalanetug mature, researchers face a new dilemma: should experimental tau drugs continue to be tested as monotherapies against placebos, or do ethical considerations demand they be tested as add-on treatments for patients already receiving an amyloid-clearing standard of care? 46
Bottom line
The 2026 Alzheimer's Association International Conference marks a definitive turning point for the industry, as the research pipeline pivots aggressively from amyloid clearance to tau suppression. Recent Phase 2 setbacks for antibodies like posdinemab highlight the sheer complexity of neutralizing tau and the challenges of inclusive trial design. However, the advancement of diverse modalities - including Biogen's genetic silencer diranersen, Eisai's combination-focused etalanetug, and TauRx's pending oral therapeutic - offers concrete hope. Ultimately, the success of this pipeline will depend on whether these therapies can prove undeniable cognitive preservation in rigorous late-stage trials, and whether regulators agree that combining them with amyloid treatments is the key to finally halting Alzheimer's disease.