Why Your Metabolism Fights Back When You Lose Weight
When you lose weight, your body perceives the loss of stored energy as a severe biological threat and initiates a sophisticated survival response. It actively lowers your resting metabolic rate and alters your hunger hormones to conserve energy and compel you to eat, a phenomenon known as adaptive thermogenesis. While this evolutionary defense mechanism makes continued weight loss and long-term maintenance remarkably difficult, modern clinical research proves it is a reversible adaptation, not a permanent breaking of your metabolism.
The Baseline: Understanding How Your Body Burns Energy
To comprehend why the body resists weight reduction, it is necessary to first understand how it expends energy on a daily basis. The total amount of energy your body requires over twenty-four hours is known as your Total Daily Energy Expenditure (TDEE) 11. For decades, the public has been told that mastering this equation is a simple matter of "calories in, calories out." While the fundamental laws of thermodynamics absolutely apply, the "calories out" side of the equation is vastly more complex and dynamic than a simple math problem 342.
Total Daily Energy Expenditure is not a single number, but rather a dashboard of interconnected systems divided into several core components:
- Resting Metabolic Rate (RMR): Often used interchangeably with Basal Metabolic Rate (BMR), this is the sheer baseline energy your body requires to simply stay alive. It accounts for the calories needed to keep your heart beating, lungs breathing, blood circulating, and cells repairing while completely at rest 67. For the average adult, RMR is the dominant factor in daily energy burn, fulfilling roughly 60% to 70% of total energy expenditure 63.
- Non-Exercise Activity Thermogenesis (NEAT): This component encompasses all the energy expended through subconscious, unintentional movements. It includes maintaining posture, pacing while talking on the phone, fidgeting, and routine daily chores 69.
- Thermic Effect of Food (TEF): The energy your body expends to digest, absorb, and metabolize the nutrients in the food you consume. This generally accounts for about 10% to 15% of your daily energy output 14.
- Exercise Activity Thermogenesis (EAT): The calories burned during intentional, structured physical workouts, such as running, cycling, or lifting weights. Surprisingly, for most non-athletes, this accounts for the smallest fraction of total daily energy expenditure 67.
Because testing resting metabolic rate in a clinical setting via indirect calorimetry - which measures the exact amount of oxygen your body uses at rest - is not available to everyone, scientists historically developed predictive models 7. Standard equations, such as the Harris-Benedict formula, attempt to estimate a person's baseline burn using height, weight, age, and sex 3. However, these equations often fail to account for the dramatic biological shifts that occur the moment a person begins to alter their food intake.
The Constrained Energy Model
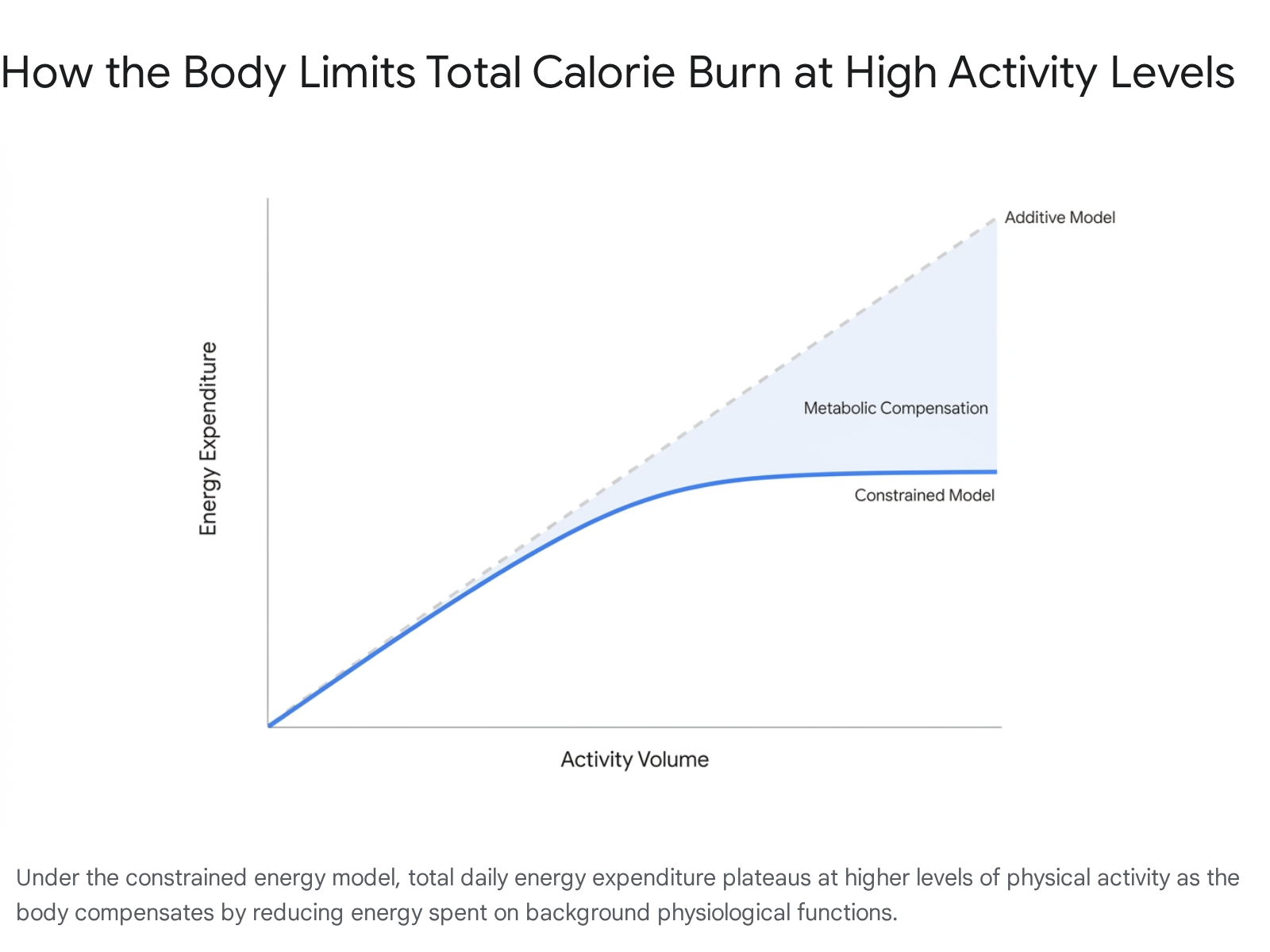
For a long time, exercise and weight loss were viewed through an "additive" lens. The additive model suggested that the human metabolism operated like a simple bank account: if you burned 2,000 calories resting, and then went for a run and burned 500 calories, your total daily energy expenditure would be 2,500 calories 134. Under this model, moving more inherently guaranteed burning more.
This long-held assumption was fundamentally disrupted by evolutionary anthropologist Herman Pontzer. Pontzer and his colleagues conducted a landmark study on the Hadza, a highly active hunter-gatherer population in Tanzania 411. The Hadza walk for miles every day to hunt and forage. Under the additive model, they should burn significantly more calories than sedentary Westerners.
However, Pontzer discovered that once adjusted for body size and composition, the physically active Hadza burned roughly the exact same number of calories per day as sedentary office workers in the United States and Europe 411. Similar findings were later noted in other active populations, though some groups, like the Tsimane of Bolivia, show slightly higher expenditures due to the high metabolic cost of fighting frequent parasitic infections 11.
This research gave rise to the Constrained Energy Expenditure Model. The constrained model posits that the human body has a relatively fixed ceiling on total daily energy expenditure. When physical activity increases significantly, the body does not simply add those burned calories to the daily total indefinitely. Instead, it compensates by quietly down-regulating non-activity energy expenditure to keep the total within a narrow, heavily regulated band 145.
| Model Type | Core Mechanism | Effect of Increased Exercise | Physiological Reality |
|---|---|---|---|
| Additive Model | Energy expenditure functions in a strictly linear fashion. | Total daily calories burned increases directly by the exact amount of exercise calories burned. | Highly simplistic. Only applies to the transition from complete sedentary behavior to light activity 345. |
| Constrained Model | The body maintains a tightly regulated daily energy budget. | Total daily calories burned plateaus; the body compensates by reducing background metabolic functions. | The body limits energy spent on resting metabolism, systemic inflammation, and minor movements to afford the exercise 14. |
Subsequent studies have confirmed this phenomenon in modern populations. In 2021, a study of 1,754 adults found that energy compensation averaged 28%. In other words, if an individual added 500 calories of physical activity to their day, their actual daily energy expenditure only rose by roughly 360 calories, because the body compensated for the other 140 calories by slowing down other functions 1. Interestingly, leaner individuals compensated less (around 29.7%), while individuals carrying more body fat were stronger energy compensators, neutralizing up to 45.7% of the calories burned through activity 1.
This is why, as Pontzer notes, exercise alone has a notably poor track record as an isolated weight-loss method 311. It is critical for cardiovascular health, longevity, and muscle preservation, but the body simply will not allow you to run away from a high-calorie diet.
The Battery Saver Mode of Human Biology
When you introduce a caloric deficit - either by eating less or attempting to drastically out-train your diet - your body does not passively burn away its fat reserves. It actively defends them.
A useful analogy is the battery saver mode on a smartphone. When a phone's battery drops to a critical level, the device does not simply shut down. Instead, the operating system intervenes to stretch out every last drop of power. It dims the screen brightness, reduces the processing speed of the CPU, delays background app notifications, and stops auto-syncing data 13146. The phone still functions, but it is intentionally sluggish to prevent sudden death 1314.
Your biological systems perform an almost identical triage. When energy intake drops, your brain's hypothalamus senses a fuel shortage. It essentially puts your body into "low power mode." Your resting metabolic rate drops. Cellular operations, such as mitochondrial proton leak and resting myosin ATP consumption in your skeletal muscles, become highly efficient, doing the same work for less energy 7. Your subconscious movements plummet; you stop fidgeting, your posture slumps slightly, and you opt for the elevator instead of the stairs without even realizing it 329.
This means that as a diet progresses, the very deficit you created begins to shrink, not because you are eating more, but because your body is systematically refusing to burn as much energy 8910.
The Hypothalamus and Your "Weight Thermostat"
The regulation of body weight is not governed by willpower; it is governed by a physiologic set point. You can think of this set point like a thermostat in a house 42.
If you set your home thermostat to 70 degrees Fahrenheit and open a window on a freezing winter day, the ambient temperature inside the house drops. However, the thermostat immediately detects this drop and kicks the furnace into high gear to drive the temperature back up to 70 degrees 4.
Similarly, obesity and weight regulation are deeply tied to this metabolic thermostat. The human body aims to maintain its current weight, protecting its fat stores against the threat of starvation - an evolutionary imperative critical for surviving ancient famines 11920. When you restrict calories, your brain interprets the drop in energy not as a desired physical transformation, but as an environmental danger 22021. It lowers the furnace (your metabolism) and ramps up the drive to find fuel (your hunger).
The Hormonal Symphony
The brain does not monitor fat stores via a single neural wire. It relies on a complex, continuous symphony of chemical messengers flowing from the gut, pancreas, and fat cells through the brain-gut axis 811.
| Hormone | Primary Source | Function and Response to Weight Loss |
|---|---|---|
| Leptin | Fat Cells (Adipose Tissue) | The master fuel gauge. Discovered in 1994, leptin scales with fat mass. It signals the brain that energy stores are full, suppressing appetite. During weight loss, leptin levels plummet, which the brain interprets as a starvation crisis, violently ramping up hunger 2111213. |
| Ghrelin | Stomach | The primary "hunger hormone." It initiates feeding and regulates meal frequency. During a diet, ghrelin levels rise by 18% to 25%, making you persistently food-focused 9101112. |
| GLP-1 | Intestines (L-cells) | Released after eating, glucagon-like peptide-1 slows stomach emptying, stimulates insulin, and signals fullness to the brain 81214. |
| Peptide YY (PYY) | Intestines | Works alongside GLP-1 to induce satiety and meal termination. Levels of PYY decrease during weight loss, meaning you feel less satisfied after a meal 101112. |
| Cholecystokinin (CCK) | Duodenum (Small Intestine) | Secreted in the presence of fats and proteins, CCK is a rapid-response satiety signal with a short half-life of one to two minutes 1112. |
| Insulin | Pancreas | Regulates glucose storage. Levels drop during weight loss, which facilitates fat burning but also serves as an alarm bell to the brain regarding low energy availability 21215. |
When you lose body fat, this entire hormonal profile shifts against you. The drop in leptin is perhaps the most devastating. Many people living with obesity have high levels of leptin but suffer from "leptin resistance" - inflammation or other factors prevent the brain from hearing the signal, so the brain believes the body is starving even when heavily overweight 2.
When the diet begins, the little leptin signal that was getting through diminishes further. The "door" is sticky, and the knocking stops 2. Simultaneously, ghrelin surges. This hormonal assault explains why long-term dieters report constant food focus, irritability, and an intense drive to eat 2920.
Adaptive Thermogenesis: The Body's Defense
When you successfully lose weight, your daily energy expenditure will inevitably drop simply because a smaller body requires less energy to operate. A 150-pound individual requires less mechanical effort to walk up a hill than a 200-pound individual 9. This mechanical reduction is entirely normal.
However, metabolic adaptation - specifically referred to in the literature as adaptive thermogenesis - occurs when the decline in energy expenditure is significantly greater than what would be predicted by the loss of body mass alone 981327.
During severe caloric restriction, the body becomes ruthlessly efficient. Studies have shown that resting metabolic rate can drop between 50 to 180 kcal per day beyond predicted mechanical expectations, representing roughly a 5% to 15% deeper adaptation 16. In extreme cases involving massive caloric deficits and grueling physical activity, the adaptation is staggering.
The reality television show The Biggest Loser provided a grim but fascinating dataset for obesity researchers. Contestants underwent extreme starvation dieting paired with hours of daily exercise, losing massive amounts of weight (often over 70 kilograms) 11. Years later, researchers found their metabolisms had gone into a severe conservation mode. Six years after the competition, their resting metabolic rates remained approximately 500 kcal per day lower than expected for their new body sizes 1718. Unsurprisingly, almost all of them regained the weight 11.
The Timeline of Metabolic Slowdown
Metabolic adaptation does not wait until you have reached your goal weight to deploy; it is an aggressive and early responder.
Researchers analyzing the exact timeline of adaptation have found that adaptive thermogenesis can be detected as early as one week into a severe caloric restriction 1319. * Week 1 to 3: A significant drop in resting energy expenditure occurs, initially tied to the rapid depletion of glycogen stores, drops in total body water, and the early suppression of thyroid hormone (T3) conversion 131732. One study restricting subjects to 50% of their maintenance calories found an adaptive drop of 178 kcal per day within the first seven days. This early drop predicted that these subjects would lose 2 kg less weight over a six-week period than math would suggest 1332. * Weeks 8 to 12: As weight loss approaches 10% of total body mass, exercise-induced energy expenditure also becomes more efficient. You burn fewer calories doing the exact same workout you did months prior 19. Hormonally, the reductions in sympathetic nervous system activity and circulating leptin solidify the adaptation 13.
Does Adaptation Actually Cause Weight Regain?
Because adaptive thermogenesis is so widely publicized, it is often treated as the sole villain responsible for the "yo-yo dieting" effect, where individuals rapidly regain all the weight they lost. However, modern scientific literature provides a highly nuanced correction to this belief.
Dr. Cátia Martins, a leading researcher at the University of Alabama at Birmingham, has spent a decade investigating the mechanisms of metabolic adaptation. Her extensive clinical trials indicate a surprising truth: while adaptive thermogenesis is real, there is no strong, undeniable link between metabolic adaptation and long-term weight regain 2021.
What her research actually proves is that a heavily adapted metabolism increases the time required to hit a weight loss goal. Individuals who experience severe metabolic adaptation lose less fat mass in response to a low-energy diet than those who do not adapt as strongly, making the diet process frustratingly slow and grueling 2021.
However, when subjects finally transition to a weight maintenance phase and stop the caloric deficit, the adaptation largely subsides. The gap between measured and predicted resting metabolic rate shrinks dramatically (often to a negligible 50 kcal/day difference) once weight stabilizes 20. The primary driver of weight regain is not a broken metabolic rate, but the intense, persistent surge in appetite caused by the hormonal shifts 21. The body makes you intensely hungry; if you succumb to that hunger and overeat, the weight returns.
Rapid vs. Slow Weight Loss: Which Is Better?
A pervasive myth in nutrition spaces dictates that you must lose weight slowly (no more than 1 to 2 pounds per week) to protect your metabolism, and that rapid weight loss inevitably destroys your resting metabolic rate 635. The clinical data tells a more complex story.
When researchers review broad demographic data, they generally find that people who lose weight rapidly without specific interventions experience a greater decline in their resting metabolic rate compared to those who lose weight gradually 622. A meta-analysis comparing gradual weight loss against rapid weight loss showed that while total pounds lost were often similar, gradual loss resulted in superior reductions in fat mass and better preserved the resting metabolic rate (sparing an average of 407 kilojoules) 22.
The primary reason rapid weight loss often harms the metabolism is due to the loss of fat-free mass (muscle tissue). Standard, unmonitored calorie restriction can cause 20% to 30% of the lost weight to come from muscle 9. Because muscle is highly metabolically active tissue, sacrificing it during a crash diet significantly lowers your daily energy burn 637.
However, this negative outcome is not entirely due to the speed of the loss, but rather the method. When rapid weight loss is supported by adequate protein intake and intense resistance training, the loss of muscle mass is drastically minimized 6.
| Factor | Slow / Gradual Weight Loss | Rapid Weight Loss |
|---|---|---|
| Typical Duration / Target | ~0.5 kg to 1 kg per week (e.g., 15 weeks for 5% loss) 623. | >1.0 kg per week (e.g., 5 weeks for 5% loss) 623. |
| Muscle Preservation | Generally better preservation of fat-free mass in general populations 2223. | Higher risk of muscle atrophy if protein and resistance training are ignored 623. |
| Metabolic Adaptation | Smaller adaptive drops in resting metabolic rate 623. | Larger initial drops in resting metabolic rate during the active diet phase 623. |
| Metabolic Health Markers | Improves insulin sensitivity and lipid profiles 23. | Often yields significantly faster improvements in fasting blood sugar and lipid profiles 23. |
Recent robust clinical trials are even challenging the psychological dogma that rapid weight loss leads to rapid regain. At the 2026 European Congress on Obesity, researchers presented a 52-week randomized clinical trial involving 284 adults with obesity 35. One group utilized a rapid weight-loss protocol starting under 1,000 calories a day, while the gradual group consumed roughly 1,400 calories.
At the end of the initial 16-week phase, the rapid group lost nearly 13% of their body weight, compared to just 8% in the gradual group. Crucially, a year later, the rapid weight-loss group had maintained significantly greater weight loss and hit superior clinical targets for reducing the risk of type 2 diabetes and hypertension 35. As lead researcher Line Kristin Johnson noted, these findings directly challenge the prevailing belief that slow and steady is strictly necessary to prevent weight regain 35.
Can You Fix or Prevent Metabolic Adaptation?
The fitness industry is rife with strategies promising to "repair" or "boost" a broken metabolism. Most of these claims lack rigorous scientific backing.
For instance, eating frequent, small meals throughout the day does not boost fat oxidation or significantly elevate the thermic effect of food; in fact, clinical trials show it can actually increase feelings of hunger compared to eating three standard meals 37. Similarly, while supplements containing green tea or capsaicin (chili peppers) show minor metabolic interactions, the effects are clinically negligible - often requiring absurd doses (like a cup of coffee every two hours) to achieve a transient 11% boost, which is neither healthy nor sustainable 3724.
Furthermore, you cannot blame the natural aging process for a sudden metabolic halt. A comprehensive 2021 study utilizing global doubly labeled water data revealed that adult human metabolism remains incredibly stable from age 20 all the way to age 60, regardless of sex or life events like pregnancy 1. The "middle-age spread" is overwhelmingly driven by subtle lifestyle changes, increased stress, and creeping inactivity, rather than a failing biological furnace 11024.
If the metabolism is not broken, how do we handle adaptive thermogenesis? Clinical science points to strategic nutritional adjustments.
The Efficacy of Diet Breaks
Because continuous caloric restriction triggers a decline in leptin and thyroid hormones within 8 to 12 weeks, taking structured breaks from dieting has emerged as a highly effective intervention 9.
This was rigorously tested in the MATADOR (Minimising Adaptive Thermogenesis And Deactivating Obesity Rebound) study 254226. Researchers assigned men with obesity to one of two protocols: 1. Continuous Group: Maintained a 33% caloric deficit for 16 consecutive weeks. 2. Intermittent Group: Dieted at the same 33% deficit for two weeks, followed by two weeks of eating at maintenance calories. This cycle repeated for a total of 30 weeks (achieving the same 16 weeks of actual dieting).
The intermittent group achieved vastly superior results. They lost an average of 14.1 kg compared to the continuous group's 9.1 kg, and specifically lost more fat mass 4226.
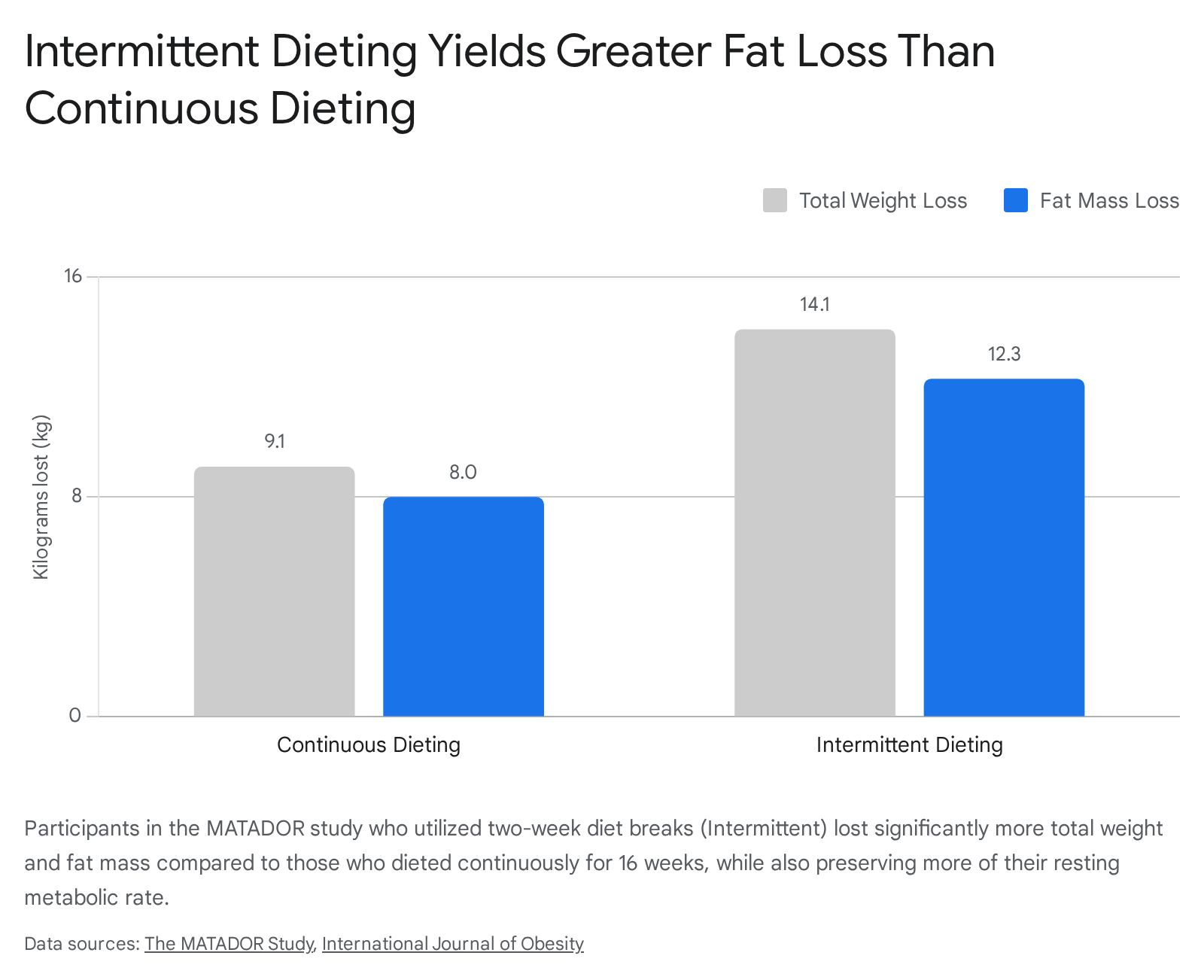
Most importantly, after adjusting for body composition changes, the intermittent group suffered significantly less reduction in their resting energy expenditure 4226. By routinely introducing periods of maintenance eating, the body perceived an environment of abundance, preventing the hypothalamus from fully engaging its starvation protocols.
The Truth About Reverse Dieting
In recent years, "reverse dieting" has gained massive popularity in fitness communities. The protocol dictates that after finishing a diet, an individual should add a microscopic amount of calories back to their diet each week (e.g., 50 to 100 kcal) 1718. Advocates claim this slowly "stokes the metabolic fire," allowing the resting metabolic rate to recover without the body storing the incoming energy as fat.
While it sounds logically appealing, human clinical trials do not support the physiological hype. A recent randomized controlled trial compared a strict reverse dieting approach (adding back a small percentage of calories weekly) to a control group that simply ate ad libitum (to fullness), and another that jumped straight back to estimated maintenance calories 27.
The results showed no statistically significant difference in weight regain or weight gain efficiency between the groups 27. In fact, the reverse dieting group actually trended toward greater relative weight regain, though it fell short of statistical significance 27.
As researchers like Eric Trexler note, the benefits of reverse dieting are largely psychological 18. It forces hyper-compliance and prevents the post-diet binging that derails many weight-loss attempts. Physiologically, however, attempting to "trick" the metabolism by tiptoeing up the caloric ladder is unnecessary. Because metabolic adaptation is a direct response to an energy deficit, the most effective way to eliminate the adaptation is simply to erase the deficit 1845. Experts increasingly recommend "dynamic maintenance" - calculating your new estimated maintenance calories and transitioning immediately to that level, making small adjustments based on how scale weight responds 18.
The Role of Modern Obesity Medications
The profound difficulty of fighting the brain's hormonal defense systems has catalyzed a medical revolution. The advent of highly effective incretin therapies, specifically glucagon-like peptide-1 (GLP-1) receptor agonists and dual GIP/GLP-1 agonists, has shifted the paradigm from viewing obesity as a failure of willpower to treating it as a complex, chronic, and relapsing metabolic disease 82829.
Medications like semaglutide (Wegovy, Ozempic) and tirzepatide (Zepbound, Mounjaro) chemically mimic native satiety hormones 143049. By interacting directly with receptors in the brain and gut, they drastically slow gastric emptying, stimulate insulin appropriately, and forcefully suppress the appetite centers of the hypothalamus 144931. They essentially drown out the body's starvation alarms (plunging leptin and surging ghrelin), allowing patients to sustain a caloric deficit without enduring intense physical and psychological hunger 84931.
Altering the Metabolic Blueprint
Beyond simply reducing caloric intake, advanced clinical trials and preclinical animal models suggest these drugs interact with resting energy expenditure and metabolic adaptation in unique and profound ways.
In a highly controlled 2026 study using obese minipigs, researchers compared diet restriction alone against diet restriction paired with semaglutide 7. The diet-only group experienced the classic hallmarks of metabolic adaptation: a sharp drop in energy expenditure, severe loss of fat-free mass, and decreased cellular energy function (specifically decreased mitochondrial proton leak) 7. Conversely, the semaglutide group achieved the exact same weight loss trajectory but avoided these energy-conserving adaptations. The medication appeared to chemically prevent the metabolism from slowing down, preserving fat-free mass and maintaining cellular energy functions 7.
| Characteristic | GLP-1 Receptor Agonists (e.g., Semaglutide) | Dual GIP/GLP-1 Agonists (e.g., Tirzepatide) |
|---|---|---|
| Mechanism of Action | Targets GLP-1 receptors to delay gastric emptying and suppress appetite 3049. | Targets both GLP-1 and GIP receptors, providing synergistic appetite control and metabolic benefits 304932. |
| Energy Expenditure Response | Initially causes a transient reduction in energy expenditure as weight rapidly drops, aligning with natural adaptation, but prevents severe long-term conservation 3132. | Has been shown in animal models to trigger a profound, temporary increase in resting energy expenditure independent of physical activity 3132. |
| Fat Oxidation | Shifts the respiratory exchange ratio (RER) to heavily favor fat oxidation over carbohydrate metabolism during treatment 3132. | Similarly decreases RER, mobilizing fat stores effectively 31. |
| Clinical Weight Loss (Averages) | Approximately 15% to 17% body weight reduction in non-diabetic populations over 68 weeks (STEP 1 trials) 5233. | Frequently exceeds 20% to 22.5% body weight reduction over similar timeframes (SURMOUNT trials) 54. |
Furthermore, head-to-head trials have continually demonstrated that tirzepatide generally yields superior weight loss compared to semaglutide 345635. While both medications dramatically alter the metabolic landscape, they only work as long as the chemical signal is present. When treatment is withdrawn, the artificial satiety signals vanish, the suppressed baseline appetite rebounds, and the vast majority of patients regain the lost weight 325254.
Global Guidelines and the Future of Treatment
The staggering efficacy of these therapies has prompted international action. The World Health Organization (WHO) recently released its first living guidelines on the use of GLP-1 therapies, officially recognizing obesity as a chronic disease requiring lifelong care 282936.
With over 1 billion people globally affected by obesity - driving millions of deaths and trillions in economic costs - the WHO now advocates for these medications as long-term treatments, provided they are integrated with comprehensive behavioral interventions, dietary support, and resistance training to protect muscle mass 282937.
The clinical pipeline is already advancing beyond dual-agonists. Emerging trials are testing triple-hormone-receptor agonists (like retatrutide, targeting GIP, GLP-1, and glucagon), which are demonstrating bariatric surgery-level weight loss approaching 24% of total body weight in Phase 2 trials 54. Researchers are also aggressively investigating oral formulations and combination therapies specifically designed to maintain weight loss and preserve muscle mass after transitioning off GLP-1 treatments, hoping to finally outsmart the body's relentless drive to regain weight 5460.
Bottom line
When you reduce your caloric intake, your body actively fights the loss of stored energy by orchestrating a drop in your resting metabolic rate and a surge in hunger-stimulating hormones. This adaptive thermogenesis is a powerful evolutionary survival mechanism that makes the journey to a lower weight remarkably difficult, but it is not a permanent breaking of your metabolism. While strategic diet breaks, high protein intake, and resistance training can help preserve metabolic function, overcoming the body's biological defense requires sustained behavioral consistency or the integration of modern, long-term pharmacological therapies.