Why Stress Makes It Hard to Fall Asleep
At a biological level, stress blocks sleep by activating the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system, flooding the bloodstream with corticotropin-releasing hormone, adrenaline, and cortisol. This neuroendocrine cascade evolved to prioritize immediate survival over restorative processes, artificially elevating the heart rate, increasing core body temperature, and suppressing sleep-inducing neurotransmitters. Consequently, the brain's hyperarousal mechanisms forcibly override the homeostatic sleep drive, rendering the transition into unconsciousness physiologically impossible until the perceived threat has passed.
It is 2:00 AM. The environment is completely silent, the lights are extinguished, and the physical exhaustion from a demanding day is palpable in every muscle. Yet, staring up at the dark ceiling, the mind races at a relentless, uncontrollable pace. The heart beats just a fraction too hard against the mattress, breathing feels shallow, and a pervasive, vibrating alertness makes the very idea of sleep feel like an impossible task. This infuriating paradox - being physically exhausted but mentally electrified - is not a personal failing, a lack of willpower, or a psychological weakness. It is the result of millions of years of evolutionary hardwiring functioning exactly as it was designed to. When modern psychological stressors hijack ancient biological survival circuits, the body prepares to fight a predator rather than drift into restorative sleep.
This comprehensive report delves into the intricate biological mechanisms of stress-induced sleep latency, breaking down the complex endocrinology of systemic hyperarousal. By debunking pervasive cultural misconceptions and examining the latest cross-cultural epidemiological research from 2023 to 2025, this analysis provides an evidence-based roadmap for downregulating the nervous system and closing the physiological gap between exhaustion and clinical sleep onset.
Why does my brain wake up the second my head hits the pillow?
The phenomenon of the brain seemingly "turning on" the moment an individual lies down is deeply rooted in the mechanics of sensory gating and the autonomic nervous system. Throughout the waking hours, the brain is continuously bombarded with external stimuli - work demands, complex social interactions, digital notifications, auditory processing, and physical movement. This constant stream of exogenous data occupies the brain's processing capacity, effectively masking the internal physiological signals of stress.
However, when an individual transitions to the bedroom and lies down in a dark, quiet environment, this external sensory input is abruptly and completely cut off. Without environmental distractions, the brain turns its attention inward, amplifying the perception of internal somatic states 12. If the sympathetic nervous system (the body's "fight-or-flight" mechanism) has been subtly activated all day by chronic psychological stress, the sudden quiet acts as an amplifier for the biological alarm bells that were previously drowned out by the noise of daily life.
To utilize an accessible analogy, imagine a residential smoke detector equipped with a low-battery chirp. During a loud, bustling afternoon gathering, the chirp is entirely inaudible, masked by the ambient noise of conversation and activity. But once the guests depart and the house falls completely silent in the evening, that exact same chirp becomes deafeningly loud and impossible to ignore. Similarly, the moment the head hits the pillow, the sudden environmental quiet forces the brain to register the elevated circulating cortisol levels, widespread muscle tension, and rapid heart rate that it had been successfully ignoring all day.
Furthermore, this sudden influx of unfiltered psychological distress frequently triggers cognitive rumination. Clinical studies and psychological evaluations consistently demonstrate that the act of ruminating on stressful events - rather than the severity of the events themselves - is a primary driver of prolonged sleep onset latency (the specific metric measuring the time it takes to transition from full wakefulness to stage 1 non-rapid eye movement sleep) 21. The brain interprets this intense cognitive spinning as a literal, physical threat, signaling the adrenal glands to release additional alertness-promoting hormones. This creates a vicious, self-sustaining feedback loop of nocturnal wakefulness where the anxiety of not sleeping further delays sleep onset.
What does tired but wired actually mean biologically?
The ubiquitous sensation of feeling "tired but wired" represents a fierce physiological tug-of-war between two distinct, opposing biological systems: the homeostatic sleep drive and the stress response system.
The "tired" aspect is driven by sleep homeostasis and cellular metabolism. Throughout waking hours, the brain continuously consumes energy (adenosine triphosphate, or ATP) and produces a metabolic byproduct known as adenosine. As adenosine accumulates in the brain's basal forebrain throughout the day, it binds to specific neural receptors, creating what sleep scientists refer to as "sleep pressure." The longer a person remains awake, the heavier this biochemical pressure becomes, eventually manifesting as profound physical exhaustion and noticeable cognitive fatigue 1.
The "wired" aspect, however, is dictated entirely by the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system. When the brain detects a stressor - whether a real physical danger, an abstract psychological worry, or anticipation of an upcoming deadline - it triggers a systemic alarm. This alarm floods the systemic circulation with glucocorticoids (primarily cortisol) and catecholamines (like adrenaline and noradrenaline). These potent chemicals evolved to execute immediate, life-saving actions: they dramatically raise the resting heart rate, shunt blood away from the digestive tract and toward major skeletal muscles, and increase blood glucose levels to provide quick energy 2236.
When an individual is "tired but wired," they simultaneously possess high adenosine levels (representing a cellular craving for sleep) alongside high cortisol and adrenaline levels (enforcing strict wakefulness). The evolutionary hierarchy of human biology dictates that acute survival always supersedes recovery. Therefore, the HPA axis effectively places a dominant chemical block on the homeostatic sleep drive. The physiological system cannot and will not allow the extreme vulnerability of sleep while it genuinely believes a predator is nearby - even if that modern "predator" is merely financial anxiety or workplace stress 14.
The Clinical Assessment of Sleep Latency and Reactivity
To fully grasp how stress blocks sleep, it is necessary to understand how sleep disruptions are measured in clinical and research settings. Sleep latency, explicitly defined as the total time required to transition from full wakefulness to the first epoch of sleep, is a critical indicator of sleep quality and a highly sensitive biomarker for stress 56. Healthy, unstressed individuals typically fall asleep within 10 to 20 minutes 5.
Recent developments in sleep medicine have highlighted a specific trait known as "sleep reactivity," which dictates the degree to which stress exposure disrupts an individual's sleep system 1. Highly reactive individuals experience drastic, immediate deteriorations in sleep onset latency when stressed, whereas individuals with low sleep reactivity proceed largely unperturbed by similar stressors 17. This trait is not purely psychological; it has deep neurobiological underpinnings involving genetic predispositions, disrupted cortical networks, and autonomic nervous system dysregulation. Notably, highly reactive sleepers exhibit significant decreases in rapid eye movement (REM) sleep duration and increased nocturnal arousals during stress, whereas low-reactive sleepers maintain stable REM architecture 1.
Furthermore, objective measurement devices (such as polysomnography or actigraphy) frequently reveal a phenomenon known as "sleep misperception" or subjective-objective sleep discrepancy. Individuals suffering from severe stress and insomnia frequently overestimate their sleep latency, reporting that they lay awake for hours, whereas objective metrics indicate they were actually experiencing light, fragmented sleep 8. This discrepancy underscores how stress creates a persistent state of hyperarousal that prevents the deep, restorative stages of sleep, leaving the brain feeling as though it never truly shut down.
The HPA Axis: The Body's Biological Alarm System
To understand the exact mechanics of how stress dismantles sleep architecture, one must examine the HPA axis in detail. The HPA axis functions much like a highly sophisticated, multi-tiered commercial fire alarm and sprinkler system, operating across different regions of the brain and body.
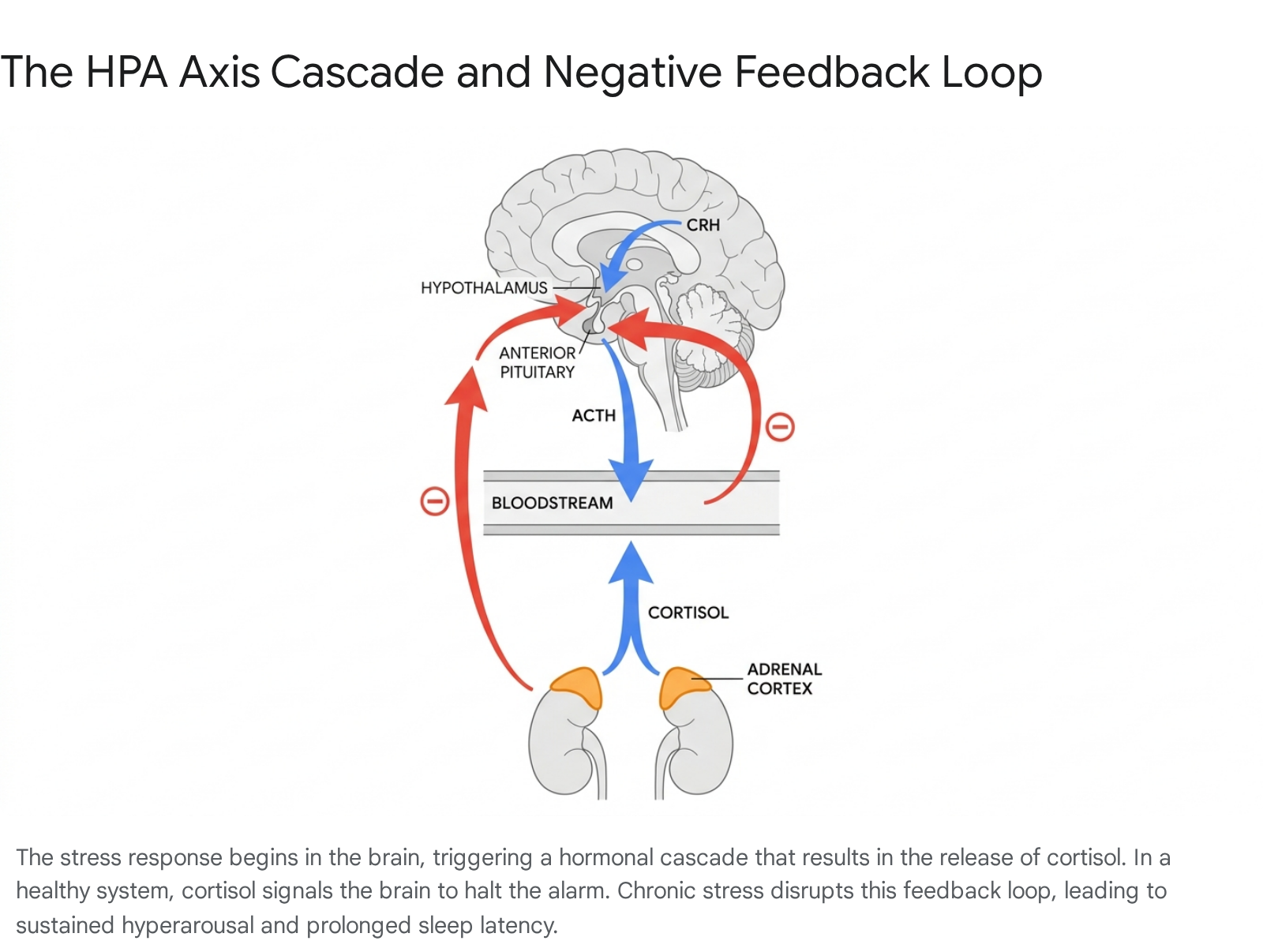
The process begins in the amygdala, which acts as the brain's internal smoke detector, constantly scanning the environment for threats. When it detects danger, it sends a high-priority distress signal to the hypothalamus, the brain's master command center 1213. In response, parvocellular neurosecretory cells within the hypothalamus release Corticotropin-Releasing Hormone (CRH) into the hypophyseal portal circulation. CRH serves as the initial chemical alarm bell, signaling that the entire body must mobilize for action 4149.
CRH travels a very short distance to the anterior pituitary gland. Upon receiving the CRH signal, the pituitary gland synthesizes and releases Adrenocorticotropic Hormone (ACTH) directly into the general bloodstream 131416. ACTH then travels systematically down to the adrenal glands, which are located superior to the kidneys. The adrenal cortex (specifically the zona fasciculata) responds to ACTH stimulation by manufacturing and pumping cortisol into the blood 131610. Cortisol then binds to glucocorticoid receptors located throughout the entire body, aggressively raising alertness, increasing metabolic rate, and halting sleep induction.
In a healthy, homeostatic system, there is a built-in shut-off mechanism known as the negative feedback loop. Cortisol eventually travels back across the blood-brain barrier. Glucocorticoid receptors located in the hippocampus and the hypothalamus detect these high circulating cortisol levels and signal the system to stop producing further CRH and ACTH. This negative feedback loop is the physiological equivalent of turning off the sprinklers once a fire has been extinguished, allowing the body to return to a baseline parasympathetic state where restorative sleep is finally possible 1491611.
Step-by-Step Textual Flowchart of the HPA-Axis Cascade
To clearly map this biological process without relying on sparse bulleted lists, the sequential neuroendocrine cascade is detailed in the structured table below. This progression highlights the exact pathway from threat perception to systemic hyperarousal.
| Sequence | Biological Phase | Anatomical Location | Primary Mechanism and Hormonal Action |
|---|---|---|---|
| Step 1 | Threat Perception | Amygdala | The brain identifies a psychological or physical stressor (e.g., financial worry, a looming deadline, interpersonal conflict) and signals distress. |
| Step 2 | Hypothalamic Activation | Hypothalamus | Parvocellular neurosecretory cells secrete Corticotropin-Releasing Hormone (CRH) into the specialized capillary system. |
| Step 3 | Pituitary Stimulation | Anterior Pituitary Gland | CRH binds to specific receptors, triggering the rapid synthesis and secretion of Adrenocorticotropic Hormone (ACTH). |
| Step 4 | Adrenal Cortisol Release | Adrenal Cortex | ACTH travels via systemic circulation to the zona fasciculata of the adrenal glands, stimulating the release of glucocorticoids, primarily cortisol. |
| Step 5 | Systemic Hyperarousal | Systemic / Whole Body | Cortisol binds to widespread glucocorticoid receptors, mobilizing glucose, increasing cardiovascular tone, and chemically inhibiting sleep-promoting neurobiology. |
| Step 6 | Negative Feedback Inhibition | Hippocampus & Hypothalamus | Circulating cortisol crosses the blood-brain barrier, binding to central receptors to suppress further release of CRH and ACTH, attempting to restore homeostasis. |
Note on Pathology: In cases of chronic, unrelenting stress, the continuous bombardment of high cortisol levels physically damages the glucocorticoid receptors in the hippocampus. This damage blunts or entirely breaks the negative feedback loop. Consequently, the "shut-off valve" fails, leaving the body in a perpetual state of hyperarousal that clinically manifests as chronic sleep onset insomnia and sleep fragmentation 1610.
Correcting Common Misconceptions About Stress and Sleep
The broad landscape of sleep medicine is heavily clouded by pervasive cultural myths that consistently exacerbate insomnia. Addressing these misconceptions with rigorous clinical evidence is absolutely critical for implementing effective, long-term sleep interventions.
Misconception 1: "Stress is all in your head"
A highly prevalent and damaging myth is that stress-induced insomnia is purely a psychological issue - that if an individual could simply "think positive thoughts," "stop worrying," or "calm down," restorative sleep would immediately arrive. In stark clinical reality, stress is a deeply systemic, biological phenomenon with measurable, objective physiological biomarkers that circulate throughout the entire body.
When acute or chronic psychological stress occurs, the autonomic nervous system directly activates specific genes responsible for producing pro-inflammatory immune substances, known as cytokines 212. Sleep deprivation and stress dramatically elevate circulating levels of C-reactive protein (CRP), Interleukin-6 (IL-6), Interleukin-1 beta (IL-1β), and Tumor Necrosis Factor-alpha (TNF-α) 4131422.
This relationship is aggressively reciprocal: stress induces systemic inflammation, and systemic inflammation directly degrades the neurological architecture of sleep. Elevated daytime hypersecretion of IL-6 is strongly associated with prolonged sleep latency, chronic daytime fatigue, and severely fragmented nocturnal sleep 4. A robust meta-analytic review of over 70 clinical studies confirmed a highly consistent association between sleep disturbances and elevated circulating inflammatory markers, demonstrating unequivocally that stress leaves a tangible, toxic footprint in the blood 13. Data from the comprehensive POPPY-Sleep substudy, which utilized advanced bioassays to quantify 31 biomarkers across 8 distinct inflammatory pathways, further highlighted the sheer immunologic complexity of stress-induced sleep loss 13. Telling a stressed individual that their severe insomnia is merely "all in their head" completely ignores the proven clinical reality of their inflamed, biochemically altered central nervous system.
Misconception 2: "Alcohol effectively overrides stress-induced wakefulness"
Because stress causes systemic hyperarousal and muscle tension, many individuals attempt to force the nervous system into submission using central nervous system depressants, primarily alcohol. It is a deeply entrenched cultural belief that a "nightcap" is an effective, accessible tool for overcoming stress-induced sleep latency.
Biologically, alcohol acts as a powerful agonist for Gamma-aminobutyric acid (GABA), the brain's primary inhibitory neurotransmitter. Consuming alcohol does indeed decrease initial sleep onset latency; it artificially suppresses the firing of cortical neurons and forcibly sedates the brain, helping an individual lose consciousness much faster than they would naturally.
However, clinical sedation is fundamentally not sleep. While alcohol forces the brain into early slow-wave sleep, it severely suppresses Rapid Eye Movement (REM) sleep, a phase that is absolutely critical for emotional regulation, memory consolidation, and cognitive processing 615. More destructively, as the liver metabolizes the alcohol during the night, the brain experiences a profound "glutamate rebound." Glutamate, a highly excitatory neurotransmitter, surges rapidly as the alcohol wears off. This sudden chemical shift leads to immediate sympathetic nervous system activation, a highly elevated heart rate, increased core body temperature, and physical sweating. This physiological rebound results in severe sleep fragmentation, frequent nocturnal micro-arousals, and premature awakening in the second half of the night 615. Ultimately, alcohol does not resolve stress-induced wakefulness; it merely delays the hyperarousal by a few hours while completely destroying the restorative architectural integrity of the sleep cycle.
Acute vs. Chronic Stress: Divergent Sleep Disruptions
While both acute and chronic stress reliably disrupt sleep, they do so through fundamentally different neurobiological mechanisms, structural brain alterations, and biochemical pathways. Understanding this clinical distinction is vital, as the therapeutic interventions required for a single highly stressful day differ vastly from the systemic interventions required for months of unyielding burnout.
The comparative table below outlines the specific divergences in how acute and chronic stress disrupt the human sleep system.
| Physiological Feature | Acute Stress Mechanisms | Chronic Stress Mechanisms |
|---|---|---|
| Primary Clinical Trigger | A sudden, transient event (e.g., an interpersonal argument, a sudden workplace deadline, an acute physical threat) 112. | Prolonged, unyielding pressure without resolution (e.g., a toxic work environment, long-term financial strain, intensive caregiving) 12. |
| Brain Region Impact & Structure | Causes transient prefrontal-amygdala decoupling. Temporarily impairs "cool" executive functions such as working memory and cognitive flexibility 12. | Induces severe structural changes; prolonged high cortisol exposure leads to hippocampal atrophy, synaptic dysfunction, and sustained amygdala hypertrophy 121610. |
| HPA Axis Dynamics | Generates a rapid, adaptive spike in CRH, ACTH, and cortisol. The negative feedback loop remains perfectly intact and shuts off the hormonal response once the immediate threat passes 1416. | Results in dangerous glucocorticoid resistance. The negative feedback loop is broken or severely blunted due to receptor damage. Cortisol remains perpetually elevated 1610. |
| Sleep Architecture Disruptions | Specifically targets and prolongs sleep onset latency. May cause a transient reduction in total REM sleep strictly for the specific night immediately following the stressor 12. | Profoundly disrupts overall sleep continuity. Causes widespread sleep fragmentation, severe reductions in slow-wave (deep) sleep, and significantly heightened nocturnal arousals 216. |
| Metabolic & Immune Biomarkers | Results in temporary spikes in plasma insulin and glucose levels. Causes a temporary, adaptive shift in white blood cell distribution 314. | Drives sustained systemic neuroinflammation. Increases blood-brain barrier permeability, maintains chronic elevation of IL-6 and CRP, and significantly increases adrenal gland weight 31222. |
| Sleep Reactivity Response | Highly dependent on individual trait-level sleep reactivity. Highly reactive individuals experience severe single-night insomnia, while low-reactive individuals may sleep normally 17. | Creates a maladaptive, vicious cycle: chronic stress causes severe insomnia, and chronic insomnia acts as a systemic biological stressor that further upregulates the HPA system 212. |
Recent Breakthroughs in Sleep Latency Research (2023 - 2025)
The study of sleep latency has seen significant, paradigm-shifting advancements recently, particularly regarding the intersection of neurobiology, cultural sociology, and spatial epidemiology. Recent data indicates that clinical assessments must look far beyond the isolated individual biology and meticulously evaluate systemic, geographic, and cultural environments to understand the root causes of sleep disruption.
The Role of Cultural Coping Mechanisms
A major paradigm shift in modern sleep research involves understanding how the broad cultural dimensions of Individualism versus Collectivism dictate the biological stress response, which in turn profoundly impacts sleep architecture and latency.
Individualistic cultures (predominantly found in the United States and Western Europe) highly emphasize personal agency, autonomy, distinct uniqueness, and aggressively altering one's environment to suit individual needs. Conversely, collectivist cultures (predominantly found in East Asia and parts of the Global South) prioritize group harmony, social interdependence, and internal emotional adaptation to external realities 25172728.
Recent global bio-data and cross-cultural longitudinal studies reveal startling physiological disparities between these groups when faced with standard psychosocial stress. When individuals from individualistic societies experience stress - particularly situations involving social exclusion, a lack of control, or a loss of personal agency - they exhibit immediate, extreme high-arousal physiological responses. This includes sharp, measurable spikes in heart rate and rapid elevations in circulating cortisol 2818. Individualists are far more likely to externalize stress but suffer significantly higher levels of cardiovascular and HPA-axis reactivity as a consequence of blocked autonomy 2728.
In stark contrast, individuals from collectivist cultures tend to heavily rely on secondary control coping mechanisms. These include silent internal emotion regulation, cognitive reframing, and broad acceptance of unchangeable external circumstances 2527. Because the suppression of high-arousal negative emotion is socially sanctioned, normative, and praised in these cultures, collectivists display significantly less physiological stress (demonstrating dramatically lower HPA axis reactivity) in response to the exact same social disruptions that trigger individualists 2528.
These distinct, culturally ingrained coping mechanisms leave direct, measurable fingerprints on global sleep data. A massive comparative longitudinal study analyzing two-wave data between the United States and Japan found a fascinating paradox. Japanese adults sleep, on average, for a significantly shorter duration than their U.S. counterparts (averaging 6.27 hours compared to 6.91 hours in the US cohort) 19. However, despite this notably shorter duration, Japanese adults consistently reported significantly better global sleep quality as measured by the Pittsburgh Sleep Quality Index (PSQI). They experienced much shorter sleep onset latency, higher habitual sleep efficiency, fewer nocturnal sleep disturbances, and lower reliance on sleeping medications 19. This robust data strongly suggests that the collectivist tendency toward internal emotional regulation and systemic acceptance may act as a powerful neurobiological buffer against the HPA-axis hyperarousal that typically prolongs sleep latency in highly individualistic populations.
Spatial and Geographic Disparities in Sleep Health
Research published in 2024 has also decisively highlighted that stress-induced sleep disruption is not just an individual biological issue, but a profound geographic and systemic one. A comprehensive population-based geospatial analysis of the United States revealed that over 45.8 million residents experience extremely low spatial access to professional sleep health care 20.
These stark disparities are most acute in rural geographic areas and among non-white racial minority populations. For instance, Black and Hispanic populations residing in rural settings face significantly higher geographic and socioeconomic barriers to accessing specialized sleep medicine. This lack of access strongly correlates with high rates of untreated chronic insomnia and chronically elevated stress biomarkers 2021.
Furthermore, recent research indicates that the precise biological translation of poor sleep into systemic inflammation actually varies significantly by race and ethnicity, underscoring the need for highly personalized medicine. A detailed 2022 study analyzing hospital nurses found that among White nurses, low sleep time was strictly associated with high levels of IL-6. However, among Black nurses, subjective lower sleep efficiency was strongly associated with dangerous elevations in both IL-6 and IL-1β. Conversely, among Hispanic nurses, greater sleep time was unexpectedly associated with higher CRP levels 14. These complex, highly nuanced findings mandate that future clinical interventions for stress-induced sleep latency must meticulously account for unique cultural stressors (such as everyday discrimination), systemic geographic inequities, and distinct demographic inflammatory biomarkers 142021.
Sleep Duration and Biological Longevity
Adding urgency to the treatment of sleep latency, massive studies from 2024 and 2025 utilizing global biobank data from over 500,000 individuals have conclusively linked sleep duration to biological aging and longevity. Researchers utilizing 23 distinct biological aging clocks found that both excessively short and excessively long sleep durations result in signals of an "older biology" 33.
The data revealed a distinct U-shaped mortality curve. Shorter sleep led to a 50% higher relative risk for all-cause mortality, while exceptionally longer sleep carried a 40% higher risk 33. The optimal "sweet spot" associated with the lowest biological age gap and maximum longevity was identified as 6.5 to 7.8 hours for women, and 6.4 to 7.7 hours for men 33. The lack of adequate sleep was identified as the top behavioral driver of mortality, surpassing even lack of exercise or poor diet, ranking second only to chronic smoking 34.
What This Means for You: Actionable Habits for Downregulating Physical Arousal
Understanding the intricate neurobiology of stress is ultimately only useful if it can be successfully translated into clinical practice. To effectively overcome stress-induced sleep latency, therapeutic interventions must explicitly target what clinical researchers refer to as the "Dual Calm Gap."
The Dual Calm Gap is a physiological framework postulating that the human body possesses two distinct, parallel relaxation systems: the hormonal stress response (the HPA axis regulating cortisol) and the neuromuscular calming system (GABA receptor activity and mineral-dependent processes regulating physical muscle tension) 35. Treating only one of these systems often leaves the individual highly frustrated; lowering cortisol output won't induce sleep if the skeletal muscles remain locked in tension, and relaxing the muscles won't induce sleep if the brain is continuously flooded with CRH and ACTH.
Addressing stress-induced sleep latency permanently requires a rigorous, multi-pronged approach that targets both behavioral conditioning and, where clinically appropriate, physiological supplementation.
Behavioral and Environmental Interventions
1. Cognitive Behavioral Therapy for Insomnia (CBT-I) CBT-I remains the absolute, undisputed gold standard for treating chronic sleep latency and insomnia disorder. Recent 2024 clinical data highlights a specific, fascinating benefit of CBT-I: it actively resolves "sleep misperception." As noted previously, individuals with high stress often suffer from a severe subjective-objective sleep discrepancy. A rigorous 2024 study demonstrated that engaging in CBT-I directly and significantly reduces the discrepancy between subjective and objective measures of sleep onset latency, wake after sleep onset (WASO), and sleep efficiency 8. By fundamentally recalibrating the brain's cognitive perception of rest early in the treatment process, CBT-I breaks the anxiety loop that fuels the HPA axis 822.
2. Light Therapy and Circadian Anchoring A comprehensive 2024 systematic review and meta-analysis investigating sleep interventions for shift-working nurses - a demographic forced to exist under extreme, chronic HPA-axis stress due to irregular schedules - found that light therapy was the most statistically effective non-pharmacological intervention available 37. Viewing bright, natural light immediately upon waking aggressively halts the endogenous production of melatonin and firmly anchors the circadian rhythm. This circadian anchoring in turn optimizes the precise timing of the cortisol nadir (the absolute lowest point of daily cortisol secretion) for the late evening, dramatically facilitating faster sleep onset when the individual finally lies down 1637.
3. Implementing "Somatic Off-Ramps" Because the highly evolved human brain cannot easily utilize cognitive logic to think its way out of a primal stress response, physical (somatic) interventions are absolutely required to signal immediate safety to the hyperactive amygdala. Techniques that mechanically stimulate the vagus nerve - such as prolonged exhalations (where the out-breath is deliberately twice as long as the in-breath) or structured non-sleep deep rest (NSDR) protocols - mechanically slow the cardiovascular heart rate. This physical action forces the parasympathetic nervous system online, effectively applying the biological brakes to the runaway HPA axis and allowing the sleep drive to take over 1638.
The Mixed Clinical Evidence on Dietary Supplements
When behavioral modifications are insufficient to close the Dual Calm Gap, many exhausted individuals turn to over-the-counter dietary supplements. However, the clinical evidence for these compounds is highly mixed, plagued by methodological inconsistencies, and consumers must navigate this unregulated space with extreme caution.
Ashwagandha (Withania somnifera) * Mechanism: Ashwagandha is a botanical adaptogen that specifically targets the hormonal side of the Dual Calm Gap. It acts directly on the HPA axis to actively reduce adrenal cortisol output and modulate the stress response 3539. * Clinical Evidence: Graded Strong. Numerous recent meta-analyses and randomized controlled trials (RCTs) involving hundreds of human subjects show that 300 - 600 mg of standardized ashwagandha root extract (such as KSM-66 or Shoden) taken daily significantly reduces serum cortisol. It objectively improves sleep onset latency, increases total sleep efficiency, and drastically lowers subjective stress scores in chronically stressed individuals 35392341.
Magnesium * Mechanism: Magnesium targets the neuromuscular side of the Dual Calm Gap. It acts as a natural NMDA receptor antagonist and a potent GABA agonist, dampening excitatory neural signaling throughout the cortex and promoting deep physical muscle relaxation 3539. * Clinical Evidence: Graded Mixed/Moderate. While widely promoted across social media, the rigorous clinical evidence for magnesium as a standalone sleep aid is surprisingly heterogeneous. Some studies report notable improvements in sleep parameters, but others (especially those utilizing lower doses like 250mg of cheap Magnesium Oxide) demonstrate absolutely no significant effect compared to a placebo 24. Clinical consensus suggests Magnesium is highly effective primarily for individuals with an underlying dietary deficiency or those whose stress manifests primarily as severe physical muscle tension, rather than purely cognitive anxiety 3924.
Valerian Root (Valeriana officinalis) and L-Theanine * Mechanism: Valerian root contains specific volatile oils and valepotriates that actively inhibit the enzymatic breakdown of GABA in the brain, thereby prolonging its natural sedative effects 4325. L-Theanine, an amino acid found in tea, promotes the generation of alpha brain waves associated with a state of relaxed wakefulness. * Clinical Evidence: Graded Moderate. A comprehensive meta-analysis of 18 RCTs indicated that valerian extract modestly but significantly reduces sleep latency and improves subjective sleep quality metrics (such as the PSQI). However, many studies suffer from severe methodological inconsistencies regarding extraction methods and dosing. It is generally recognized as safe and well-tolerated, and is most appropriate for mild, transient insomnia 15254546.
Melatonin: A Critical 2025 Cardiovascular Safety Warning * Mechanism: Melatonin is not a traditional sedative; it is an endogenous hormone secreted by the pineal gland that regulates the biological circadian rhythm. It signals the optimal timing of sleep to the body, but does not aggressively depress the central nervous system to induce unconsciousness 2648. * Clinical Evidence: Highly Mixed for Insomnia and Potentially Dangerous Long-Term. While melatonin is highly effective for treating acute circadian misalignment (e.g., jet lag, delayed sleep-wake phase disorder), its actual clinical efficacy for treating stress-induced primary insomnia is exceptionally poor. Studies show it often reduces sleep latency by a clinically insignificant margin of merely 5 to 7 minutes 26. * Crucial Update: Melatonin supplements are widely perceived by the general public as universally harmless and "natural." However, a landmark, multinational cohort study presented at the prestigious American Heart Association (AHA) Scientific Sessions in November 2025 issued a severe, paradigm-shifting warning. The massive study, utilizing the TriNetX Global Research Network, analyzed over 130,828 adults diagnosed with insomnia, utilizing rigorous propensity score matching across 40 clinical variables to eliminate confounding factors 2728. The findings were staggering: long-term melatonin use (strictly defined as continuous use for 12 months or more) was associated with an 82% to 90% higher risk of developing incident heart failure, a 3.5-fold increase in heart failure hospitalizations (19.0% vs. 6.6%), and a doubling of all-cause mortality (7.8% vs. 4.3%) over a five-year follow-up period compared to non-users 2648272829. While the study is observational and cannot definitively prove direct causation, this massive data signal strongly suggests that chronic, unregulated reliance on synthetic hormones to bypass stress-induced insomnia may carry profound, previously unrecognized cardiovascular risks. Expert consensus strongly dictates that melatonin should not be utilized as a chronic, nightly crutch for stress-induced wakefulness.
Bottom Line
Stress makes it profoundly harder to fall asleep because it triggers a deeply ingrained, evolutionary survival mechanism that physically alters the body's biochemistry. By activating the HPA axis, psychological stress floods the brain and systemic circulation with cortisol, adrenaline, and inflammatory cytokines, artificially elevating the heart rate and aggressively suppressing the homeostatic sleep drive. This intense systemic hyperarousal cannot be overridden by sheer psychological willpower, nor can it be healthily bypassed with central nervous system depressants like alcohol or risky long-term use of synthetic melatonin. Successfully reducing sleep latency and restoring rest requires a deliberate, biological downregulation of both hormonal arousal and neuromuscular tension. This is achieved through closing the Dual Calm Gap using evidence-based behavioral routines, circadian anchoring, cognitive behavioral therapy, and targeted, clinically validated interventions.