What Centanafadine Offers for ADHD Treatment in 2026
Centanafadine is an investigational, once-daily non-stimulant medication currently under priority review by the U.S. Food and Drug Administration (FDA) for the treatment of attention-deficit/hyperactivity disorder (ADHD) in children, adolescents, and adults. By uniquely targeting three key neurotransmitters - norepinephrine, dopamine, and serotonin - it aims to deliver effective symptom control with significantly fewer side effects and a lower risk of abuse than traditional stimulants. An official FDA approval decision is expected by July 24, 2026.
The State of ADHD Treatment in 2026
Attention-deficit/hyperactivity disorder (ADHD) is a widespread, chronic neurodevelopmental condition characterized by persistent patterns of inattention, hyperactivity, and impulsivity that interfere with daily functioning and development 12. While historically viewed strictly as a childhood behavioral issue, modern clinical consensus recognizes that ADHD frequently persists across the lifespan. Today, an estimated 6 to 9 percent of all school-age children and roughly 15.5 million adults in the United States currently live with an ADHD diagnosis 3.
For decades, the pharmacological management of ADHD has been dominated by central nervous system stimulants, primarily methylphenidate (e.g., Ritalin, Concerta) and amphetamine derivatives (e.g., Adderall, Vyvanse). The dominance of these drugs is immense; according to 2022 DEA data, 90 percent of ADHD prescriptions were for stimulants, while only 10 percent were for non-stimulants 4. When effectively prescribed, stimulant medications are highly efficacious, yielding large effect sizes and rapid, same-day symptom relief 45.
However, the dominance of stimulants has created significant bottlenecks and risks in patient care, spurring a pharmaceutical race to develop viable alternatives.
The Limitations of Stimulant Therapies
Despite their proven efficacy, up to 30 percent of patients either do not respond adequately to stimulant medications or simply cannot tolerate their physiological side effects 56.
Stimulants are classified by the U.S. Drug Enforcement Administration (DEA) as Schedule II controlled substances. This classification indicates a drug with a high potential for abuse, dependency, and diversion, carrying strict federal prescribing limitations and black-box warnings 78.
The clinical and systemic drawbacks of stimulants include: * Adverse physiological effects: Stimulants are routinely associated with severe appetite suppression, insomnia, mood lability, and cardiovascular risks, including elevated heart rate and blood pressure 79. * Psychiatric risks: In rare cases, stimulants can trigger the emergence of manic or psychotic symptoms in patients with no prior psychiatric history 7. * Supply chain vulnerabilities: Between 2022 and 2025, the U.S. experienced severe, prolonged shortages of generic and brand-name stimulant medications. This crisis left millions of patients without consistent access to their prescribed treatments, forcing many to abruptly switch medications or go without care 10.
The Role of Existing Non-Stimulants
To address patients who are averse to stimulants, have a history of substance use disorder, or have comorbid conditions that contraindicate stimulant use, clinicians turn to non-stimulant medications.
Prior to 2026, the FDA-approved non-stimulant landscape consisted primarily of four medications: atomoxetine (Strattera), viloxazine extended-release (Qelbree), guanfacine (Intuniv), and clonidine (Kapvay, Onyda XR) 610. The newest of these, Onyda XR (a liquid oral suspension of clonidine), was approved in May 2024 specifically for pediatric patients 6.
While these options lack the abuse liability of stimulants and are not scheduled as controlled substances, they come with their own trade-offs. Atomoxetine and viloxazine generally exhibit lower clinical effect sizes (approximately 0.7) compared to stimulants 11. Furthermore, they require a longer period of consistent, daily dosing - often taking anywhere from one to six weeks before patients experience peak therapeutic benefits 5911.
This landscape leaves a distinct gap in the market: a pressing need for a non-stimulant medication that bridges the gap between the robust efficacy of stimulants and the superior safety profile of existing non-stimulants. This is the precise clinical void that Otsuka Pharmaceutical's centanafadine aims to fill 112.
What Is Centanafadine? Understanding the NDSRI Mechanism
To understand why centanafadine represents a novel approach to ADHD treatment, it is necessary to examine its unique pharmacological mechanism.
Current medications typically target one or two neurotransmitter systems. Stimulants primarily flood the brain's synapses with dopamine and norepinephrine. Existing non-stimulants like atomoxetine and viloxazine act primarily as selective norepinephrine reuptake inhibitors (SNRIs), meaning they selectively block the reabsorption of norepinephrine to increase its availability in the brain, with atomoxetine having only a very weak secondary effect on serotonin 59.
Centanafadine introduces an entirely new drug class to the ADHD armamentarium: it is a norepinephrine, dopamine, and serotonin reuptake inhibitor (NDSRI) 127. Also referred to in the clinical literature as a "triple-monoamine reuptake inhibitor," centanafadine works by blocking the transport pumps responsible for clearing these three vital chemicals from the synaptic cleft between neurons 210.
At the cellular level, neurotransmitters are released from a presynaptic neuron into the synaptic cleft, where they bind to receptors on a postsynaptic neuron to pass along a signal. Normally, reuptake transporters (NET for norepinephrine, DAT for dopamine, and SERT for serotonin) act like vacuums, quickly reabsorbing these chemicals to end the signal. Centanafadine physically blocks these three specific transporters. By doing so, it allows dopamine, norepinephrine, and serotonin to linger in the synaptic cleft for longer periods, continuously stimulating the receiving neuron and regulating attention, motivation, and emotional control 210.
The Role of Each Neurotransmitter
By modulating all three pathways simultaneously, centanafadine is designed to target the multifaceted nature of ADHD symptoms: 1. Norepinephrine: This neurotransmitter is critical for maintaining alertness, sustaining attention over time, and executing complex cognitive functions. Research suggests norepinephrine levels are often depleted in individuals with ADHD 29. 2. Dopamine: Essential for motivation, reward-processing, and the ability to initiate and focus on unstimulating tasks. Traditional stimulants rely heavily on dopamine modulation 2. 3. Serotonin: This chemical regulates mood, impulse control, and emotional reactivity. By purposefully introducing a strong serotonergic component, centanafadine aims to address associated behavioral features of ADHD that are frequently overlooked by traditional dual-action treatments 2.
Beyond Focus: Executive Function and Emotional Dysregulation
The addition of deliberate serotonin modulation is particularly notable in clinical psychiatry. While the core diagnostic criteria for ADHD outlined in the DSM-5 strictly involve metrics of inattention, hyperactivity, and impulsivity, real-world patients frequently struggle with profound emotional dysregulation and severe deficits in executive functioning 13. Executive functioning refers to the brain's management system - the ability to plan, organize, manage time, and execute multi-step tasks.
In exploratory, post-hoc analyses of Phase 3 adult trials presented at the 2026 American Society of Clinical Psychopharmacology (ASCP) Annual Meeting, centanafadine was shown to significantly improve both patient-reported executive functioning and emotional control 13.
The analysis included 744 adults assessed using the Adult ADHD Self-Report Scale (ASRS) Expanded Version. At week six, patients treated with centanafadine reported measurable reductions in the frequency of executive functioning difficulties compared to a placebo group 13. Furthermore, the drug was associated with improved emotional dysregulation, including distinct reductions in emotional overactivity, affective lability (severe mood swings), and sudden anger outbursts 13.
For many adults navigating the professional and interpersonal complexities of daily life, addressing these associated emotional and organizational features is just as critical to their quality of life as improving raw, momentary focus 13.
Clinical Trial Evidence: Pediatric and Adolescent Populations
The New Drug Application (NDA) submitted by Otsuka Pharmaceuticals is heavily supported by a robust clinical program comprising four pivotal Phase 3 randomized, double-blind, placebo-controlled trials 13. Notably, the drug's manufacturer conducted simultaneous, widespread testing across the entire lifespan - children, adolescents, and adults - providing a comprehensive view of the drug's efficacy 1415.
In pediatric and adolescent populations, efficacy was primarily measured using the ADHD Rating Scale-5 (ADHD-RS-5), a validated clinical tool for assessing symptom severity 1.
The Pediatric Trial (Ages 6 to 12)
In a six-week Phase 3 trial involving 480 children with a primary diagnosis of ADHD, patients were randomized to receive a weight-based low dose of centanafadine, a weight-based high dose, or a placebo 16.
By the end of the trial, children receiving the high dose demonstrated a statistically significant improvement in their ADHD-RS-5 total raw scores compared to those on a placebo. The high-dose group saw a 16.3-point reduction in symptom scores, compared to a 10.8-point reduction in the placebo group 16.
Importantly, the high-dose group showed a measurable separation from the placebo group as early as week one, suggesting a relatively rapid onset of action for a non-stimulant 16. However, the low-dose cohort failed to reach statistical significance regarding the primary efficacy endpoint, indicating that appropriate dosing is critical for pediatric success 1416.
The Adolescent Trial (Ages 13 to 17)
Similar results were observed in the adolescent trial, which enrolled 459 participants. Adolescents were randomly assigned to a low fixed dose (164.4 mg), a high fixed dose (328.8 mg), or a placebo 1718.
Adolescents treated with the higher 328.8 mg daily dose achieved a significantly greater reduction in symptoms compared to the placebo group, with an 18.50-point drop on the ADHD-RS-5 scale versus a 14.15-point drop for placebo 1718. As with the younger cohort, the medication demonstrated separation from placebo at week one. Once again, the lower 164.4 mg dose failed to meet the primary clinical endpoint, establishing the necessity of the higher dosage for clear clinical efficacy in youth 1718.
Clinical Trial Evidence: Adult Populations
In the adult population (aged 18 to 55 years), centanafadine was evaluated across two identically designed Phase 3 trials (Study 1 and Study 2) using the Adult ADHD Investigator Symptom Rating Scale (AISRS). Participants in these trials generally presented with moderate to severe ADHD, holding a mean baseline AISRS total score of 38.7 1920.
Unlike the pediatric trials where only the highest doses proved effective, adults responded positively to both investigated doses. Participants receiving either 200 mg/day or 400 mg/day (administered as sustained-release tablets taken twice daily) demonstrated statistically significant and clinically meaningful reductions in ADHD symptoms compared to a placebo over the 42-day study period 1920.
The effect sizes generated in these adult trials ranged from -0.24 to -0.40 against placebo. While these figures are moderate, they place centanafadine firmly within the efficacy range expected of modern non-stimulant ADHD therapies 1921. Furthermore, both dose groups achieved their key secondary endpoints, showing significant improvements on the Clinical Global Impression - Severity of Illness Scale (CGI-S), a metric used by physicians to judge a patient's overall functional improvement 1920.
Summary of Centanafadine Phase 3 Clinical Trials
| Target Demographic | Trial Duration | Primary Efficacy Scale | Dosages Evaluated | Key Efficacy Findings |
|---|---|---|---|---|
| Children (Ages 6-12) | 6 Weeks | ADHD-RS-5 | Weight-based High vs. Low | High dose: Significant improvement (-16.3 points). Low dose: Not significant. 16 |
| Adolescents (Ages 13-17) | 6 Weeks | ADHD-RS-5 | 328.8 mg vs. 164.4 mg | High dose: Significant improvement (-18.5 points). Low dose: Not significant. 1718 |
| Adults (Ages 18-55) | 6 Weeks | AISRS | 400 mg/day vs. 200 mg/day | Both doses: Significant improvement. Effect sizes of -0.24 to -0.40. 1920 |
Comparing Centanafadine to Existing Medications
Because centanafadine is an investigational drug, there are currently no completed head-to-head clinical trials directly comparing it to other ADHD medications on the market. In the absence of direct trials, researchers utilize a rigorous statistical technique known as a Matching-Adjusted Indirect Comparison (MAIC) to help clinicians understand where a new drug fits into the treatment landscape 2223.
An MAIC pools patient-level data from the new drug's trials and matches it mathematically to aggregate data from published trials of competing drugs. By using propensity score weighting, researchers adjust for baseline patient characteristics - such as age, sex, and starting symptom severity - to create a fair, simulated comparison across different studies 222324.
A comprehensive MAIC published in the Journal of Managed Care & Specialty Pharmacy compared centanafadine against three dominant ADHD treatments for adults: lisdexamfetamine (Vyvanse, a stimulant), atomoxetine (Strattera, a non-stimulant), and viloxazine ER (Qelbree, a non-stimulant) 222325.
Efficacy Comparisons
The indirect comparison revealed that centanafadine is less effective at reducing core ADHD symptoms than the stimulant lisdexamfetamine. Patients taking lisdexamfetamine experienced a 6.58-point greater reduction on the AISRS symptom scale than those on centanafadine 222326. This finding aligns with broader medical consensus: Schedule II stimulants remain the most potent pharmacological agents for raw symptom control 45.
However, when compared to its true peers - the existing non-stimulants - centanafadine held its ground. The MAIC showed no statistically significant difference in efficacy (symptom reduction) between centanafadine and either atomoxetine or viloxazine ER 2223.
Safety and Tolerability Advantages
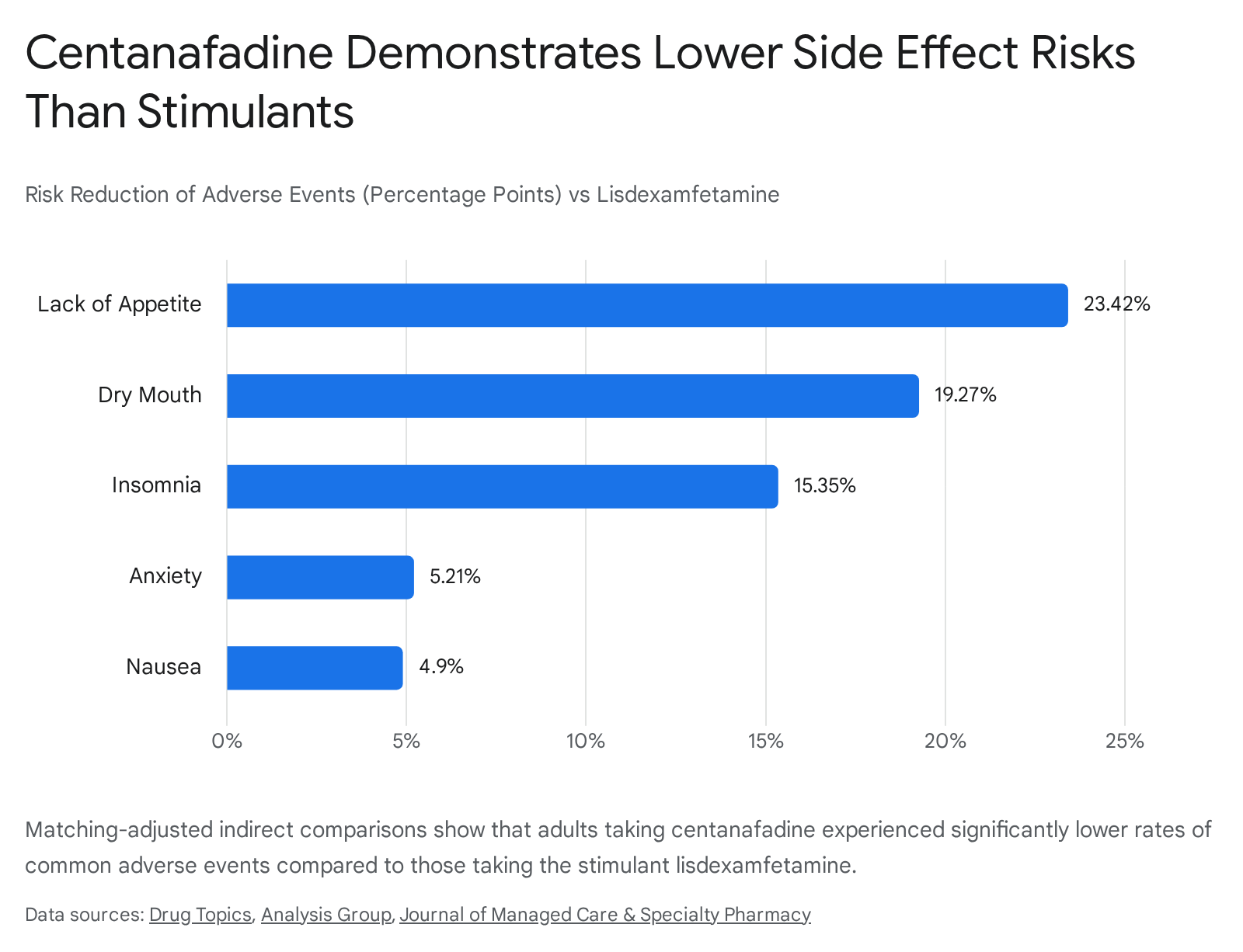
While centanafadine may not beat stimulants on pure efficacy, it demonstrated a profound advantage in its safety and tolerability profile. The MAIC study highlights that the primary clinical utility of centanafadine will likely lie in its ability to offer symptom control with a vastly reduced side-effect burden.
When matched against the stimulant lisdexamfetamine, patients on centanafadine had a substantially better experience regarding treatment-emergent adverse events. Specifically, centanafadine users had a 23.4 percentage-point lower risk of appetite loss, a 19.2 percentage-point lower risk of dry mouth, and a 15.3 percentage-point lower risk of insomnia 2223.
Even when compared to competing non-stimulants, centanafadine appeared notably more tolerable. Compared to atomoxetine, centanafadine users experienced significantly lower risks of nausea (-18.6 percentage points), dry mouth (-17.4 percentage points), and fatigue (-9.2 percentage points) 23. Against viloxazine ER, centanafadine was associated with lower risks of fatigue (-11.0 percentage points) and insomnia (-10.6 percentage points) 2325.
The table below synthesizes the findings of the matching-adjusted indirect comparison across both efficacy and safety domains.
| Medication Type | Drug Name | Efficacy vs. Centanafadine | Safety/Tolerability vs. Centanafadine |
|---|---|---|---|
| Stimulant | Lisdexamfetamine (Vyvanse) | Superior (6.58 point greater reduction) | Inferior (Higher risk of insomnia, dry mouth, appetite loss) |
| Non-Stimulant | Atomoxetine (Strattera) | Comparable (No significant difference) | Inferior (Higher risk of nausea, dry mouth, fatigue) |
| Non-Stimulant | Viloxazine ER (Qelbree) | Comparable (No significant difference) | Inferior (Higher risk of fatigue, insomnia, nausea) |
Note: Data derived from anchored Matching-Adjusted Indirect Comparisons 22232425. Head-to-head clinical trial data remains unavailable.
Across its own Phase 3 trials, the most common adverse events reported by children and adolescents taking centanafadine included mild to moderate abdominal pain, decreased appetite, fatigue, nausea, rash, and somnolence (drowsiness) 2927. In adults, the most frequently reported issues were simply headache and decreased appetite 1029. Crucially, there was no evidence of symptom rebound or acute discontinuation syndrome when patients stopped taking the medication 11.
Abuse Potential and DEA Scheduling Expectations
One of the primary driving forces behind the development of novel non-stimulant medications is the necessity of mitigating the abuse and diversion risks inherent to amphetamines and methylphenidate. Stimulants carry bolded, boxed warnings from the FDA regarding their high potential for addiction 47.
Throughout its clinical development program, centanafadine has consistently demonstrated a favorable safety profile with a remarkably low potential for abuse or dependency 12282930. In early exploratory human abuse liability studies, participants given immediate-release formulations of centanafadine showed drug-liking scores that suggest the liability is significantly less than that of traditional stimulants 621.
Because of this lack of euphoric effect, industry analysts and clinical experts widely expect that, if approved by the FDA, centanafadine will either remain entirely unscheduled (similar to Strattera and Qelbree) or be placed into a much lower restrictive tier (e.g., Schedule IV) by the DEA 61030.
For both patients and prescribers, a non-controlled or lower-schedule classification is a major logistical advantage. It vastly simplifies the prescribing process, removes strict monthly refill limitations that require constant doctor visits, allows for easier telehealth prescribing, and eliminates the stigma and regulatory anxiety often associated with Schedule II drugs 10.
Regulatory Status and the Global Timeline to Market
The global market for ADHD drugs is massive and growing. Driven by rising diagnosis rates across pediatric and adult populations, the global Adderall and ADHD drug market was valued at $21.74 billion in 2025 and is projected to expand to $32.18 billion by 2035 34. The entry of new non-stimulant candidates like centanafadine signals increasing manufacturer investment in next-generation pharmacotherapy aimed at this lucrative market 34.
The regulatory journey for centanafadine in the United States is currently in its final stages. Otsuka Pharmaceutical initially submitted the New Drug Application (NDA) to the FDA on November 24, 2025 1429.
On January 27, 2026, the FDA formally accepted the NDA and granted it Priority Review status 13. Priority Review is a highly coveted designation granted only to investigational drugs that the FDA believes would provide a significant improvement in the safety or effectiveness of the treatment, diagnosis, or prevention of a serious condition 1. This designation shortens the FDA's standard review timeline from ten months to six months, signaling that federal regulators view the ongoing ADHD medication shortage and the side-effect burden of existing therapies as an unmet medical need 131.
The FDA has set a Prescription Drug User Fee Act (PDUFA) target action date of July 24, 2026 1330. On or before this date, the FDA will announce whether centanafadine is officially approved for commercial sale in the United States.
International Review: Europe and Japan
While the U.S. FDA is nearing a decision, global regulatory bodies are also evaluating the drug. In Japan, the Pharmaceuticals and Medical Devices Agency (PMDA) has been working to promote pediatric drug development through an "All-Japan approach" 32. To facilitate faster access to new therapies, the PMDA now allows Japan to participate in global pediatric trials planned in Europe and the U.S. even before clinical trials in Japanese adults have commenced 32. Centanafadine is part of these global pediatric evaluations, though a formal NDA timeline for Japan has not been finalized 3237.
In Europe, the European Medicines Agency (EMA) and its Committee for Medicinal Products for Human Use (CHMP) publish monthly lists of medicines under evaluation. While Otsuka maintains a global presence, as of mid-2026, specific EMA approval dates for centanafadine's European market entry remain pending as the agency works through its 2026 regulatory pipeline 33.
The Path to the Pharmacy: Prior Authorizations
If the FDA grants approval in July 2026, patients will not necessarily be able to pick up the medication the very next day.
First, if the DEA decides to evaluate the drug for any level of controlled scheduling, that administrative process can delay the drug's physical arrival in pharmacies by several weeks or months following FDA clearance.
Second, as a newly approved, branded medication, centanafadine will inevitably face friction from insurance companies. Health insurers typically employ "prior authorization" protocols for expensive new drugs to prevent unnecessary spending. This requires doctors to prove that a patient has a medical necessity for the brand-name drug - often requiring proof that the patient has already tried and failed cheaper, generic alternatives (like generic atomoxetine or generic stimulants) before the insurer will cover the cost 3940.
Navigating prior authorizations for newly approved specialty or branded medications routinely takes between 7 to 14 business days, and complex appeals or peer-to-peer physician reviews can extend the wait to 30 days or more 404142. Therefore, while the clinical availability is slated for the second half of 2026, widespread, frictionless access may take longer to materialize as insurance formularies update and clinics adapt to the prior authorization requirements 3940.
Bottom line
If approved in July 2026, centanafadine will represent the first new class of ADHD medication (an NDSRI) to enter the market in years, offering a triple-neurotransmitter approach that addresses both core focus deficits and associated emotional dysregulation. While indirect comparisons suggest it is not as potent as traditional stimulants for raw symptom control, it offers a vastly superior safety profile and promises to reduce the severe appetite suppression, insomnia, and abuse risks that currently complicate ADHD care. What remains to be seen is exactly how the DEA will schedule the drug post-approval, and how quickly insurance companies will allow patients to access it through prior authorization channels.