How Sleep Works and How to Improve It
Sleep is an active, highly regulated biological necessity driven by the steady accumulation of neurochemical sleep pressure and the rhythmic ticking of an internal circadian clock. While modern culture often promotes quick fixes like chemical sedatives or weekend sleep-ins to cure chronic exhaustion, scientific consensus points to a different reality: optimizing daily light exposure, aligning with natural chronotypes, and utilizing behavioral frameworks like Cognitive Behavioral Therapy for Insomnia are the only proven methods to achieve restorative, long-term sleep health.
The Paradigm Shift in Sleep Science
For centuries, sleep was viewed by the medical community and the general public as a passive state - a simple, quiet powering down of the biological machine required to rest the physical body. This perception fundamentally changed in the 1950s when researchers Nathaniel Kleitman and Eugene Aserinsky utilized early electroencephalographic (EEG) recordings to demonstrate that the sleeping brain is remarkably active 1. Their discovery of distinct, cyclical sleep stages proved that sleep is a dynamic physiological state characterized by intense neurological, metabolic, and hormonal activity 12.
Today, neurobiological research has mapped the precise mechanisms that drive human sleep, revealing a dual-system framework known as the two-process model 3. This model dictates that human sleep is governed by two interacting, yet independent, biological mechanisms: Process S, which represents homeostatic sleep pressure, and Process C, which represents the circadian rhythm 34. The interaction between these two systems dictates when individuals feel alert, when they experience profound fatigue, and how effectively their brains can transition into a state of rest.
The Mechanics of Slumber: The Two-Process Model
Understanding the two-process model is essential for diagnosing sleep dysfunction and optimizing rest. The delicate balance between homeostatic drive and circadian timing governs the entire architecture of the human sleep-wake cycle.
Process S: The Adenosine Hourglass
Process S represents the homeostatic sleep drive, which operates like an internal biochemical hourglass. The primary currency by which the brain measures the time an individual has spent awake is a molecule called adenosine 4. Adenosine is a fundamental byproduct of cellular metabolism. Specifically, it is the breakdown product of adenosine triphosphate (ATP), which serves as the primary energy substrate for all nucleated cells in the body, including neurons and glial cells 56.
From the moment an individual wakes up, ATP is steadily depleted by normal neuronal activity, cognitive function, and physical exertion. As ATP is consumed, adenosine progressively accumulates in the extracellular space of the brain, particularly within wake-active regions such as the basal forebrain and the cortex 67. This accumulation acts as a biochemical "tiredness meter." As adenosine levels rise throughout the day, the molecule binds to specific high-affinity neuro-receptors, primarily the A1 and A2A receptors 67.
The binding of adenosine to these receptors initiates a cascading neurological effect. It actively inhibits arousal-promoting neurons that rely on excitatory neurotransmitters like acetylcholine and hypocretin 57. Simultaneously, adenosine enhances the activity of sleep-promoting GABAergic neurons in the ventrolateral preoptic nucleus of the brain 77. This dual action - suppressing the wakeful centers while stimulating the sleep centers - creates a profound, irresistible physiological pressure to sleep 7.
When an individual finally succumbs to sleep, the brain begins to clear this accumulated adenosine, recycling it back into new stores of glycogen and ATP 49. This clearance resets the homeostatic hourglass for the following day. This precise mechanism perfectly explains the biological function of caffeine. Caffeine operates as a competitive antagonist that fits seamlessly into A1 and A2A adenosine receptors, effectively blocking the sleep signal from reaching the brain 710. However, caffeine does not halt the production or accumulation of adenosine. Once the caffeine is metabolized and vacates the receptors, the brain is flooded by the artificially dammed reservoir of adenosine, resulting in a severe, sudden crash in energy 1011.
Process C: The Circadian Clock
While Process S builds a linear, mounting pressure to sleep based on time spent awake, Process C operates as a continuous, oscillating 24-hour clock that regulates alertness independently of prior sleep 4. Driven primarily by a dense cluster of neurons in the hypothalamus known as the suprachiasmatic nucleus (SCN), the circadian rhythm responds strongly to environmental light and dark cycles 118.
The SCN acts as the body's master conductor, regulating the nocturnal release of melatonin from the pineal gland, which signals to the body's systemic physiology that it is time to wind down 4. The circadian process also coordinates a natural drop in core body temperature, which is biologically required to facilitate the onset and maintenance of deep sleep 4.
Sleep naturally occurs with the least resistance when the gap between these two processes is at its absolute widest - when homeostatic sleep pressure (adenosine) is at its peak, and the circadian alerting signal drops to its lowest nocturnal point 11. The interaction between sleep pressure and the circadian rhythm is a foundational concept in chronobiology that perfectly explains the phenomenon of the "second wind." If an individual pulls an all-nighter, they will experience crushing fatigue at 3:00 AM. However, by 8:00 AM, they may oddly feel a surge of wakefulness. This occurs because, even though adenosine levels remain critically high, the circadian alerting signal (Process C) begins its morning upswing, closing the gap between the two processes and temporarily overriding the homeostatic pressure to sleep 11.
The Architecture of the Night: Sleep Stages and Cycles
Once an individual transitions from wakefulness to sleep, the brain does not simply enter a uniform state of dormancy. Instead, it embarks on a highly structured, complex 90-to-110-minute cycle that repeats four to six times over the course of a typical night 29. This architecture is broadly divided into Rapid Eye Movement (REM) sleep and Non-Rapid Eye Movement (NREM) sleep. NREM sleep is further categorized into three distinct stages of increasing depth 1011.
The duration and density of these stages change dynamically throughout the night. The first half of the sleep period is heavily dominated by deep, restorative NREM sleep, while the second half is disproportionately weighted toward REM sleep 810.
A Clinical Breakdown of the Sleep Cycle
The stages of sleep are defined by specific electroencephalographic (EEG) patterns, muscle tone variations, and eye movements 110.
| Sleep Stage | Classification | % of Total Sleep | Typical Duration per Cycle | Clinical Characteristics and Biological Functions |
|---|---|---|---|---|
| Stage 1 (N1) | Light NREM | ~5% | 1 - 7 minutes | The transition phase between wakefulness and sleep. Characterized by theta waves (4 - 8 Hz). Brain activity slows, heartbeat regulates, but the individual can be easily awakened. Often perceived subjectively as being "awake" 18912. |
| Stage 2 (N2) | Core NREM | 45 - 50% | 10 - 25+ minutes | The baseline state of stable sleep. Body temperature drops, and muscles relax. Characterized by "sleep spindles" (10-15 Hz bursts) and "K-complexes" (long delta waves) that protect the brain from waking up due to external environmental noise 181217. |
| Stage 3 (N3) | Deep NREM | 20 - 25% | 20 - 40 minutes (early night) | Known as slow-wave sleep (SWS), defined by slow delta brain waves (0.5-2 Hz). Blood pressure drops significantly. It is incredibly difficult to wake someone from N3. Critical for physical tissue repair, growth hormone release, and immune system strengthening 1891713. |
| REM Sleep | REM | 20 - 25% | 10 - 60 minutes (late night) | Brain activity mirrors the awake state (beta activity). Muscles become temporarily atonic (paralyzed) to prevent acting out dreams. Essential for emotional regulation, memory consolidation, and cognitive problem-solving 181217. |
Lifespan Alterations in Sleep Architecture
Sleep architecture is not static; it evolves dramatically across the human lifespan, reflecting the changing biological necessities of the brain 810. Newborn infants experience highly irregular sleep patterns, spending a vast majority of their total sleep time in active REM sleep, which is believed to be vital for rapid neural development and synapse formation 810.
As children mature, circadian rhythms solidify. The total amount of deep slow-wave sleep (N3) peaks in early childhood, supporting periods of massive physical growth, before dropping sharply during the teenage years 810. This decline continues relentlessly throughout adulthood. By late adulthood, the amplitude of delta waves diminishes significantly, and many older individuals may experience a near-total loss of the deepest stages of N3 sleep, resulting in lighter, highly fragmented sleep that is easily disrupted by environmental stimuli or physiological discomfort 810.
The Glymphatic System: The Brain's Nightly Detoxification
One of the most profound discoveries in modern neuroscience revolves around why Stage 3 deep sleep is so fiercely protected by biological evolution, despite leaving the organism highly vulnerable to predation. In 2012, researchers at the University of Rochester identified the glymphatic system, a macroscopic waste-clearance pathway in the central nervous system that functions essentially as the brain's internal plumbing 1920.
Throughout the waking day, normal neuronal metabolism produces massive amounts of biochemical waste. Among these byproducts are neurotoxic proteins, specifically amyloid-beta and tau, the accumulation of which is the primary pathological hallmark of neurodegenerative diseases such as Alzheimer's 201415. During wakefulness, the cellular structure of the brain is highly compacted to facilitate rapid neural transmission, and the glymphatic system operates at a mere fraction of its total capacity 2023.
However, when the brain enters deep, dreamless NREM sleep, a remarkable mechanical shift occurs. The interstitial space between brain cells physically expands by roughly 60%, drastically reducing the resistance to fluid flow 2023. This expansion is facilitated by specialized water channels called aquaporin-4 (AQP4), which are densely located on the endfeet of astrocyte cells surrounding the brain's blood vessels 201415.
Driven by the rhythmic pulsation of the brain's arteries with each heartbeat, cerebrospinal fluid (CSF) surges into the expanded brain tissue 201415. This fluid acts akin to a high-pressure mechanical wash, mixing with interstitial fluid to flush out the day's accumulation of neurotoxins, lactic acid, and metabolic garbage 1523. The waste-laden fluid is then shuttled out through perivenous spaces into the body's standard peripheral lymphatic system for ultimate disposal 2023.
The Danger of Chemical Unconsciousness
This mechanical cleaning cycle reveals a vital clinical insight regarding the nature of rest: chemical unconsciousness induced by pharmacology is not biologically equivalent to natural sleep architecture.
Recent studies indicate that certain widely prescribed sedative-hypnotic medications, such as zolpidem (Ambien) and various benzodiazepines, can successfully render a patient unconscious but often fail to produce the natural sleep architecture required for physiological maintenance 23. The glymphatic flushing mechanism relies heavily on rhythmic waves of the neurotransmitter norepinephrine, which occur naturally every 50 seconds during deep NREM sleep 23. These waves trigger the vasomotion (vessel pumping) that drives the fluid through the brain.
Data shows that some common sleep aids actively suppress these vital norepinephrine oscillations by approximately 50%, effectively reducing the brain's cleaning efficiency by roughly 30% 23. This suggests that while pharmaceutical sleep aids may provide the subjective illusion of a full night's rest, they may inadvertently trap metabolic waste in the brain by blunting the depth of the slow-wave sleep required to run the glymphatic "dishwasher" at full capacity 23.
The Hidden Biological Costs of Sleep Debt
When individuals fail to secure the necessary 7 to 9 hours of sleep recommended for optimal adult health, they begin to accumulate a physiological deficit known as "sleep debt" 1617. Because sleep debt is strictly cumulative, losing just 30 to 60 minutes of sleep a night over the course of a workweek results in a profound, systemic biological deficit 16.
The immediate health impacts of even minor sleep loss are severe and measurable. A recent clinical study conducted at Columbia University demonstrated that losing just one hour of sleep per night for six weeks increased endothelial oxidative stress - cellular damage lining the circulatory system - by 78% 26. This acute inflammatory response helps explain why epidemiological data consistently shows a 24% spike in acute myocardial infarctions (heart attacks) on the Monday immediately following the transition to Daylight Saving Time, when the population collectively loses a single hour of rest 26.
Chronic sleep deprivation compounds these acute issues into systemic, long-term health crises. Prolonged restriction to less than five or six hours a night is statistically linked to an array of pathologies: * A 50% higher risk of clinical obesity, driven by the severe dysregulation of metabolic hormones. Sleep loss artificially lowers leptin (the hormone responsible for signaling satiety) and drastically elevates ghrelin (the hormone that triggers intense hunger and cravings for carbohydrate-dense foods) 1819. * A nearly 3-fold increased risk of Type 2 diabetes, as chronic sleep loss severely impairs the body's ability to utilize insulin efficiently, resulting in elevated blood glucose levels and profound metabolic syndrome 171819. * A 33% increase in dementia risk, stemming directly from the chronic failure of the glymphatic system to clear amyloid-beta and tau proteins over decades of restricted sleep 1920. * Profound Immunosuppression, characterized by a marked decrease in the activity of natural killer cells, leaving sleep-deprived individuals nearly three times more likely to contract common viral infections 1819.
The Weekend Recovery Myth
For decades, millions of individuals in industrialized nations have operated on the assumption that they can endure sleep restriction from Monday to Friday and simply "catch up" on their accrued sleep debt by sleeping extended hours on the weekend 30. Modern clinical research definitively proves this behavioral strategy is biologically inadequate 1630.
While sleeping in on Saturday and Sunday can restore subjective feelings of alertness and temporarily alleviate the sensation of fatigue, it does not repair the underlying metabolic and cognitive damage incurred during the week 30. A pivotal 2024 study published in Current Biology investigated this specific dynamic. Participants were subjected to five days of restricted sleep (5 hours per night), followed by two days of completely unrestricted "recovery" sleep 1630. The study demonstrated that the weekend recovery sleep completely failed to reverse the metabolic dysregulation, persistent insulin sensitivity deficits, and caloric overconsumption caused by the initial restriction 30. The metabolic markers of the recovery group were statistically no better than the control group that received zero recovery sleep at all 30.
Furthermore, aggressively shifting sleep timing on the weekends creates a phenomenon known as "social jetlag." A massive 2024 study from Jagiellonian University analyzing 477 adults found that extreme differences between weekday and weekend sleep timing were directly associated with increased systemic inflammatory markers and higher Body Mass Index (BMI), regardless of the total weekly sleep hours obtained 3031.
The scientific consensus is absolute: while a single night of poor sleep can be mostly recovered with one subsequent night of adequate rest, chronic, multi-day sleep debt causes cumulative damage to metabolic, cognitive, and cardiovascular health that weekend recovery cannot reverse 163031. Complete recovery from profound chronic sleep deprivation requires weeks of consistent, restorative sleep scheduling 31.
Global Sleep: Chronotypes and Cultural Habits
While the biological necessity of sleep is a human universal, the specific execution of sleep timing is heavily influenced by individual genetics and macro-level cultural norms.
The Chronotype Spectrum and Social Jetlag
A chronotype represents an individual's natural, genetically influenced predisposition to feel alert or sleepy at specific times of the 24-hour cycle 2122. Historically, researchers and the public categorized chronotypes as a simplistic binary between "early birds" (morningness) and "night owls" (eveningness) 23.
However, a massive 2026 study from McGill University utilizing artificial intelligence to analyze brain imaging, medical records, and behavioral questionnaires from 27,000 adults in the U.K. Biobank revealed a much more complex reality 23. The analysis identified five distinct biological subtypes of chronotypes, each with highly unique cognitive and health profiles 23. For example, the data revealed multiple distinct variations of the "night owl" chronotype: one group demonstrated superior cognitive performance but struggled with emotional regulation, while another exhibited a high propensity for risk-taking behaviors, and a third was disproportionately linked to depression, smoking, and cardiovascular disease 23.
Crucially, psychiatric and neurobiological research indicates that forcing late-chronotype individuals to adhere to rigid, early-morning societal schedules (such as traditional corporate hours or early school start times) creates a profound, chronic mismatch between their preferred biological sleep timing and their actual behavioral timing 24. This chronic misalignment is consistently linked to poorer mental health outcomes, higher rates of anxiety, and a generally elevated neurocognitive vulnerability across the lifespan 24.
Cultural Variations: Beyond the Western Monophasic Norm
Western society overwhelmingly promotes monophasic sleep - the expectation that humans should sleep in one continuous, uninterrupted 7-to-8-hour block throughout the night 36. However, global anthropological data suggests that strict monophasic sleep is largely a modern artifact of the Industrial Revolution and the advent of artificial lighting 373839.
- Pre-industrial and Hunter-Gatherer Sleep: Studies analyzing contemporary traditional hunter-gatherer societies, such as the Hadza of Tanzania and the Tsimane of Bolivia, reveal highly flexible sleep patterns 37. Without the influence of artificial light, these populations naturally align with seasonal light-dark cycles, often practicing biphasic or polyphasic sleep 37. This involves frequent daytime napping combined with shorter, more fragmented nighttime sleep, a pattern hypothesized to maintain communal vigilance against environmental threats and predators 3740.
- The Siesta Tradition: Mediterranean and Latin American cultures have historically embraced the siesta - a formal biphasic pattern dividing daily sleep into a 5-to-6-hour overnight segment and a sustained 2-to-3-hour afternoon rest 363738. Originally an adaptation to avoid intense midday heat and align agricultural labor with cooler evening hours, the biphasic siesta model has been shown to be perfectly compatible with excellent long-term physical health and cognitive function 3637.
- Inemuri in Japan: In stark contrast to Western corporate culture, where sleeping in the workplace is viewed as highly unprofessional, Japan practices the cultural tradition of Inemuri, which translates literally to "being present while sleeping" 4041. It is a socially accepted, and often respected, practice of taking brief micro-naps on public transit, in offices, or even during corporate meetings 4243. Far from being interpreted as a sign of laziness, Inemuri is viewed as a testament to an employee's extreme diligence - proof that they have dedicated themselves to their work to the point of utter physiological exhaustion 394243. Research indicates that keeping these micro-naps brief (ideally between 10 and 20 minutes) provides a substantial boost to alertness and performance without triggering the deep-sleep grogginess known as sleep inertia 4142.
Evaluating Sleep Optimization Trends and Technologies
As the public health impact of sleep deprivation becomes more widely understood, a massive consumer market has emerged offering technologies and techniques aimed at optimizing rest. However, clinical evidence separating effective interventions from marketing hype is vital.
The Accuracy of Consumer Sleep Trackers
To combat poor sleep, an estimated one-in-three Americans now wear a consumer sleep-tracking device, such as an Oura Ring, Apple Watch, or Fitbit 44. Consumers increasingly rely on these devices to dictate their daily behavior and judge the quality of their rest. But how clinically accurate are the proprietary algorithms driving these devices?
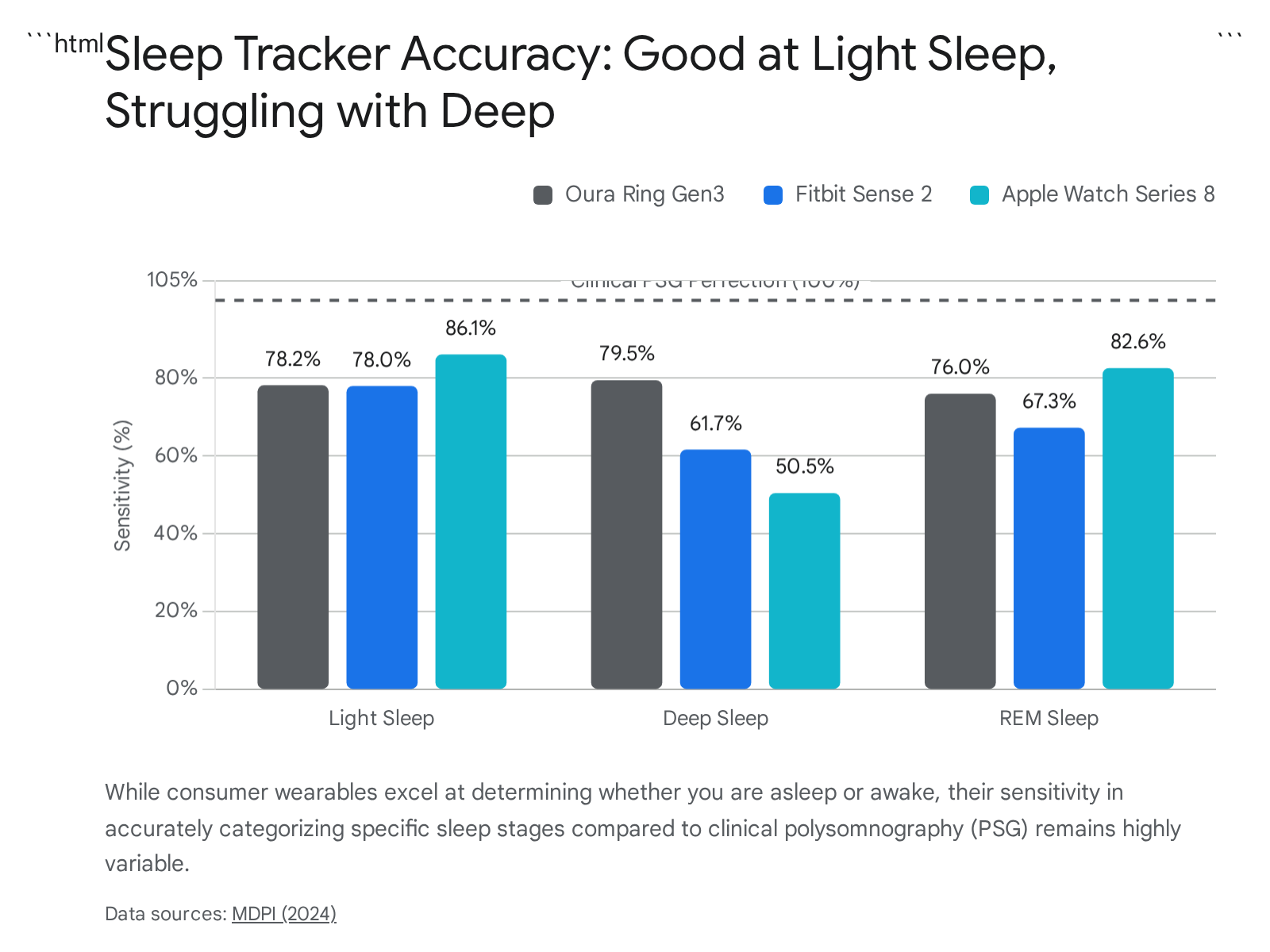
Recent peer-reviewed analyses from 2024 suggest these devices are highly effective at their primary, most basic task: differentiating between sleep and wakefulness. Compared to clinical polysomnography (PSG) - the absolute gold standard of lab-based sleep tracking that utilizes EEG brainwave monitoring - modern consumer wearables boast an impressive sensitivity of 95% or higher for detecting gross sleep versus wakefulness 4525. In fact, due to advancements in multi-sensor integration (combining accelerometry with optical heart rate variability), consumer devices are now considered on par with, or even superior to, the expensive clinical actigraphy watches traditionally issued by medical professionals for at-home sleep studies 444748.
However, the major limitation of these devices lies in their ability to accurately identify specific sleep stages (Light, Deep, and REM sleep). Because wearables rely entirely on peripheral markers like movement and pulse, rather than direct brainwave activity, their accuracy drops significantly when attempting to map the exact architecture of the night. When compared epoch-by-epoch to PSG data, the sensitivity for stage detection ranges widely from 50% to 86%, depending heavily on the specific brand of the device and the specific sleep stage being estimated 4547.
The Disappointment of Blue-Light Glasses
Another ubiquitous trend in the quest for optimized rest is the utilization of blue-light blocking glasses (BBGs) before bed to protect the circadian rhythm from the glow of digital screens. However, extensive clinical research indicates that this intervention is largely ineffective.
A major 2023 Cochrane systematic review - widely considered the gold standard of evidence-based medicine - evaluated 17 randomized controlled trials across six countries to determine the efficacy of blue-light filtering lenses 4926. The review concluded that the evidence supporting these lenses is practically non-existent. Wearing blue-light filtering glasses made absolutely no statistically significant difference in sleep quality, the time it took patients to fall asleep (sleep onset latency), or the alleviation of subjective eye strain compared to clear, non-filtering placebo lenses 492651.
One of the primary biological reasons for this clinical failure relates to sheer volume. While the concept of minimizing artificial light at night is scientifically sound for melatonin production, the specific amount of blue light emitted by a standard smartphone or computer monitor is roughly one-thousandth of the blue light the human eye receives from natural ambient daylight 492627. Therefore, while minimizing late-night screen time is generally beneficial for reducing psychological stimulation, the specific physical intervention of wearing non-prescription blue-light filter lenses appears to be driven almost entirely by aggressive commercial marketing rather than demonstrated clinical efficacy 4926.
Common Sleep Myths Debunked
Alongside commercial trends, public health is routinely undermined by pervasive, deeply ingrained myths regarding how sleep works. * "Alcohol helps induce sleep." Many individuals rely on a "nightcap" to wind down. While alcohol acts as a central nervous system depressant that can cause an individual to lose consciousness faster, it fundamentally destroys sleep architecture. Alcohol severely fragments sleep in the second half of the night and aggressively suppresses REM sleep, leaving the brain unrefreshed and preventing vital emotional and cognitive processing from occurring 185354. * "Snoring is a harmless annoyance." While occasional, light snoring can be benign (often related to sleep position or mild allergies), loud, chronic snoring is frequently the primary outward symptom of Obstructive Sleep Apnea (OSA) 185354. OSA is a severe condition where the airway collapses, causing breathing to repeatedly stop throughout the night. This yanks the brain out of deep, restorative sleep in order to gasp for air, leading to profound cardiovascular strain, hypertension, and long-term cognitive decline 185354. * "I can train my body to survive on 5 hours of sleep." Humans possess no biological capacity to "adapt" to chronic sleep deprivation. While an individual may quickly lose the subjective feeling of extreme sleepiness - because their brain's baseline perception of normal simply resets to a lower, impaired level - objective clinical tests reveal a different reality. When tested, the reaction times, working memory, and emotional regulation of these individuals continue to deteriorate relentlessly, leaving them operating at a profound, often dangerous, cognitive deficit 165354.
Evidence-Based Protocols to Improve Sleep Quality
If weekend catch-ups, evening alcohol, and blue-light glasses do not work, what interventions does the clinical evidence actually support for improving the quality and duration of sleep?
1. Harnessing Environmental Light Exposure
Because the circadian rhythm (Process C) relies on light as its primary external zeitgeber (time-giver), manipulating your physical light environment is one of the most powerful, evidence-based behavioral interventions available. A major scientific consensus report, summarizing extensive laboratory data on human circadian responses, established concrete targets based on "melanopic equivalent daylight illuminance" (EDI) 5657:
- Daytime: Maximize bright light exposure (Melanopic EDI > 250 lux) throughout the intervening daytime hours. Bright light exposure early in the day robustly anchors the circadian clock, increases daytime alertness, and surprisingly correlates with lower subjective sleepiness later in the evening 5628.
- Evening (3 hours before bed): Drastically reduce ambient light exposure (Melanopic EDI < 10 lux). High pre-bedtime light exposure aggressively delays the onset of natural melatonin production and significantly prolongs sleep onset latency (the time it takes to transition from wakefulness to stage 1 sleep) 5628.
- Nighttime/Sleep: The sleeping environment should be as pitch black as practically possible (Melanopic EDI < 1 lux). Any ambient light in the bedroom can trigger inappropriate nonvisual neurological responses that fragment sleep architecture, even through closed eyelids 565728.
2. Natural Sleep Supplements: Evaluating the Evidence
The global supplement market is saturated with products promising deep, restorative rest. However, a review of systemic literature reveals a highly nuanced picture of what actually influences sleep architecture.
| Supplement / Aid | Clinical Evidence Level | Mechanism & Efficacy |
|---|---|---|
| Melatonin | Strong | Highly effective for shifting circadian rhythms, making it ideal for treating jet lag, shift work disorders, or delayed sleep phase syndrome. Best taken in very low doses (0.5 - 3mg) 30-60 minutes prior to bed. It helps initiate the onset of sleep but is generally not a reliable cure for chronic, middle-of-the-night awakenings 596061. |
| Magnesium (Glycinate) | Moderate | Observational data strongly links low magnesium intake to poor sleep quality and daytime sleepiness. Several randomized controlled trials (RCTs) show it can improve sleep efficiency and increase total sleep time, particularly in older adults or those with a baseline deficiency. Magnesium glycinate is the preferred formulation over citrate to maximize absorption and avoid gastrointestinal distress 59296330. |
| L-Theanine | Moderate | An amino acid commonly found in green tea that promotes neurological relaxation without heavy sedation. Clinical trials show it is particularly effective at quieting racing thoughts in individuals suffering from anxiety or stress-related sleep onset issues, though the overall effects on sleep architecture are subtle 5931. |
| Valerian Root | Weak / Mixed | A highly popular botanical herb that frequently improves subjective sleep quality (patients report feeling they slept better). However, rigorous umbrella reviews of high-quality RCTs show almost no objective clinical evidence that it actually helps patients fall asleep significantly faster or stay asleep longer compared to a placebo. Standardized extraction methods vary wildly, leading to inconsistent results 59663233. |
| CBD & Ashwagandha | Insufficient | Most perceived benefits are secondary to general stress and anxiety reduction. Direct clinical trials specifically measuring precise sleep outcomes (latency, duration, architecture) for these supplements currently show minimal, if any, objective improvements over placebo. Marketing claims heavily outpace the peer-reviewed data 59. |
| Prescription Hypnotics (Z-Drugs) | Strong (Short-Term) | Medications like Zolpidem (Ambien) and Eszopiclone are highly effective at forcing rapid sleep onset by enhancing GABA activity in the brain. However, they carry significant risks of pharmacological dependence, next-day cognitive impairment, complex sleep behaviors, and can alter the depth of natural sleep architecture. Clinical guidelines strongly recommend limiting their use to short, acute durations 603470. |
3. The Clinical Gold Standard: Cognitive Behavioral Therapy for Insomnia (CBT-I)
When addressing chronic, persistent sleep disruption, the consensus among medical bodies, including the American Academy of Sleep Medicine, is absolute: the first-line treatment is not a pharmacological pill or an herbal supplement, but Cognitive Behavioral Therapy for Insomnia (CBT-I) 667172.
Unlike medications or supplements that merely mask the downstream symptoms of sleeplessness, CBT-I systematically targets the underlying behavioral, psychological, and neurobiological root causes of chronic insomnia 7172. It is a highly structured, multi-component therapeutic intervention that typically operates over several weeks and relies on specific behavioral protocols: * Sleep Restriction Therapy: This counterintuitive process involves temporarily, deliberately reducing the total amount of time a patient is allowed to spend in bed. By eliminating fragmented tossing and turning, the therapy artificially drives up Process S (homeostatic sleep pressure), forcing the brain to consolidate sleep into a single, dense, unbroken block 3574. * Stimulus Control: This component aims to break the toxic psychological association between the bedroom and feelings of anxiety, frustration, or wakefulness. Patients are instructed to re-associate the bed purely with sleep (and sex), requiring them to physically leave the bed and the room if they cannot fall asleep within 20 minutes, thereby rebuilding a strong neurological cue for rest 7275. * Cognitive Restructuring: A psychological intervention designed to challenge and dismantle the severe performance anxiety and catastrophic thinking that plagues individuals when they look at the clock and realize they cannot fall asleep 7172.
Extensive systematic reviews and meta-analyses consistently demonstrate that CBT-I is clinically superior to both placebos and prescription sleep medications for long-term insomnia relief 723574. While pharmaceutical sleeping pills inevitably lose their efficacy over time due to receptor tolerance and carry significant risks of rebound insomnia upon cessation, the behavioral and cognitive skills acquired through CBT-I induce durable, permanent changes to a patient's sleep architecture. Clinical data shows that the positive effects of CBT-I persist for months, and often years, after the formal treatment has concluded, empowering individuals to manage their sleep pathology independently without reliance on external chemical substances 713574.
Bottom line
Sleep is not a passive luxury, but an active, foundational biological process that strictly dictates cardiovascular health, metabolic stability, and cognitive longevity. The brain relies completely on the deep, slow-wave stages of sleep to literally wash itself of neurotoxins via the glymphatic system - a mechanical process that cannot be fully replicated by chemical sedatives or casually recovered during fragmented weekend sleep-ins. While the consumer market is flooded with quick-fix supplements, questionable diagnostic trackers, and ineffective blue-light glasses, true sleep optimization stems from respecting core biological mechanisms: anchoring the circadian rhythm with bright morning light, aggressively protecting evenings from artificial illumination, and utilizing proven, evidence-based behavioral frameworks like CBT-I to resolve chronic dysfunction.