5 Myths About GLP-1 Weight-Loss Drugs Debunked
Glucagon-like peptide-1 (GLP-1) receptor agonists - such as semaglutide and tirzepatide - drive profound weight loss not by melting fat or artificially spiking metabolism, but by rewiring the brain's hunger circuitry. While current evidence confirms they do not inherently destroy muscle tissue or chemically age the skin, they do require careful nutritional management and are designed for long-term chronic use, as stopping the medication typically results in substantial weight regain.
The Paradigm Shift in Global Obesity Management
The medical and public health landscapes are currently experiencing an unprecedented transformation in the clinical management of obesity and metabolic syndrome. For decades, the foundational advice for weight management relied almost entirely on behavioral modifications: caloric restriction and increased physical activity. However, mounting longitudinal data has repeatedly demonstrated that lifestyle interventions alone are often insufficient for sustained, long-term weight loss. The human body possesses powerful, evolutionarily conserved physiological adaptations that fiercely defend a person's highest body weight, unleashing hormonal counter-regulatory responses whenever a caloric deficit is introduced 121.
The widespread adoption of incretin-based therapies - specifically glucagon-like peptide-1 (GLP-1) receptor agonists and dual glucose-dependent insulinotropic polypeptide (GIP) agonists - has disrupted this behavioral paradigm. Medications such as semaglutide (marketed as Wegovy, Ozempic, and Rybelsus) and tirzepatide (marketed as Zepbound and Mounjaro) routinely achieve 15 to 25 percent reductions in total body weight in clinical trials, rivaling the historical efficacy of metabolic and bariatric surgery 4562.
Because these medications have rapidly saturated the public consciousness, they have also generated a vast ecosystem of misinformation. Unsubstantiated claims regarding their safety, mechanisms of action, and long-term consequences proliferate across media platforms. The sheer demand for these drugs has also strained global healthcare systems, leading to profound supply shortages, the rise of unregulated compounded alternatives, and intense debates over insurance coverage 34511. To make informed healthcare decisions, it is critical to separate physiological reality from sensationalism. By examining peer-reviewed data, clinical trial outcomes, and extensive regulatory safety reviews from 2024 and beyond, we can systematically deconstruct the five most pervasive myths surrounding GLP-1 medications.
Myth 1: GLP-1 Medications Chemically Destroy Your Muscle Mass
One of the most persistent alarms raised about GLP-1 receptor agonists is the claim that they aggressively target and dissolve lean muscle tissue. Critics often point to clinical trial data showing that a significant portion of the weight lost by patients taking medications like semaglutide and tirzepatide comes from fat-free mass, which includes skeletal muscle, bone, and water.
The Universal Biology of Weight Loss and Lean Mass
To understand why this myth is misleading, it is necessary to examine the universal physiology of weight loss. The human body does not possess a mechanism to exclusively burn adipose tissue (fat) while in a state of caloric deficit. Whenever an individual loses a substantial amount of weight - whether through traditional dieting, intensive exercise, bariatric surgery, or pharmacotherapy - they inevitably lose a combination of fat mass and fat-free mass 1121314.
A highly publicized commentary published in The Lancet by researchers from the Pennington Biomedical Research Center highlighted that muscle loss can account for 25 to 39 percent of the total weight lost over a 36-to-72-week period on GLP-1 medications 13. Because these drugs are so effective at suppressing appetite, patients often enter a severe caloric deficit. Without intentional nutritional and physical interventions, the body will break down muscle tissue to meet its daily energy requirements. The researchers noted that this rate of muscle decline is higher than what is typically observed with normal aging - which is roughly 8 percent per decade - raising concerns about long-term cardiorespiratory fitness (CRF), frailty, and overall metabolic health 1213.
However, the loss of muscle is a natural consequence of the rapid caloric restriction, not a direct, toxic effect of the GLP-1 molecule on muscle fibers 1415. Pre-clinical research, including extensive studies on obese mouse models and humans, demonstrates that GLP-1 medicines predominantly reduce body fat. While absolute muscle mass may decrease slightly, relative muscle mass and strength often improve due to the massive reduction in burdensome fat, resulting in better overall mobility and physical performance 16. Furthermore, clinical studies indicate that GLP-1-induced weight loss leads to an increased proportion of lean mass relative to total body weight, which is generally viewed as a positive shift in overall body composition 1.
Mitigating Muscle Loss Through Strategic Protocols
The medical consensus is not to avoid GLP-1 therapies due to fears of muscle atrophy, but rather to pair the medication with proactive, muscle-sparing protocols. Clinical guidelines strongly emphasize that preserving lean tissue requires two non-negotiable behavioral changes: dramatically increased protein consumption and progressive resistance training.
Because GLP-1 medications drastically reduce a patient's overall food intake - sometimes by as much as 40 percent of their usual dietary volume - achieving adequate daily protein becomes mathematically and practically difficult due to profound early satiety 1417. A 2025 study of adults using GLP-1 RAs found that average protein intake was only 77 grams per day, falling well below clinical recommendations 17. While the average non-dieting adult requires about 0.8 grams of protein per kilogram of body weight, patients actively losing weight on GLP-1 therapies must double this intake.
Clinical nutrition centers and endocrinology guidelines recommend a target of 1.2 to 2.2 grams of protein per kilogram of body weight daily to provide the necessary amino acids for muscle repair and synthesis 141819. The Joslin Diabetes Center recommends calculating this based on an adjusted body weight to prevent overfeeding, focusing on high-quality, complete protein sources such as lean meats, fish, dairy, legumes, and plant-based alternatives 196.
Dietary interventions must be coupled with a mechanical stimulus. Structured resistance training three to four times per week is critical for lean mass preservation 1417. When a patient engages in progressive overload - lifting weights at 75 to 85 percent of their one-rep maximum - they send an essential biological signal to the body that muscle tissue is required for survival, forcing the metabolism to prioritize adipose tissue to fill the caloric deficit 14. Patients who initiate resistance training within the first two to three weeks of starting GLP-1 therapy recover significantly more lean mass than those who delay exercise until later in their treatment 14.
The Impact on Bone Mineral Density
Alongside skeletal muscle, researchers are closely monitoring how GLP-1 medications impact bone mineral density (BMD). As body weight decreases, bones experience less mechanical loading (Wolff's Law), which naturally reduces the stimulus to maintain bone mass 21. Some studies, including data presented at the 2024 American Academy of Orthopaedic Surgeons meeting, observed a modest 30 percent relative increase in osteoporosis diagnoses among certain GLP-1 users compared to non-users, alongside increased risks of gout flares due to rapid fluctuations in uric acid 227.
However, the context of these findings is nuanced. Research from Epic Research analyzing over 2 million patients found that for individuals with type 2 diabetes, GLP-1 use was actually associated with an 8.7 percent lower risk of osteoporosis compared to non-users, though the risk was slightly elevated in non-diabetic populations 8. Crucially, a 2024 clinical trial published in JAMA Network Open split patients into exercise-only, GLP-1-only, and combined groups. The results were unambiguous: while patients on GLP-1 medication alone saw bone density decline at the hip and spine, patients who combined the medication with resistance exercise preserved their bone density completely while still maximizing fat loss 21.
Myth 2: The Medication Causes Unnatural Skin Aging and "Ozempic Face"
As GLP-1 medications surged in popularity, a phenomenon dubbed "Ozempic Face" began dominating media headlines. The term describes the sudden appearance of sunken cheeks, hollow eyes, pronounced nasolabial folds, and sagging jowls in patients taking the drug. The pervasive myth suggests that the medication itself contains compounds that actively attack collagen or accelerate the biological aging process of the skin.
The Structural Role of Subcutaneous Facial Fat
From a dermatological and plastic surgery perspective, "Ozempic face" is neither a medical diagnosis nor a side effect specific to semaglutide or tirzepatide 25. It is a well-documented morphological consequence of rapid and massive weight loss, irrespective of how that weight loss is achieved 152627.
The youthful appearance of the human face relies on a delicate architectural balance of skin, muscle, connective tissue, and specific compartments of subcutaneous fat. Facial fat pads provide essential structural support, acting as a kind of biological filler that keeps the overlying skin taut and voluminous 28. When a patient carries excess weight for an extended period, the skin of the face stretches to accommodate the underlying adipose tissue.
When a patient takes a highly effective GLP-1 agonist, they often experience accelerated fat loss across their entire body. The body does not selectively preserve facial or breast fat; weight loss occurs globally, leading to similar colloquial terms like "Ozempic body" or "Ozempic butt" 15. As these facial fat pads shrink rapidly, the overlying skin - which may already suffer from reduced elasticity due to age, genetics, or chronic sun exposure - does not have adequate time to contract and adapt to the new, smaller facial volume 252627. The resulting deflation causes gravity to pull the loose tissue downward, emphasizing existing wrinkles, creating hollows under the eyes, and resulting in an overall gaunt or fatigued appearance 252628.
Compensatory Remodeling and Medical Aesthetics
The accelerated evidence of facial aging is a direct consequence of preferential volume loss of adipose tissue without compensatory collagen remodeling at the level of the skin 15. This phenomenon is identical to the facial changes observed in patients who undergo bariatric surgery or achieve massive weight loss through extreme caloric restriction; it simply affects a broader demographic now that injectable pharmacotherapy is widely accessible 152527.
Understanding that this is a biomechanical volume-loss issue rather than a chemical-toxicity issue informs how the medical community addresses it. Slower, more moderate weight loss trajectories can sometimes give the skin's collagen matrix more time to adapt, mitigating the severity of the hollowing 2627. For patients who experience significant facial deflation, plastic surgeons and dermatologists utilize established aesthetic interventions. Non-surgical treatments like dermal fillers or autologous fat grafting are routinely used to restore volume to the temples, tear troughs, and cheeks 1526. Modalities that stimulate collagen production, such as microneedling and targeted ultrasound therapies (like Sofwave or Ultherapy), help tighten mild skin laxity by initiating the body's natural healing processes 2628. In cases of severe global skin redundancy, surgical interventions such as a lower facelift or blepharoplasty remain the definitive solution for morphological changes following massive weight loss 15.
Ultimately, GLP-1 receptor agonists do not prematurely age the skin; they effectively eliminate the fat that was previously stretching it.
Myth 3: GLP-1s Work by Artificially Boosting Your Metabolic Rate
Because GLP-1 receptor agonists are frequently referred to as "weight-loss drugs," many patients mistakenly assume they function similarly to older, stimulant-based diet pills (such as phentermine) or lipotropic injections. A common misconception is that semaglutide and tirzepatide act as thermogenic agents that artificially spike the basal metabolic rate, causing the body to burn significantly more calories while at rest.
The Neurology of Appetite and Satiety
The clinical reality is entirely different. GLP-1 medications do not directly increase the metabolic rate in any traditional sense 29. Instead, their primary mechanism of action relies on fundamentally rewiring the neurological pathways that govern appetite, satiety, and reward.
Glucagon-like peptide-1 is a naturally occurring incretin hormone secreted by the enteroendocrine cells of the gut in response to carbohydrate and fat ingestion. In its natural state, it stimulates insulin secretion, suppresses glucagon release from the liver, and delays gastric emptying, keeping food in the stomach longer 493110. However, native GLP-1 is rapidly degraded by enzymes in the body within minutes. Pharmaceutical GLP-1 receptor agonists are structurally modified to resist this enzymatic degradation, allowing them to remain active in the bloodstream for days or even a full week 1033.
Crucially, these medications cross the blood-brain barrier and target specific receptors in the hypothalamus, the brainstem, and the brain's reward centers 33. Within the arcuate nucleus of the hypothalamus - the brain's master control center for hunger - GLP-1 medications act as a highly targeted neurological switchboard. They simultaneously activate POMC/CART neurons, which suppress appetite and signal profound, lasting fullness, while actively inhibiting NPY/AgRP neurons via GABAergic transmission, shutting down the signals that drive hunger and food-seeking behavior 31103334.
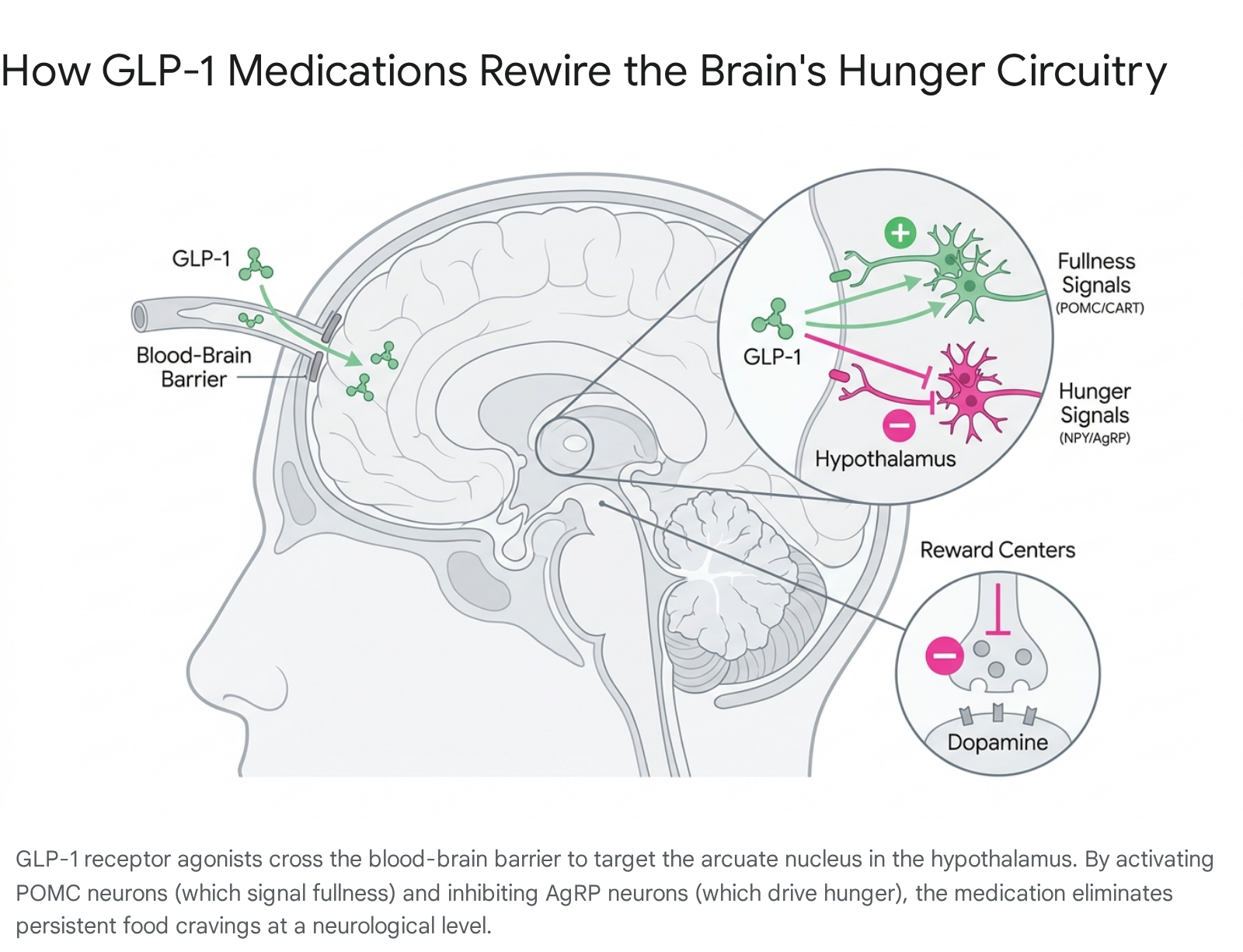
Furthermore, these medications influence the nucleus accumbens and the ventral tegmental area, regions of the brain that dictate the pleasure and emotional reward derived from eating 31. By dampening the dopamine response triggered by highly palatable, high-calorie foods, GLP-1 medications eliminate the obsessive "food chatter" or "food noise" that plagues many individuals living with obesity, changing food preferences at a fundamental neurological level 3133.
Metabolic Adaptation and Fuel Partitioning
Far from boosting the metabolism, total energy expenditure actually decreases as patients lose weight on GLP-1 therapies. This is a normal biological phenomenon known as metabolic adaptation; as body mass shrinks, the body requires fewer calories to maintain itself 1229. The medications do not prevent this natural reduction in the resting metabolic rate 29.
However, GLP-1s do possess a distinct "metabolic advantage" compared to sheer willpower. During traditional, unmedicated calorie restriction, the body aggressively fights back by slowing the metabolism sharply and releasing massive surges of the hunger hormone ghrelin 135. GLP-1 medications prevent this aggressive counter-regulatory response, easing the hormonal friction that typically guarantees dietary failure. Furthermore, emerging research indicates that GLP-1 and dual-agonist drugs directly alter metabolic shifts, increasing fat oxidation and improving the way the body partitions fuel, independent of the sheer reduction in caloric intake 35. Research utilizing fluorescence imaging in mouse brain tissue has revealed that this weight-loss effect depends heavily on cyclic adenosine monophosphate (cAMP) signaling inside the neurons, explaining why patients respond differently to the medications on a cellular level 36.
Single, Dual, and Triple Agonists: The Evolution of Efficacy
Understanding that these drugs work via receptor activation rather than metabolic acceleration explains why newer generations of the medication are increasingly effective. Semaglutide is a single agonist, targeting only the GLP-1 receptor. Tirzepatide, a dual agonist, engages both the GLP-1 receptor and the glucose-dependent insulinotropic polypeptide (GIP) receptor 45637.
Historically, GIP was thought to have a weaker effect on weight, but modern pharmacology has revealed that activating both receptors synergistically enhances insulin sensitivity, glucagon suppression, and centrally mediated appetite reduction 4937. Clinical trials show tirzepatide generally leads to a greater average weight loss (20 to 25 percent) compared to semaglutide (15 to 17 percent) 3738.
The frontier of this research is retatrutide, an investigational triple agonist currently in Phase 3 trials. Retatrutide targets GLP-1, GIP, and glucagon receptors simultaneously. In Phase 2 trials published in the New England Journal of Medicine, patients on the highest dose of retatrutide (12 mg) achieved a staggering 24.2 percent mean reduction in body weight over just 48 weeks - with roughly 10 to 15 percent of patients losing 30 percent or more of their body weight 39401142. This progressive increase in efficacy confirms that weight loss is driven by complex neuroendocrine receptor signaling, not crude metabolic stimulation.
| Medication (Active Ingredient) | Receptor Targets | Primary Action Mechanism | Average Clinical Weight Loss | FDA/MHRA Status (As of 2024/2025) |
|---|---|---|---|---|
| Semaglutide (Wegovy, Ozempic) | GLP-1 | Slows gastric emptying, signals profound satiety in the hypothalamus. | 15% - 17% (at 68 weeks) | Approved for Type 2 Diabetes and Obesity 53743. |
| Tirzepatide (Zepbound, Mounjaro) | GLP-1 + GIP | Dual action enhances insulin sensitivity and magnifies appetite suppression. | 20% - 25% (at 72 weeks) | Approved for Type 2 Diabetes and Obesity 53743. |
| Retatrutide (Investigational) | GLP-1 + GIP + Glucagon | Triple agonism maximizes energy utilization and neuroendocrine satiety signaling. | 24.2% (at 48 weeks, Phase 2 data) | Investigational; Not yet approved for clinical use 394042. |
Myth 4: Rebound Weight Gain Proves the Drugs Ruin Your Natural Metabolism
A common headline regarding GLP-1 medications warns that patients regain the weight "four times faster" when they stop taking the drug compared to stopping a traditional diet. This statistic is frequently used to argue that the medications inflict permanent damage on the body's natural metabolic function, trapping the patient in a cycle of lifelong chemical dependency.
The Illusion of "Four Times Faster"
The claim that weight is regained four times faster is mathematically accurate but highly misleading without proper context. This figure emerged from systematic reviews evaluating dozens of weight-loss interventions. When analyzing the data, researchers found that patients who discontinued GLP-1 therapies regained their lost weight over roughly four years, whereas those who stopped lifestyle interventions (diet and exercise alone) also regained their weight, but over a much slower timeline 4412.
The reason for this discrepancy is the sheer magnitude of the initial weight loss. In the STEP 1 and SURMOUNT-4 trials, patients on semaglutide or tirzepatide lost between 15 and 20 percent of their body weight rapidly 441213. In contrast, intensive lifestyle-only trials - such as the landmark Diabetes Prevention Program (DPP) or the Look AHEAD study - typically result in an average weight loss of only 5 to 8 percent, followed by slow regain despite ongoing program engagement 44. If a patient loses 20 kilograms on a medication and regains 15 kilograms, their absolute rate of regain is numerically much faster than a dieting patient who only lost 4 kilograms and regained 3 kilograms 4412. The body is simply replacing a much larger deficit, but the proportional trajectory of biological failure is remarkably similar across all modalities of obesity treatment.
The SURMOUNT-4 and STEP 4 Discontinuation Trials
Rigorous clinical trials have specifically tested what happens when the physiological support of these medications is withdrawn. In the SURMOUNT-4 trial, patients underwent a 36-week lead-in period on tirzepatide, experiencing a massive mean weight reduction of 20.9 percent 3813. At week 36, half the participants were randomly assigned to switch to a placebo, while the other half continued the medication for an additional 52 weeks.
The results were definitive: the group that continued tirzepatide lost an additional 5.5 percent of their body weight, achieving a total mean weight reduction of 25.3 percent over 88 weeks 3813. Meanwhile, the group switched to the placebo experienced a rapid reversal, regaining 14.0 percent of their body weight over the next year 3813.
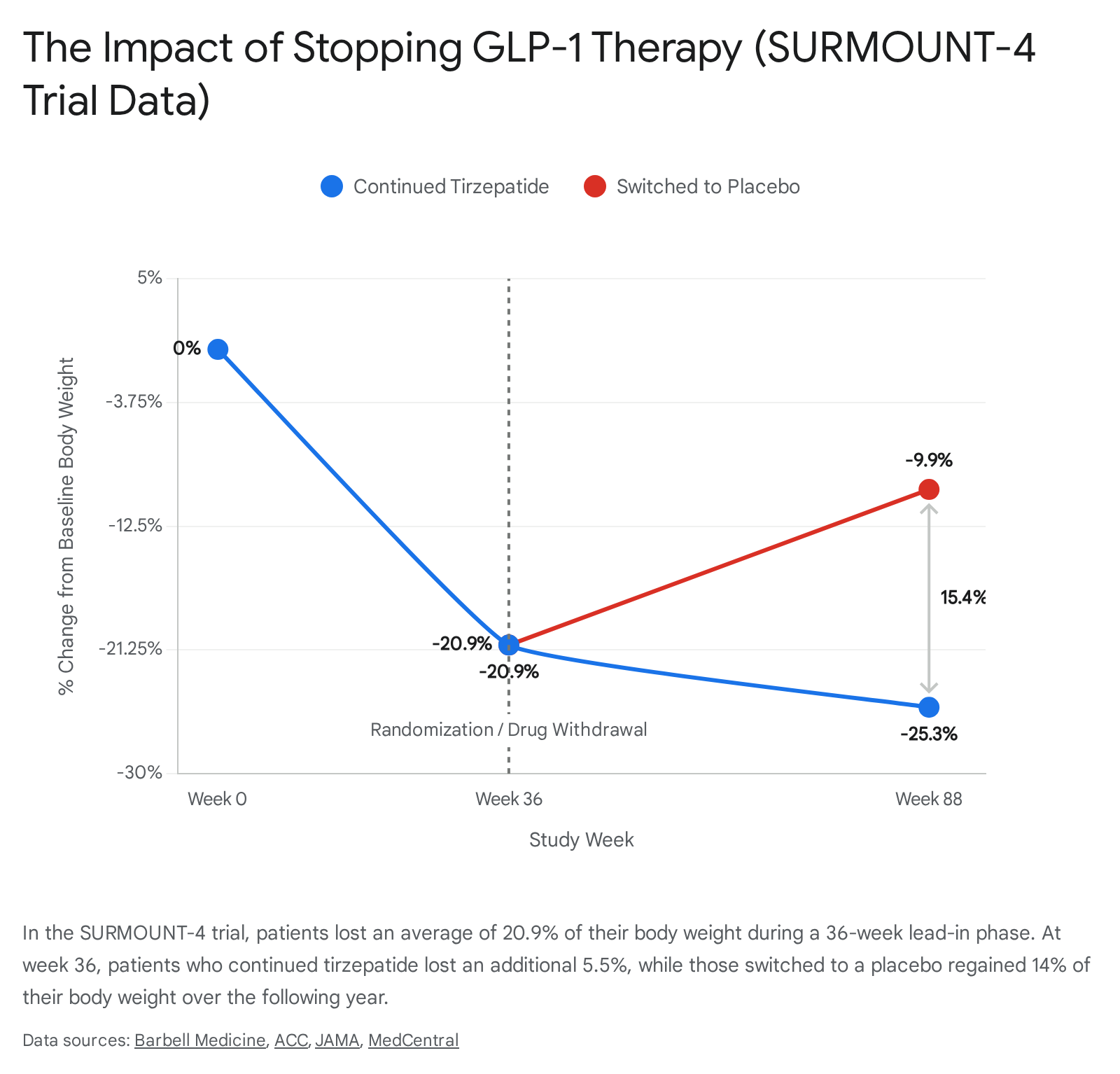
This means they regained roughly two-thirds of the weight they had initially lost within 12 months 4412.
Furthermore, this rapid weight regain was accompanied by a direct reversal of their cardiometabolic improvements. The placebo group saw significant rebounds in waist circumference (an increase of up to 14.7 cm in the highest regain category), systolic blood pressure (increasing by 10.4 mm Hg), non-HDL cholesterol, and fasting insulin levels 47. The STEP 1 and STEP 4 trials evaluating semaglutide discontinuation mirrored these exact findings, confirming a class-wide effect 44.
Reframing Obesity as a Chronic Disease
The intense regain experienced after stopping a GLP-1 agonist does not indicate that the drug has damaged the metabolism. Rather, it highlights a profound paradigm shift in how the medical community views severe overweight and obesity. Much like hypertension or type 2 diabetes, obesity is increasingly recognized as a chronic, relapsing disease 14.
If a patient with high blood pressure stops taking their anti-hypertensive medication, their blood pressure will inevitably rise. The medical community does not blame the medication for "ruining" the cardiovascular system; it acknowledges that the medication was actively managing a chronic biological defect. Similarly, GLP-1 medications correct the hormonal dysregulation of satiety and energy balance. When the exogenous hormones are removed, the patient's underlying neurobiology returns to its baseline state, and the body's natural defense of its previous high weight resumes 4715.
This underscores why major clinical guidelines from organizations like the World Health Organization (WHO) and the American Diabetes Association conceptualize these interventions as long-term, potentially lifelong pharmacotherapy 381416. To combat the issue of lifelong injections, researchers are currently exploring oral maintenance drugs. In 2026 pre-clinical studies, researchers at the University of Alabama at Birmingham demonstrated that an investigational oral drug named TIX100 completely prevented weight rebound in mouse models after semaglutide was stopped, signaling a potential future "off-ramp" for patients 17.
Myth 5: Long-Term Use Causes Severe Psychiatric and Physical Harm
The unprecedented demand for GLP-1s has spawned widespread anxiety regarding their long-term safety profile. Sensational reports frequently suggest that taking these medications for years will inevitably lead to severe mental health crises, pancreatic cancers, or the rapid degradation of internal organs.
The Suicidality and Mental Health Investigations
In mid-2023, the Icelandic Medicines Agency flagged several post-marketing reports of suicidal ideation and self-harm among patients taking liraglutide and semaglutide. This triggered massive, parallel pharmacovigilance investigations by the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) to determine if GLP-1 medications chemically altered the brain to induce depression or suicidality 521819.
After almost a year of rigorous analysis - which included parsing spontaneous adverse-event reports, analyzing massive electronic health record databases via the Sentinel System, and conducting a meta-analysis of 91 placebo-controlled trials involving over 107,000 patients - both regulatory bodies reached the same definitive conclusion in April 2024: there is no evidence of a causal link between GLP-1 receptor agonists and suicidal thoughts or actions 52192021.
In fact, extensive retrospective cohort studies comparing patients on GLP-1s to those on other diabetes medications (like SGLT2 inhibitors) found a significantly lower risk of incident suicidal ideation and intentional self-harm among the GLP-1 users 181920. Following this comprehensive review, the FDA requested that drug manufacturers remove the warnings regarding suicidal behavior and ideation from the labeling of medications like Wegovy and Zepbound 1920. Health Canada conducted a similar safety review and also concluded that the evidence did not support a causal link, though they emphasized the need for ongoing monitoring in the general obese population due to inconsistent data in isolated sub-groups 57.
It is worth noting, however, that the psychological impact of GLP-1s is complex. Because the drugs interfere with the pleasure and reward derived from eating, patients who previously relied on food as a primary coping mechanism for stress or depression may experience mood disturbances. Australian prescribing guidelines explicitly warn that rapid appetite loss can complicate mental health assessments, as patients are forced to navigate a radically altered relationship with food 15.
10-Year Data: Pancreatitis, Gallbladder, and Cancer Risks
While the explosion of GLP-1 use for obesity feels recent, the drug class has been heavily studied for over a decade. Liraglutide was approved for type 2 diabetes in 2010 and for weight management in 2014, while semaglutide was approved for diabetes in 2017 165859. This provides a robust window of long-term safety data that counteracts much of the public fear.
Early theoretical concerns that these drugs would cause high rates of pancreatitis or pancreatic cancer have been largely dispelled by large-scale cardiovascular outcome trials and meta-analyses. The rates of pancreatitis in patients taking GLP-1s are statistically similar to the background rates found in the general population living with obesity and diabetes 5859. Similarly, the National Academy of Medicine reports no significant long-term safety concerns regarding overall cancer risk related to the medications 58.
GLP-1 medications are associated with a modest increase in gallbladder events, such as gallstones. However, clinical data shows this is an indirect effect of rapid weight loss rather than a direct toxic effect of the drug on the gallbladder. These events primarily occur in the first year of treatment when weight loss is most aggressive, and the rates stabilize over the long term 1459.
The most common side effects remain gastrointestinal - specifically nausea, vomiting, diarrhea, and constipation. In clinical trials, these effects caused roughly 6.5 percent of people to abandon the medication, compared to 3.6 percent on placebo 131458. However, real-world data shows a much starker reality: 50 to 75 percent of people stop taking GLP-1 medications within the first year, driven heavily by persistent GI side effects, inadequate medical support, and prohibitive costs 121758.
Unprecedented Cardiovascular Protection
Far from being dangerous, long-term GLP-1 use offers profound, unprecedented cardiovascular benefits that actively extend life. The landmark SELECT trial, which followed over 17,000 non-diabetic patients with existing cardiovascular disease for a median of 40 months, demonstrated that taking semaglutide resulted in a 20 percent reduction in major adverse cardiovascular events (MACE), including heart attacks, strokes, and cardiovascular death 5859.
Similarly, the LEADER trial tracking liraglutide found a 13 percent reduction in MACE, while research published in the Journal of Clinical Investigation linked GLP-1 use to a 21 percent lower all-cause mortality compared to other diabetes medications 5859. These cardioprotective effects are so definitive that the medications are now widely prescribed explicitly for cardiovascular risk reduction, and are being investigated for protective effects against kidney disease and obstructive sleep apnea 385860.
The Global Struggle for Access and Coverage
Despite the overwhelming clinical evidence supporting the efficacy and safety of GLP-1 therapies, access remains highly inequitable globally. The rapid surge in demand - driven in part by extensive media attention and off-label cosmetic use - has triggered massive supply chain failures. In 2023 and 2024, the UK, Australia, Canada, and the US all experienced critical shortages of semaglutide and tirzepatide, forcing regulators to issue safety alerts prioritizing existing patients 34612263.
This vacuum led to a dangerous rise in falsified GLP-1 products sold through unregulated social media platforms, prompting the World Health Organization (WHO) to issue a global medical product alert regarding contaminated and ineffective counterfeit pens 56423. While manufacturing capacity has expanded and shortages were largely reported as resolved by early 2025 in the UK and Australia, the sheer cost of the drugs continues to dictate who receives care 31122.
Healthcare systems worldwide are currently wrestling with how to fund lifelong treatment for a disease that affects up to 40 percent of the adult population. * United Kingdom: The National Institute for Health and Care Excellence (NICE) strictly limits NHS access. Tirzepatide (Mounjaro) is recommended only for adults with a BMI of at least 35 kg/m2 (adjusted for ethnicity) and at least one weight-related comorbidity, rolled out in a highly phased, prioritized approach through primary care and specialized Tier 3 weight management services 43606624. * Australia: The Pharmaceutical Benefits Advisory Committee (PBAC) has faced immense pressure to subsidize GLP-1s for obesity on the Pharmaceutical Benefits Scheme (PBS). Currently, PBAC recommends prioritizing groups with established cardiovascular disease or syndromic obesity, noting that universal subsidization could be financially untenable without massive price reductions 2225. * Canada: Weight loss medications are generally excluded from public health plans. Private group insurance plans are highly resistant to covering GLP-1s for obesity due to annual costs exceeding $5,000 per patient, which actuaries estimate could drive up group plan premiums by 10 to 20 percent 1170. Furthermore, Health Canada strictly limits the use of compounded semaglutide, allowing it only during official shortages 11. * United States: Historically, Medicare has been prohibited by statute from covering purely weight-loss medications. However, due to the proven cardiovascular benefits, the Centers for Medicare & Medicaid Services (CMS) is attempting a massive policy shift. The short-term "Medicare GLP-1 Bridge" program will allow eligible Part D beneficiaries to access drugs like Wegovy and Zepbound for a flat $50 monthly copay from July 2026 through December 2027 71722674. With over 21 million Medicare claims already generating $27.5 billion in gross spending for GLP-1s in 2024 (mostly for diabetes), expanding coverage to obesity is expected to cost the federal government billions annually 722674.
In low- and middle-income countries (LMICs), where obesity rates have doubled since 2010, national coverage is virtually non-existent. Global health advocates hope that the imminent expiration of early GLP-1 patents will introduce generic competition, driving down prices and democratizing access to these life-saving therapies 27.
Bottom line
GLP-1 receptor agonists are a revolutionary class of medications that effectively treat obesity by altering deep neurological pathways related to satiety and reward, not by unnaturally stimulating the metabolism or chemically destroying healthy tissue. The most common physical side effects - including lean muscle loss, facial hollowing, and reduced bone density - are direct consequences of rapid weight loss and severe caloric restriction, all of which can be heavily mitigated with adequate protein intake and proactive resistance training. While the last decade of data proves these medications are safe for long-term use and provide exceptional cardiovascular protection, obesity must be treated as a chronic disease; halting the medication generally results in the predictable return of the underlying neurobiology and the subsequent regain of weight. What remains uncertain is whether emerging therapies, such as oral maintenance drugs or triple-agonists like retatrutide, will eventually offer a permanent, accessible "off-ramp" for patients navigating the complexities of lifelong obesity management.