What Happens to Your Body When You Start GLP-1s
Starting a GLP-1 medication triggers immediate changes in your digestive tract and brain, dramatically slowing digestion while quieting the neural pathways that drive food cravings. Over the following months, this dual action typically leads to a 15 to 22 percent reduction in total body weight, alongside profound, well-documented improvements in cardiovascular, metabolic, and renal health. Because these medications address the underlying biology of obesity rather than relying on caloric willpower, maintaining these sweeping physiological benefits usually requires long-term, ongoing treatment.
The Biology of GLP-1: Beyond Just Feeling Full
To understand what happens to your body when you take a glucagon-like peptide-1 (GLP-1) receptor agonist like semaglutide (Wegovy, Ozempic) or a dual GLP-1/GIP agonist like tirzepatide (Zepbound, Mounjaro), it is essential to look beyond the stomach. While these medications are famous for making people eat less, their mechanisms are deeply rooted in the endocrine system and the brain's reward circuitry.
The Incretin Effect and the "Dimmer Switch"
Obesity is increasingly recognized by medical authorities not as a failure of character, but as a biological mismatch between an ancient human body and a modern environment characterized by hyper-palatable, calorie-dense foods 1. In a natural state, the gut acts as a highly sensitive endocrine organ. When you eat, specialized cells in the intestine release incretin hormones, primarily GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) 1.
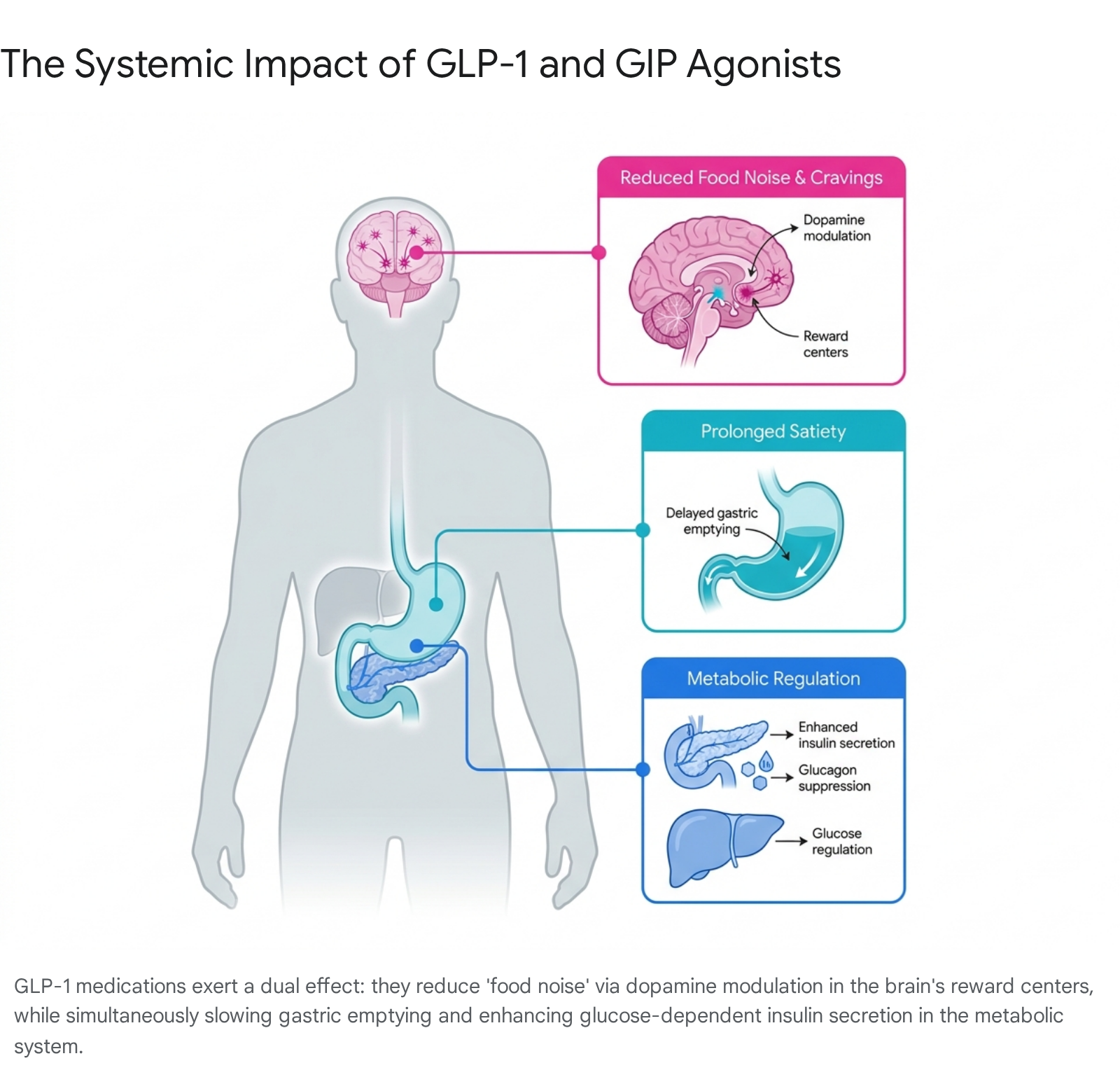
These hormones act as a physiological relay system. They signal the pancreas to release insulin, but they do so in a strictly glucose-dependent manner. Rather than forcing the pancreas to dump insulin unconditionally - which could cause a dangerous drop in blood sugar - GLP-1 and GIP act like a metabolic "dimmer switch." They amplify insulin secretion only when glucose from food is actually present in the bloodstream 1.
When you start a synthetic GLP-1 medication, you are introducing a long-lasting, highly concentrated version of this natural hormone. Native GLP-1 is broken down by the body in a matter of minutes; medications like semaglutide and tirzepatide are structurally modified to resist this breakdown, remaining active in the bloodstream for a week 12. Consequently, the pancreas becomes highly efficient at managing blood sugar, while the liver is signaled to suppress the inappropriate release of stored glucose (glucagon suppression) 3.
Simultaneously, the medication acts on the gastrointestinal tract to slow gastric emptying. This means food physically remains in the stomach longer. By delaying the transition of food into the small intestine, the medication prolongs the physical sensation of fullness and blunts the sharp spikes in blood sugar that normally follow a meal 34.
Quieting "Food Noise" in the Brain
Perhaps the most profound change patients report when starting a GLP-1 medication occurs not in the gut, but in the mind. Many individuals with obesity suffer from what is colloquially called "food noise" - a constant, intrusive mental preoccupation with food, cravings, and meal planning 56.
Neurologically, food noise is thought to be driven by hyper-reactivity in the brain's reward centers, particularly the nucleus accumbens, combined with dysregulation in the Default Mode Network (DMN), the brain system responsible for mind-wandering and future planning 56. In patients with obesity, the DMN frequently engages in "maladaptive prospection," constantly simulating the short-term reward of eating highly palatable foods 6.
GLP-1 receptors are dense in the hypothalamus (the brain's energy regulation center) and in the reward circuitry 57. When the medication crosses into the brain, it binds to these receptors, directly interacting with appetite-regulating neuropeptides like pro-opiomelanocortin (POMC), which promotes satiety, and inhibiting neuropeptide Y (NPY), which drives hunger 5. Furthermore, it modulates dopamine signaling, effectively turning down the volume on the reward value assigned to hyper-palatable, high-sugar, and high-fat foods 57.
Functional MRI studies have shown that when patients on GLP-1 therapies view images of high-calorie foods, their brain's reward centers show significantly reduced activation compared to baseline 5. A recent case study published in Nature Medicine even utilized a brain-computer interface to show that tirzepatide directly suppressed signaling in the brain's reward center associated with binge-eating impulses 89. For the patient, this complex neurochemistry translates into a sudden, often unprecedented mental silence regarding food. Rather than acting as a forceful off-switch that eliminates all desire to eat, it functions more like a dimmer switch, reducing the urgency of cravings and allowing patients to distinguish between genuine physiological hunger and boredom or stress-induced eating 101112.
The Timeline: Weeks, Months, and Years on a GLP-1
The physical and metabolic changes induced by GLP-1 therapies do not happen instantly. The journey follows a distinct chronological trajectory, governed by the biology of the drug and clinical guidelines for safety.
The First Few Months: Titration and Side Effects
Because the gut is highly sensitive to the sudden introduction of synthetic incretins, jumping directly to a therapeutic dose would cause severe illness. Therefore, both semaglutide and tirzepatide follow a strict "titration" schedule, starting at a low, sub-therapeutic dose and slowly increasing every four weeks 1114.
During the first 4 to 12 weeks, the body is adjusting. This is when gastrointestinal adverse events are most prominent. Upwards of 60 to 80 percent of patients in clinical trials report transient, mild-to-moderate side effects such as nausea, diarrhea, vomiting, or constipation 121314. The delayed gastric emptying is the primary culprit; food sitting longer in the stomach can cause bloating, acid reflux, and early satiety 3.
Despite the low initial doses, many patients experience a rapid drop in food noise and an immediate suppression of appetite during this titration phase 14. Weight loss during this initial window can be rapid, but physicians caution that a significant portion of the very early weight lost in the first few weeks is water weight and glycogen depletion, followed soon after by steady fat loss 18.
The Plateau and Long-Term Maintenance
As patients reach the maximum tolerated maintenance doses (e.g., 2.4 mg for semaglutide, 10 mg or 15 mg for tirzepatide), weight loss becomes steady. Clinical trials consistently show that the steepest decline in body weight and the most rapid improvements in fasting plasma glucose occur within the first 12 to 30 weeks 1516.
By week 60 to 72, the weight loss trajectory generally begins to plateau 1516. This plateau is not a sign that the medication has "stopped working"; rather, it represents a new metabolic equilibrium. A smaller body requires fewer calories to maintain itself, and biological adaptations meant to defend against further weight loss begin to balance out the appetite-suppressing effects of the drug 1. At this stage, patients typically stabilize at a new baseline weight, provided they continue taking the medication, and focus shifts from active weight loss to long-term health maintenance 15.
Semaglutide vs. Tirzepatide: Understanding the Differences
While often grouped together in public discourse, semaglutide (Wegovy, Ozempic) and tirzepatide (Zepbound, Mounjaro) represent two distinct generations of incretin therapy. The choice between them increasingly depends on patient-specific factors, clinical goals, and the nuanced differences in their mechanisms 21.
Single vs. Dual Agonism
Semaglutide is a single receptor agonist. It binds exclusively to the GLP-1 receptor 21. It has a massive, highly established evidence base, having been on the market longer and rigorously tested in diverse, real-world populations, proving its efficacy and safety over many years 14.
Tirzepatide, conversely, is a "twincretin" - a dual agonist that binds to both the GLP-1 and the GIP receptors 17. GIP (glucose-dependent insulinotropic polypeptide) was historically thought to be less important for weight loss, but scientists discovered that combining it with GLP-1 creates a synergistic effect. The dual mechanism produces a more robust engagement of the brain's satiety centers and may further enhance lipid and fat metabolism 1423.
The Clinical Trial Evidence
The most direct comparison between the two medications comes from the recent SURMOUNT-5 trial, a head-to-head study of adults with obesity but without diabetes. In this trial, tirzepatide demonstrated statistically superior weight reduction. At week 72, participants on tirzepatide lost an average of 20.2 percent of their body weight, compared to 13.7 percent for those on semaglutide 1819.
Furthermore, nearly 50 percent of patients on tirzepatide lost at least 20 percent of their body weight, a benchmark that was historically only achievable through bariatric surgery 19. Observational data from real-world health systems echoes these clinical trials. A large cohort study utilizing electronic health records found that at 3, 6, and 12 months, patients on tirzepatide achieved significantly larger on-treatment changes in weight compared to those on semaglutide 1320.
| Medication Profile | Semaglutide (Wegovy, Ozempic) | Tirzepatide (Zepbound, Mounjaro) |
|---|---|---|
| Mechanism of Action | GLP-1 Receptor Agonist 21 | Dual GLP-1 & GIP Receptor Agonist 17 |
| Average Weight Loss | ~15% at 68 weeks (STEP 1 Trial) 121521 | ~20-22.5% at 72 weeks (SURMOUNT-1 Trial) 1228 |
| Head-to-Head Trial (SURMOUNT-5) | -13.7% body weight at 72 weeks 1819 | -20.2% body weight at 72 weeks 1819 |
| Primary Clinical Advantage | Unprecedented long-term cardiovascular safety data (SELECT trial) and robust real-world evidence 2122. | Statistically superior total weight loss and fat mass reduction in head-to-head comparisons 1819. |
The Body Composition Debate: Fat Loss vs. Muscle Loss
As the sheer magnitude of weight lost on these medications became apparent, a new concern emerged in the medical community and the media: the composition of that weight loss. Are GLP-1 medications causing disproportionate and dangerous muscle loss? The short answer is no, but the nuance is critical for long-term health.
What the Clinical Trials Actually Show
When a human body is in a caloric deficit and loses weight rapidly, it never loses only fat. A combination of fat mass and fat-free mass (which includes skeletal muscle, bone, water, and organ tissue) is always lost 423. A commonly cited physiological rule is that roughly 25 percent of weight lost through traditional dieting or bariatric surgery comes from lean mass 2425.
To determine if GLP-1s caused worse muscle loss than standard dieting, researchers embedded dual-energy X-ray absorptiometry (DXA) sub-studies into the major clinical trials.
In the STEP 1 trial for semaglutide, the DXA substudy (140 participants) revealed that while absolute lean mass decreased by 9.7 percent, total fat mass decreased by a massive 19.3 percent. Because the fat loss so heavily outpaced the lean mass loss, the proportion of lean body mass to total body weight actually increased by 3 percentage points 262728. The ratio of lean mass to fat mass objectively improved 2829.
The SURMOUNT-1 trial for tirzepatide (160 DXA participants) yielded similar results. Patients saw a 33.9 percent reduction in fat mass alongside a 10.9 percent reduction in lean mass 3031.
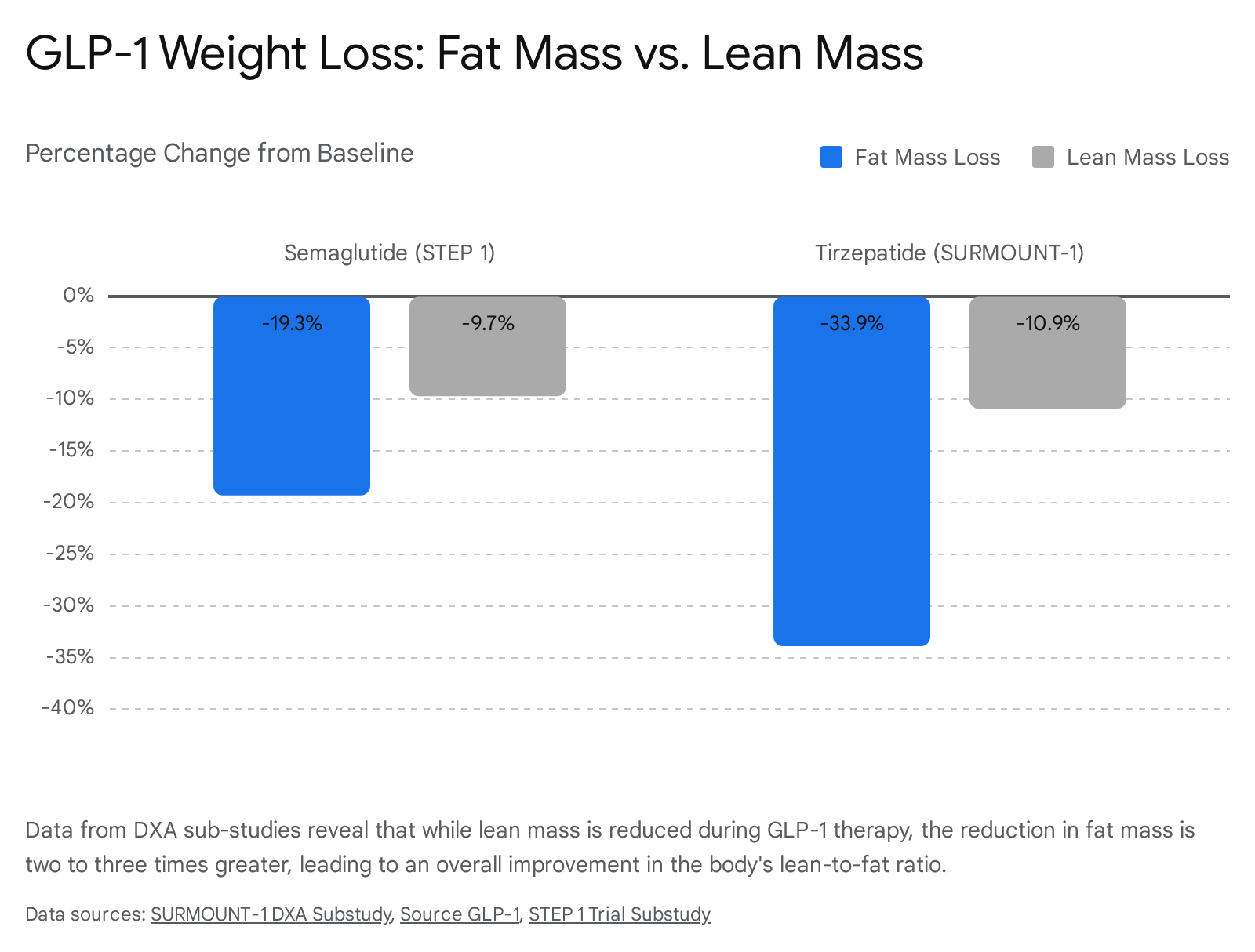
Crucially, of the total body weight lost, approximately 75 percent was fat mass and 25 percent was lean mass - aligning perfectly with expected biological norms for human weight loss 23303139.
Refining the Measurement: Intramuscular Fat and Function
Modern researchers argue that DXA scans actually overstate the amount of skeletal muscle lost. DXA technology measures lean mass as everything that isn't fat or bone - meaning it includes water, glycogen, organ tissue, and critically, intramuscular fat (fat marbled inside the muscle) 18.
When patients lose weight rapidly on a GLP-1, they lose massive amounts of fluid, glycogen, and fat stored inside the muscle (a condition known as myosteatosis) 18. The SURPASS-3 MRI sub-study directly tested this and found that tirzepatide significantly reduced fatty infiltration within the muscle 18. DXA scanners record this healthy clearing of intramuscular fat as a "loss of lean mass," penalizing the drug for a highly beneficial metabolic adaptation 18.
Furthermore, functional physical data supports the preservation of actual muscle strength. In the SEMALEAN study, patients on semaglutide actually showed a 4.5 kilogram improvement in handgrip strength over 12 months, and the prevalence of sarcopenic obesity dropped from 49 percent to 33 percent 18.
Strategies for Preserving Lean Mass
While the drugs do not inherently waste muscle, rapid weight loss itself introduces nutritional vulnerabilities 432. Because appetite is so severely blunted, patients often fail to consume adequate protein or calories to maintain their muscle tissue.
To mitigate sarcopenia (muscle wasting) and optimize the quality of weight loss, clinical guidelines are emphatic: GLP-1 therapy must be paired with structured lifestyle interventions. This includes prioritizing a high-protein diet to provide the building blocks for muscle repair, and engaging in regular resistance training, which physically signals the body to preserve skeletal muscle even while operating in a severe caloric deficit 43233.
Metabolic and Systemic Benefits Beyond the Scale
For years, obesity treatment was viewed primarily through the lens of mechanical weight reduction. The advent of GLP-1s has triggered a paradigm shift in endocrinology and cardiology, proving that reducing adipose (fat) tissue directly resolves systemic inflammation and major organ disease 33.
Cardiovascular and Kidney Protection
The most monumental shift in the perception of GLP-1s came with the publication of cardiovascular outcome trials (CVOTs). The landmark SELECT trial evaluated semaglutide 2.4 mg in over 17,000 adults with established cardiovascular disease who had overweight or obesity, but not diabetes.
The trial demonstrated that semaglutide reduced the risk of major adverse cardiovascular events (MACE) - including cardiovascular death, non-fatal heart attacks, and non-fatal strokes - by a staggering 20 percent compared to standard care 2234. Furthermore, it reduced the risk of death from any cause by 19 percent 34. Notably, these cardioprotective benefits accrued regardless of the patient's baseline age, sex, or starting BMI. The exact mechanisms are believed to be multifactorial, involving reduced systemic inflammation, improved vascular resistance, and enhanced lipid profiles 3444.
Based on this data, the European Medicines Agency (EMA) and the US FDA officially updated the label for Wegovy in 2024 to include cardiovascular risk reduction, transforming it from a "weight loss drug" into a life-saving cardiovascular intervention 2235.
In addition to heart health, long-term data indicates that GLP-1 receptor agonists provide profound renal protection. These medications have been shown to reduce albuminuria (protein in the urine) and slow the decline of estimated glomerular filtration rate (eGFR), with benefits largely independent of just blood sugar or weight reduction, suggesting direct protective effects on the kidney tissue itself 44.
Heart Failure, Liver Health, and Sleep Apnea
The benefits of systemic fat reduction extend into almost every organ system. In the STEP HFpEF trials, semaglutide led to significant reductions in heart failure-related symptoms and improved physical limitations for patients with obesity-related heart failure with preserved ejection fraction 46.
For patients with metabolic dysfunction-associated steatotic liver disease (MASH), both tirzepatide and semaglutide have shown efficacy in promoting disease remission and reducing liver fat, with semaglutide showing strong evidence for improving liver fibrosis staging 3648.
Mechanically, the removal of excess weight provides immense relief to the respiratory system and joints. In the SURMOUNT-OSA trials, tirzepatide significantly reduced the severity of obstructive sleep apnea (OSA), dramatically lowering the number of breathing interruptions per hour 1148. Semaglutide is heavily recommended for patients with knee osteoarthritis due to its proven ability to reduce joint pain and mechanical strain 37.
The New Treatment Guidelines
In response to this wave of clinical data, major medical organizations updated their clinical practice guidelines in 2024 and 2025. They explicitly state that obesity management should no longer be defined merely by BMI reductions, but by a "complications-guided" approach - focusing on the prevention and resolution of fat mass diseases (like osteoarthritis and sleep apnea) and sick fat diseases (like type 2 diabetes and cardiovascular disease) 483839. Under these new frameworks, semaglutide and tirzepatide are recommended as first-line pharmacological treatments 3738.
| Organization | Key GLP-1 Guideline Updates (2024-2025) |
|---|---|
| European Association for the Study of Obesity (EASO) | Recommends semaglutide and tirzepatide as first-line therapies. Shifts focus to a "complications-guided" algorithm rather than weight loss alone. Tirzepatide preferred for sleep apnea; Semaglutide preferred for osteoarthritis 3738. |
| Obesity Canada | Recommends pharmacotherapy (including semaglutide and tirzepatide) in conjunction with individualized medical nutrition therapy provided by a registered dietitian. Strongly warns against the use of unregulated compounded medications 3940. |
| NICE (UK National Institute for Health and Care Excellence) | Recommends tirzepatide and semaglutide for adults with a BMI of 35+ and at least one weight-related comorbidity. Crucially, the BMI threshold is lowered by 2.5 kg/m2 (to 32.5) for people from South Asian, Chinese, Middle Eastern, and Black African ethnic backgrounds due to increased metabolic risks 414243. |
Managing the Side Effects and Serious Risks
While the benefits are transformative, GLP-1 medications are serious pharmacological interventions that carry a distinct side-effect profile. Regulatory bodies like the EMA explicitly state they are not approved for, and should not be used for, cosmetic weight loss in individuals who do not have clinical obesity or weight-related metabolic conditions 4445.
Gastrointestinal Realities
Because the medications act directly on the gut, gastrointestinal adverse events are the most frequent complaint 1214. In clinical settings, nausea, diarrhea, vomiting, and constipation are the primary reasons patients discontinue the medication early 1215.
However, long-term data offers reassurance. In the STEP trials, gastrointestinal symptoms peaked during the initial 20-week dose-escalation phase and declined significantly thereafter 14. By the one-year mark, the vast majority of patients reported either mild or no gastrointestinal symptoms 14. To manage this during the early months, clinicians advise eating smaller, more frequent meals, prioritizing protein, avoiding high-fat or highly processed foods that take even longer to digest, and remaining highly hydrated 1428.
Rare but Serious Risks
There are specific, rare risks that necessitate medical supervision:
- Aspiration Risk During Anesthesia: Because GLP-1s delay gastric emptying, food and liquids remain in the stomach much longer than usual. In July 2024, the European Medicines Agency's Pharmacovigilance Risk Assessment Committee (PRAC) issued new warnings regarding the risk of aspiration and aspiration pneumonia during surgeries requiring general anesthesia or deep sedation 58. Patients are now explicitly warned to inform their doctors and anesthesiologists if they are taking a GLP-1 prior to any procedure 58.
- Pancreatitis: A personal history of pancreatitis is a significant contraindication for both semaglutide and tirzepatide. Clinical trials have noted a rare but biologically plausible association between the incretin system and pancreatic inflammation 51417.
- Thyroid Tumors: In rodent studies, GLP-1 receptor agonists were associated with an increased risk of medullary thyroid carcinoma (MTC). While this has not been definitively proven in humans, the medications are strictly contraindicated for anyone with a personal or family history of MTC or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) 315.
What Happens If You Stop Taking It?
A common criticism of GLP-1 medications is that patients must take them "forever." However, obesity specialists view this not as a flaw of the drug, but as definitive proof of the chronic, biological nature of the disease 46.
The Rebound Effect
Clinical trials that involve a withdrawal phase consistently demonstrate a harsh reality: stopping the medication leads to biological regression. When the exogenous hormones are removed, gastric emptying speeds back up, and the suppression of the brain's reward centers lifts. The "food noise" returns, often intensely 5.
On average, patients who stop GLP-1 therapy regain up to two-thirds of their lost weight within the first year of discontinuation 32. Troublingly, studies suggest that the weight regained is disproportionately fat mass, meaning patients may end up with a worse body composition (higher fat-to-muscle ratio) than before they started if they are not actively strength training 32.
Metabolic markers also drift backward. A study by Epic Research analyzing over 54,000 adults with type 2 diabetes found that while some patients managed to maintain their improved HbA1c a year after stopping, 21 percent saw their blood sugar levels revert to worse than their pre-GLP-1 baseline 47.
Shifting to a Chronic Care Model
Because obesity is a chronic, relapsing disease - much like hypertension or hyperlipidemia - the medical consensus is shifting toward viewing GLP-1s as long-term, potentially lifelong therapies 343946. Just as a doctor would not stop prescribing a statin once a patient's cholesterol reaches a healthy level, ceasing an anti-obesity medication invites the underlying disease pathology to return 46.
For those who must stop due to cost, side effects, or insurance coverage, intensive nutritional programming is critical. Programs emphasizing "Food is Medicine" (FIM) interventions - focusing on high protein, high fiber, and behavioral modifications - are essential strategies to protect the investment made during the pharmacological weight loss phase and mitigate weight regain 32.
Bottom line
Starting a GLP-1 medication fundamentally alters how your brain perceives food and how your gut digests it, acting as a metabolic dimmer switch that leads to substantial weight loss and profound reductions in cardiovascular and renal risks. While concerns about muscle loss dominate public conversation, clinical data proves that these medications primarily burn fat, and lean mass can be effectively preserved with targeted protein intake and resistance training. Because these sweeping physiological benefits rely on the active presence of the drug, obesity must be managed as a chronic condition, with discontinuation typically resulting in the rapid return of cravings and the regain of weight.