Why We Get Hungry and Why Most Diets Fail
Hunger is a sophisticated evolutionary survival mechanism driven by a complex interplay of gut hormones, neurological circuits, and environmental cues designed to prevent starvation. Most acute diets fail because human physiology interprets rapid weight loss as a severe ecological threat, triggering metabolic slowdowns and intense psychological cravings that conscious discipline cannot overcome. Sustainable weight management requires abandoning rigid dietary restrictions in favor of flexible, long-term behavioral modifications and, when appropriate, medical interventions that align with human biology rather than fighting against it.
The Biological Architecture of Appetite
To understand the high failure rate of restrictive diets, it is essential to first examine the physiological origins of appetite. Hunger is not simply the physical sensation of an empty stomach, nor is overeating fundamentally a failure of moral discipline. Rather, feeding behavior is an intricately orchestrated neuroendocrine process coordinated primarily by the hypothalamus, a small region deep within the brain 12.
The hypothalamus operates as the central processing unit for energy balance. Within this region lies the arcuate nucleus, which serves as the primary appetite control center. This nucleus houses two distinct and opposing sets of primary neurons that dictate feeding behavior 23. The first set releases neurotransmitters known as Neuropeptide Y (NPY) and Agouti-related peptide (AgRP). When activated, these excitatory neurons powerfully stimulate the drive to seek and consume food 23. The second set releases pro-opiomelanocortin (POMC) and cocaine-and amphetamine-regulated transcript (CART). When stimulated, POMC is cleaved into smaller neurotransmitters, such as alpha-MSH, which inhibit the excitatory neurons and signal a state of satiety, effectively suppressing the appetite 24.
These neuronal circuits do not function in isolation. They constantly receive chemical updates from the peripheral organs, particularly the gastrointestinal tract and adipose (fat) tissues, creating a continuous, bidirectional feedback loop known as the gut-brain axis.
The Hormonal Messengers: Ghrelin, Leptin, and the Gut Axis
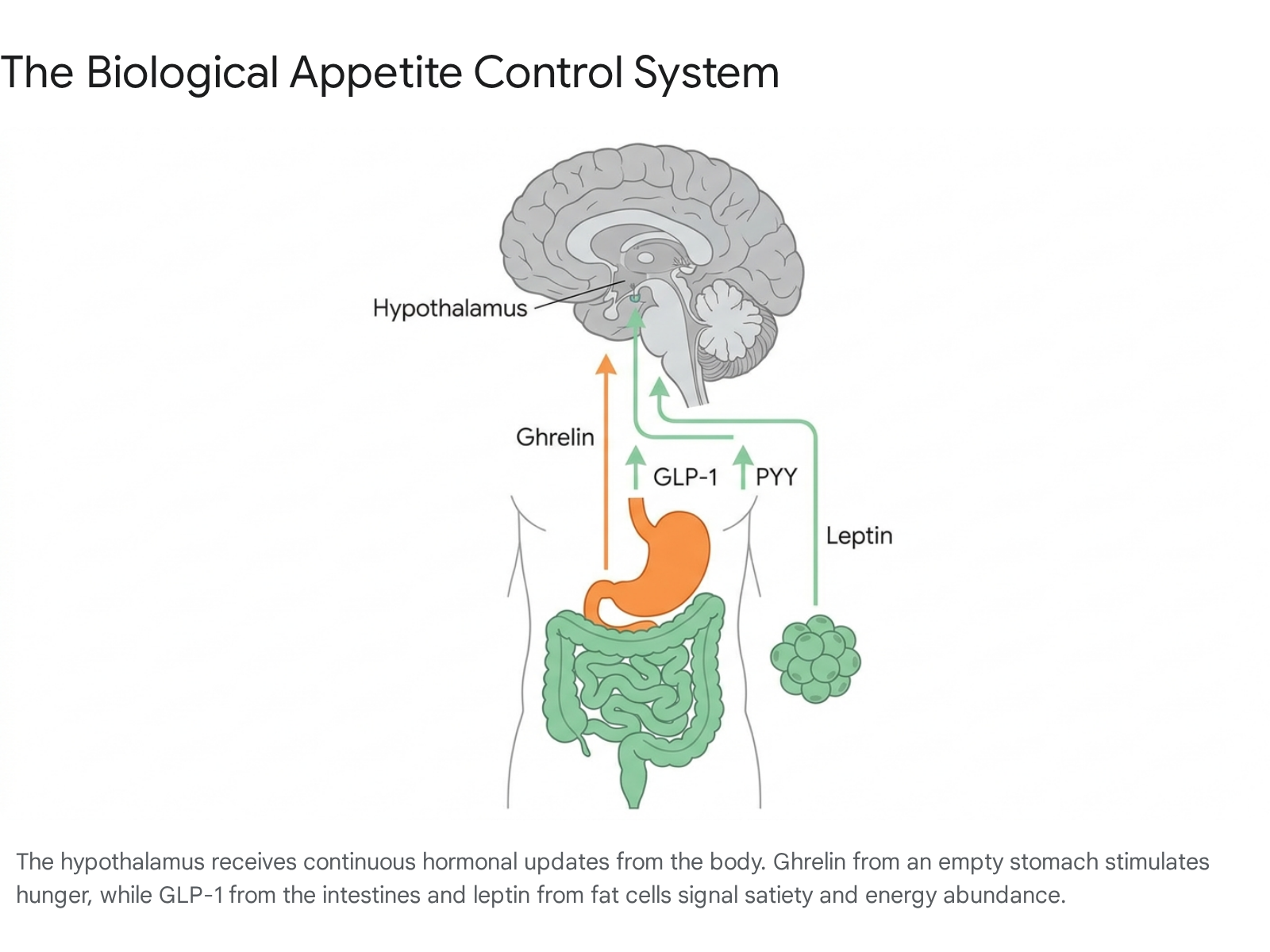
The physical sensations of hunger and fullness are dictated by a symphony of circulating hormones. When the stomach is empty, cells within the stomach wall secrete a peptide hormone called ghrelin 12. Frequently referred to as the "hunger hormone," ghrelin travels through the bloodstream to the brain, where it activates the excitatory NPY/AgRP neurons in the hypothalamus. This triggers the physical sensation of stomach contractions and initiates an intense behavioral drive to eat 124. Once food is consumed and the stomach physically expands, ghrelin concentrations drop rapidly.
Conversely, the body possesses multiple overlapping mechanisms to signal that sufficient energy has been acquired. As food enters the intestines, specialized enteroendocrine L-cells release a cascade of satiety hormones, most notably Glucagon-like peptide-1 (GLP-1), Peptide YY (PYY), and Cholecystokinin (CCK) 124. These hormones perform dual functions. Peripherally, they delay gastric emptying, ensuring that food remains in the stomach longer to prolong the physical sensation of fullness. Centrally, they travel via the bloodstream and the vagus nerve to the brainstem and the hypothalamus, where they activate the inhibitory POMC pathways and shut down the hunger signals generated by NPY neurons 24.
While gut hormones manage acute, meal-to-meal hunger, the body also meticulously monitors its long-term energy reserves through a hormone called leptin. Leptin is secreted exclusively by adipose tissue 12. The concentration of circulating leptin is directly proportional to the amount of body fat an individual carries. In a biologically optimized system, rising leptin levels inform the brain that energy stores are abundant, which suppresses the release of appetite-enhancing orexins and naturally increases energy expenditure 125.
However, this system frequently dysregulates in individuals living with obesity. Continuous overexposure to highly palatable diets can cause the hypothalamus to become resistant to leptin. Despite having elevated levels of leptin circulating in the bloodstream, the brain fails to register the signal 46. Consequently, the brain perceives the body as being in a state of starvation, maintaining high hunger levels and promoting energy conservation regardless of the physical fat stores available.
Reevaluating the Calories In, Calories Out Model
For decades, public health guidelines and the commercial diet industry have relied heavily on a fundamental rule of thermodynamics: if an individual consumes fewer calories than they expend, they will lose weight. This is widely known as the "calories in, calories out" (CICO) paradigm 789.
From a strict physics standpoint, energy balance is an undeniable reality. Energy cannot be created or destroyed. Under highly controlled conditions, such as metabolic ward studies where researchers measure every calorie consumed and burned, weight changes can be predicted with mathematical accuracy based on the imposed caloric deficit 810. However, the human body is not a closed laboratory system, nor is it a passive furnace that uniformly burns whatever fuel is provided.
The Limitations of Simple Thermodynamics
The primary failure of the CICO model in practical, free-living environments is its assumption that the "calories out" side of the equation remains static when the "calories in" side is manipulated 910. Physiology disrupts this simple arithmetic.
Recent research into evolutionary metabolism, including the "constrained energy model" proposed by researchers like Herman Pontzer, suggests that the body treats total daily energy expenditure as a constrained variable 10. When physical activity increases, the body often compensates by unconsciously reducing non-exercise movement later in the day, or by increasing appetite to match the energy burned 10.
Furthermore, the CICO model implies that all calories are metabolically equal. This has been vigorously challenged by alternative frameworks, such as the Carbohydrate-Insulin Model (CIM) 78. The CIM posits that the quality of calories profoundly influences hormonal responses. For instance, consuming calories from highly refined carbohydrates triggers a rapid spike in blood glucose, followed by a surge in insulin. Insulin promotes lipogenesis (fat storage) and inhibits the release of stored fat for energy 710. As the body rapidly stores these nutrients, circulating energy levels in the blood drop, triggering premature hunger. Thus, while the laws of thermodynamics remain intact, the hormonal environment dictated by macronutrient quality heavily influences where the energy goes and how soon hunger returns 78.
| Model | Primary Mechanism of Weight Gain | Dietary Focus | Limitations |
|---|---|---|---|
| Calories In, Calories Out (CICO) | Sustained caloric surplus. Energy intake exceeds expenditure. | Total calorie quantity; macro ratios are secondary. | Ignores biological adaptations to energy deficits and the hormonal impacts of different foods. |
| Carbohydrate-Insulin Model (CIM) | Refined carbohydrates spike insulin, driving energy into fat cells and leaving the body chemically starved. | Calorie quality; restriction of high-glycemic carbohydrates. | Isocaloric substitution studies often show minimal differences in weight loss when protein is matched. |
Metabolic Adaptation and the "Starvation" Response
When an individual drastically reduces their caloric intake to lose weight, the body does not passively burn off its fat stores to make up the difference. Instead, it perceives the sudden drop in available energy as an acute environmental threat - a famine. To ensure survival, the body automatically triggers a series of compensatory physiological responses to conserve energy, a phenomenon known as metabolic adaptation or adaptive thermogenesis 9101011.
As weight is lost, a drop in the resting metabolic rate (RMR) is expected simply because a smaller body requires less energy to function and move. However, metabolic adaptation refers to a decrease in metabolism beyond what can be accounted for by the loss of fat and fat-free mass 9101112. The body becomes ruthlessly efficient, down-regulating sympathetic nervous system activity and altering thyroid hormone production to burn fewer calories at rest 12. Simultaneously, the biological mechanisms controlling hunger escalate; leptin levels plummet as fat cells shrink, and ghrelin levels rise, leaving the individual physically hungrier and their brain's reward centers hyper-responsive to food cues 61415.
The clinical relevance of metabolic adaptation remains one of the most vigorously debated topics in nutritional science. Some highly publicized studies, such as those tracking former contestants of The Biggest Loser, observed severe metabolic slowdowns that persisted for years, contributing to massive weight regain 10. Conversely, researchers like Dr. Cátia Martins at the University of Alabama at Birmingham have published compelling evidence suggesting the magnitude of metabolic adaptation is often exaggerated 101113.
Martins' research demonstrates that when measurements are taken after a period of weight stabilization - rather than during active, aggressive weight loss - the metabolic adaptation at the level of RMR averages only about 50 to 90 calories per day 1114. Furthermore, her longitudinal studies have shown that the magnitude of a patient's metabolic adaptation does not reliably predict long-term weight regain 101115. This suggests that while the body does actively resist weight loss, the failure of long-term weight maintenance is likely driven more by the relentless neurological increase in appetite and behavioral fatigue than by a permanently damaged metabolism 1316.
The Physics of Weight: Set Point vs. Settling Point
The biological pushback against weight loss has led researchers to investigate precisely how the human body determines its ideal size. For decades, the dominant paradigm was the "set point" theory, though an updated "settling point" theory is increasingly favored to explain modern obesity trends 2017.
The Traditional Set Point Theory
First conceptualized in the 1950s, the set point theory posits that each individual possesses a biologically predetermined, genetically hardwired weight range 617. The hypothalamus acts much like a home thermostat: if an individual's weight drops below their set point, the metabolic furnace turns down and hunger turns up until the original baseline is restored. If their weight drifts above the set point, appetite should ideally decrease and energy expenditure increase 617.
This regulatory system expertly explains why dieting is so difficult and why rapid weight loss triggers immediate hormonal alarms. However, the strict set point theory fails to adequately explain the global obesity epidemic 1718. If biological set points are genetically fixed, the average weight of entire populations could not have surged as dramatically as it has over the last forty years.
The Settling Point and Dual-Intervention Models
In response to these limitations, researchers proposed the "settling point" theory. This model suggests that there is no rigid, predetermined internal thermostat. Instead, body weight is viewed as a passive equilibrium - it "settles" at a point dictated by the constant interaction between an individual's biology and their external environment 12201718.
A common analogy compares the settling point to the water level of a lake. The water level is determined by the balance of rainfall (caloric intake) and drainage (energy expenditure). If rainfall increases due to a highly processed food environment, the lake settles at a new, higher level 18. If the environment changes - for example, shifting from a highly active lifestyle to a sedentary desk job - the body's weight will naturally drift and settle at a higher equilibrium 18.
| Feature | Set Point Theory | Settling Point Theory |
|---|---|---|
| Core Concept | Weight is actively defended at a rigid, genetically predetermined value. | Weight passively stabilizes where biological traits meet environmental habits. |
| Analogy | A thermostat actively regulating room temperature. | A lake's water level determined by rainfall and drainage. |
| Response to Dieting | The body actively fights to return exactly to the original starting weight. | Weight can stabilize at a new, lower level if the new environment is permanently sustained. |
| Explanation for Obesity | Assumes the biological "thermostat" becomes broken or pathologically elevated. | Acknowledges that highly processed, calorie-dense environments naturally push the equilibrium higher. |
Some modern researchers merge these concepts into a "dual-intervention point" model. This theory proposes that individuals possess a "zone of indifference" - an upper and lower threshold defining acceptable body weight 618. Within this zone, settling point concepts prevail, and the body easily adapts to environmental changes. However, if body weight falls below the lower threshold, it triggers ancient physiological mechanisms to defend against starvation, aggressively increasing appetite and reducing energy expenditure 618.
The critical takeaway from the settling point model is that an individual's baseline weight is not irrevocably fixed 1219. However, lowering a settled weight requires immense patience. Crash diets guarantee a physiological rebound because they force the body below its starvation threshold 2021. To establish a new, lower settling point, weight loss must be gradual, and the new lifestyle behaviors must be maintained for months to years to allow hormonal signaling to fully normalize 2126.
The Psychological Mechanics of Dieting Failure
The biological defense mechanisms against weight loss are formidable, but they are frequently exacerbated by the psychological tactics individuals use to diet. Society has historically framed weight management as a test of moral character, promoting the stigmatizing narrative that a lack of discipline is the primary cause of obesity 91422. This perspective is not only scientifically inaccurate, but it actively sabotages long-term success.
The Debunked Myth of Willpower and Ego Depletion
For years, the diet industry promoted the concept of "ego depletion" - the psychological theory that willpower is a finite mental muscle that becomes fatigued with use throughout the day. Under this model, individuals fail their diets in the evening because they have exhausted their self-control.
However, modern psychological research has largely debunked this concept. Recent systematic reviews and massive meta-analyses involving thousands of participants have found that the evidence for a robust ego depletion effect is incredibly weak, with effect sizes approaching zero 28. Relying on willpower to ignore chronic hunger is a fundamentally flawed strategy because human biology is explicitly designed to override conscious resolve when energy stores are threatened 28. By heavily restricting calories, dieters exchange automatic, internal regulators of appetite for conscious, mental ones. Eventually, the biological imperative to survive overwhelms the cognitive desire to lose weight 1023.
Furthermore, the stigma generated by the "willpower myth" inflicts physiological harm. Research indicates that experiencing weight discrimination triggers the release of cortisol, the body's primary stress hormone. Chronic cortisol elevation is directly linked to increased visceral fat storage and heightened cravings for high-sugar, energy-dense comfort foods 14.
Rigid Restraint vs. Flexible Restraint
Clinical psychologists differentiate between two distinct behavioral approaches to dieting: rigid restraint and flexible restraint.
Rigid restraint is characterized by dichotomous, black-and-white rules. Foods are categorized strictly as "good" or "bad," and the dietary plan operates on an all-or-nothing mentality 1424. This approach frequently triggers what psychologists term the "abstinence violation effect" 14. Under a rigid framework, eating a single unauthorized food item (e.g., a biscuit) is interpreted as a total failure. This leads to a collapse in self-efficacy, subsequent feelings of intense guilt, and "disinhibited eating," where the individual abandons the plan entirely and consumes vast quantities of the restricted food 142526.
Flexible restraint, conversely, involves a more moderate approach to food regulation. It allows for the occasional consumption of all foods without guilt or compensatory punishment, and acknowledges slip-ups without framing them as failures 142527. Clinical studies show that while both rigid and flexible dieting can produce initial scale weight loss, flexible restraint is statistically far more successful for long-term weight maintenance 2728. It facilitates higher levels of self-regulation, significantly reduces the frequency of binge eating episodes, and mitigates the psychological fatigue that typically derails strict diets 252627.
The Default Mode Network and "Food Noise"
One of the most debilitating psychological aspects of chronic dieting is the emergence of "food noise." This phenomenon involves constant, intrusive, background rumination about food - obsessively planning the next meal, tracking calories, or fighting relentless cravings 352930.
Food noise is not a character flaw; emerging neurological research suggests it is a measurable cognitive phenomenon. It appears linked to the brain's Default Mode Network (DMN), a neural system associated with internal rumination and prospection (the mental simulation of future events) 30. In the context of a caloric deficit, food noise acts as a form of maladaptive prospection. The brain amplifies the salience of food cues in the environment, leading to repetitive, cue-elicited simulations of short-term rewards (eating) that constantly interfere with the individual's long-term health goals 30. When the body senses starvation, the DMN ensures that the acquisition of food remains the brain's highest cognitive priority.
Environmental and Cultural Drivers of Obesity
While internal biology dictates how weight is gained and defended, it does not fully explain why obesity has become a sudden global crisis. The answer lies in the intersection of ancient human physiology and the modern environment. Public health experts frequently describe modern societies as "obesogenic" - structurally engineered for over-consumption and minimal physical exertion 1438.
The Ultra-Processed Food Environment
The contemporary food supply is fundamentally different from the diets human ancestors consumed. A significant portion of the modern diet consists of ultra-processed foods (UPFs). These products are industrially engineered to achieve a "bliss point," combining optimal ratios of refined sugars, fats, and sodium to maximize palatability and bypass the brain's natural satiety signals 353132.
Because UPFs often lack dietary fiber and complex cellular structures, they are digested and absorbed exceptionally rapidly. This causes sharp spikes in blood glucose and subsequent surges in insulin 47. Furthermore, this rapid absorption means the lower gastrointestinal tract does not have sufficient time or volume to release adequate amounts of satiety hormones like GLP-1 and PYY. Consequently, an individual can consume a massive caloric load of UPFs and find themselves chemically hungry again shortly afterward 4.
Socioeconomic disparities heavily compound this issue. Healthier, minimally processed foods are frequently more expensive per calorie than highly processed alternatives. In many nations, obesity is heavily concentrated in lower-income demographics, where the high cost of fresh produce, combined with the psychological stress of poverty (a "scarcity mindset"), creates an environment where prioritizing energy-dense, cheap food becomes a survival necessity 143342.
Global Dietary Shifts: Latin America and Africa
The impact of the obesogenic environment is not confined to Western nations. Traditional, sustainable dietary patterns - such as the Mediterranean diet, which emphasizes whole grains, healthy fats, and lean proteins - are experiencing declining adherence globally, even within their regions of origin 344435.
Simultaneously, low- and middle-income countries are undergoing a rapid "nutrition transition." As globalization introduces Western-style UPFs into regions like Latin America and Africa, traditional dietary practices are being displaced 383647. This shift has resulted in soaring rates of obesity and metabolic syndrome. Strikingly, these regions often face a "double burden" of malnutrition, where severe undernutrition (stunting and thinness) coexists within the same communities - and sometimes the same households - as severe obesity 473738. In Latin America, adherence to sustainable diets like the EAT-Lancet planetary health diet is critically low, particularly in urban areas where UPF consumption is highest 3650.
The South Asian Phenotype and the Limits of BMI
The global nutrition transition has also revealed unique geographic and genetic vulnerabilities to modern diets. In South Asia, populations frequently exhibit a distinct "thin-fat" phenotype 3940.
South Asian individuals tend to accumulate highly inflammatory visceral (abdominal) fat and ectopic fat in organs like the liver, while simultaneously presenting with lower skeletal muscle mass 4041. Crucially, this metabolic dysfunction occurs at much lower Body Mass Index (BMI) thresholds compared to White or Western populations 4041. A South Asian individual with a "normal" BMI may possess the same risk for Type 2 diabetes and cardiovascular disease as a Western individual classified as obese. This phenomenon underscores that standard BMI metrics are often insufficient for accurately assessing metabolic health across diverse global populations, necessitating more culturally and genetically tailored screening approaches 4154.
Pharmacological Innovations: The Incretin Revolution
The scientific recognition that obesity is a chronic disease driven by biological, neurological, and environmental factors - rather than a failure of willpower - has led to a revolution in medical treatment. The emergence of incretin-mimetic medications, primarily GLP-1 receptor agonists, has fundamentally altered the obesity management landscape 424344.
Mechanisms of GLP-1, GIP, and Glucagon Agonists
Originally developed to manage Type 2 diabetes, medications such as semaglutide, tirzepatide, and the investigational drug retatrutide mimic the natural satiety hormones produced in the gut 2943. By delivering these hormones at higher, more sustained levels than the body naturally produces, they initiate a profound biological shift.
Peripherally, these medications slow gastric emptying, ensuring that food remains in the stomach longer and prolonging the physical sensation of fullness 42943. They also enhance glucose-dependent insulin secretion, stabilizing blood sugar levels and preventing the crashes that often trigger cravings for refined carbohydrates 2943.
However, their most revolutionary impact occurs centrally. These medications cross the blood-brain barrier and bind directly to receptors in the hypothalamus, down-regulating the biological drive to eat 32942. Recent studies utilizing fluorescence imaging in brain tissue reveal that these drugs increase levels of a signaling molecule called cyclic adenosine monophosphate (cAMP) inside appetite-regulating neurons, effectively silencing hunger signals at a cellular level 4245.
Rewiring Food Noise and the Brain's Reward Circuitry
Beyond simple physical fullness, incretin medications appear to modulate the brain's reward processing. Advanced neuroimaging and animal models demonstrate that these drugs penetrate deeper into the brain than previously understood, reaching regions like the central amygdala 4647.
By acting on these emotional and reward-processing centers, GLP-1 medications reduce the dopamine release typically associated with eating highly palatable foods 464761. For patients, this translates into a sudden cessation of "food noise." The relentless neurological rumination about food quiets down, and the compulsion to binge eat is significantly diminished 304361. The medications appear to shift the balance of activity within the Default Mode Network, correcting the maladaptive prospection that makes dieting so psychologically exhausting 30.
Clinical Efficacy and Next-Generation Therapies
The efficacy of these pharmacological interventions is unprecedented in the history of obesity medicine, with each new generation of drugs showing increased potency by targeting multiple hormone receptors simultaneously.
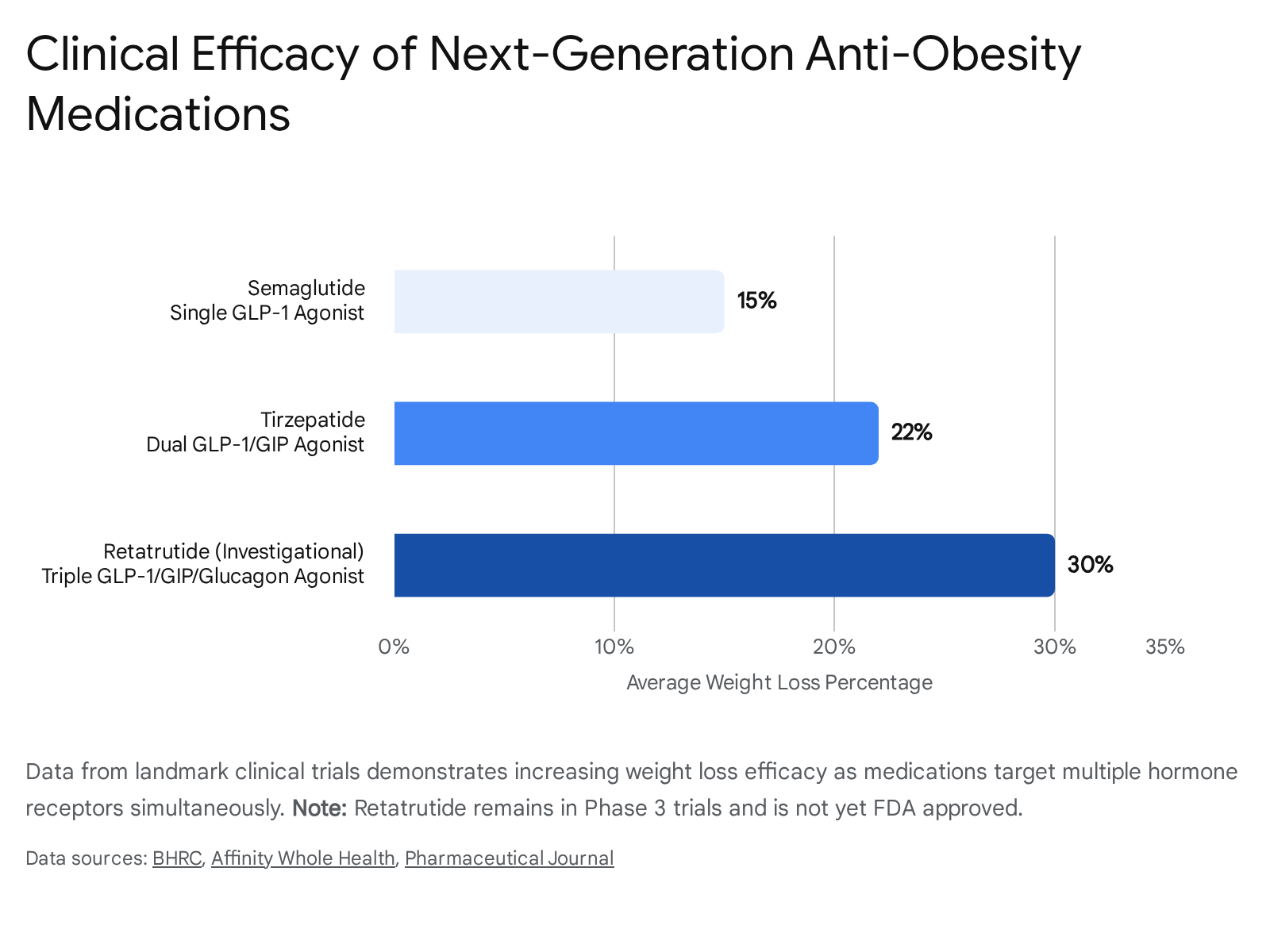
Despite their success, these medications highlight a critical clinical reality: obesity requires chronic management. Systematic reviews overwhelmingly confirm that if a patient discontinues incretin therapy, the suppressed appetite returns, metabolic adaptations persist, and weight is almost universally regained within a year or two 1648.
Furthermore, rapid pharmacological weight loss brings the risk of excessive muscle loss (fat-free mass loss), which can compromise long-term metabolic health and functional capacity if not paired with appropriate exercise and nutritional interventions 16.
Evidence-Based Strategies for Long-Term Maintenance
Understanding the complex biology of hunger makes it evident why short-term, acute restrictive diets fail 2049. Successful long-term weight management requires shifting the focus from rapid scale changes to sustainable physiological and behavioral modifications.
Data from the National Weight Control Registry, which tracks individuals who have successfully maintained significant weight loss for over five years, reveals that success is not achieved through perpetual starvation. Instead, successful maintainers rely on consistency, structure, and managing their environment 6465.
Transitioning from Acute Restriction to Nutritional Density
Rather than focusing entirely on caloric deficits, evidence-based management emphasizes nutrient density. Diets high in lean protein, dietary fiber, and whole foods naturally delay gastric emptying and stimulate the endogenous release of GLP-1 and PYY 41950. This nutritional profile keeps hunger at bay and stabilizes blood glucose without requiring intense psychological willpower.
Similarly, dietary guidelines are increasingly recognizing that total dietary flexibility is vital. Implementing sustainable eating patterns that allow for occasional indulgences prevents the psychological burnout and binge-eating episodes characteristic of rigid crash diets 2027.
The Importance of Resistance Training and Sleep
Because weight loss inevitably results in some loss of fat-free mass, incorporating resistance training is paramount. Building and preserving muscle tissue helps maintain the resting metabolic rate, providing a buffer against the metabolic adaptations that drive weight regain 161927.
Additionally, systemic lifestyle factors play a direct role in hormonal regulation. Chronic stress and sleep deprivation elevate cortisol and disrupt the delicate balance of leptin and ghrelin. Ensuring 7 to 9 hours of quality sleep and managing psychological stress are not secondary concerns; they are primary biological requirements for functional appetite control 141951.
Redesigning Primary Care Interventions
Finally, the medical community is recognizing that advising patients to simply "eat less and move more" is an insufficient standard of care. Innovative programs, such as the PATHWEIGH initiative implemented in primary care clinics, provide patients with structured, dedicated weight-care visits that address the biological and environmental complexities of obesity 52. By offering judgment-free medical support, personalized interventions, and appropriate pharmacotherapy, health systems are beginning to successfully halt population-level weight gain 4452.
Bottom line
Human hunger is driven by an incredibly efficient, overlapping system of brain circuits and gut hormones designed by evolution to defend body weight and prevent starvation. Most diets fail because acute caloric restriction triggers metabolic slowdowns, spikes hunger hormones, and amplifies neurological "food noise," creating a physiological resistance that willpower alone cannot defeat. Achieving long-term weight management requires shifting away from rigid, short-term diets toward flexible, sustainable nutritional habits, resistance training, and, when clinically indicated, medical interventions that treat obesity as a chronic, biological condition.