What Happens During Fight-or-Flight Second by Second
The acute stress response is initiated when the amygdala detects a threat, instantly triggering the fast-acting sympathetic nervous system to release catecholamines like adrenaline for immediate physiological arousal. This rapid neural signaling is followed by the slower, hormonally driven hypothalamic-pituitary-adrenal (HPA) axis, which releases cortisol minutes later to sustain energy levels and mobilize metabolic resources. Together, these cascading neural and endocrine signals rapidly transform the body from a state of resting homeostasis into one optimized for survival.
The Evolutionary Mismatch: Why an Email Triggers Ancient Biology
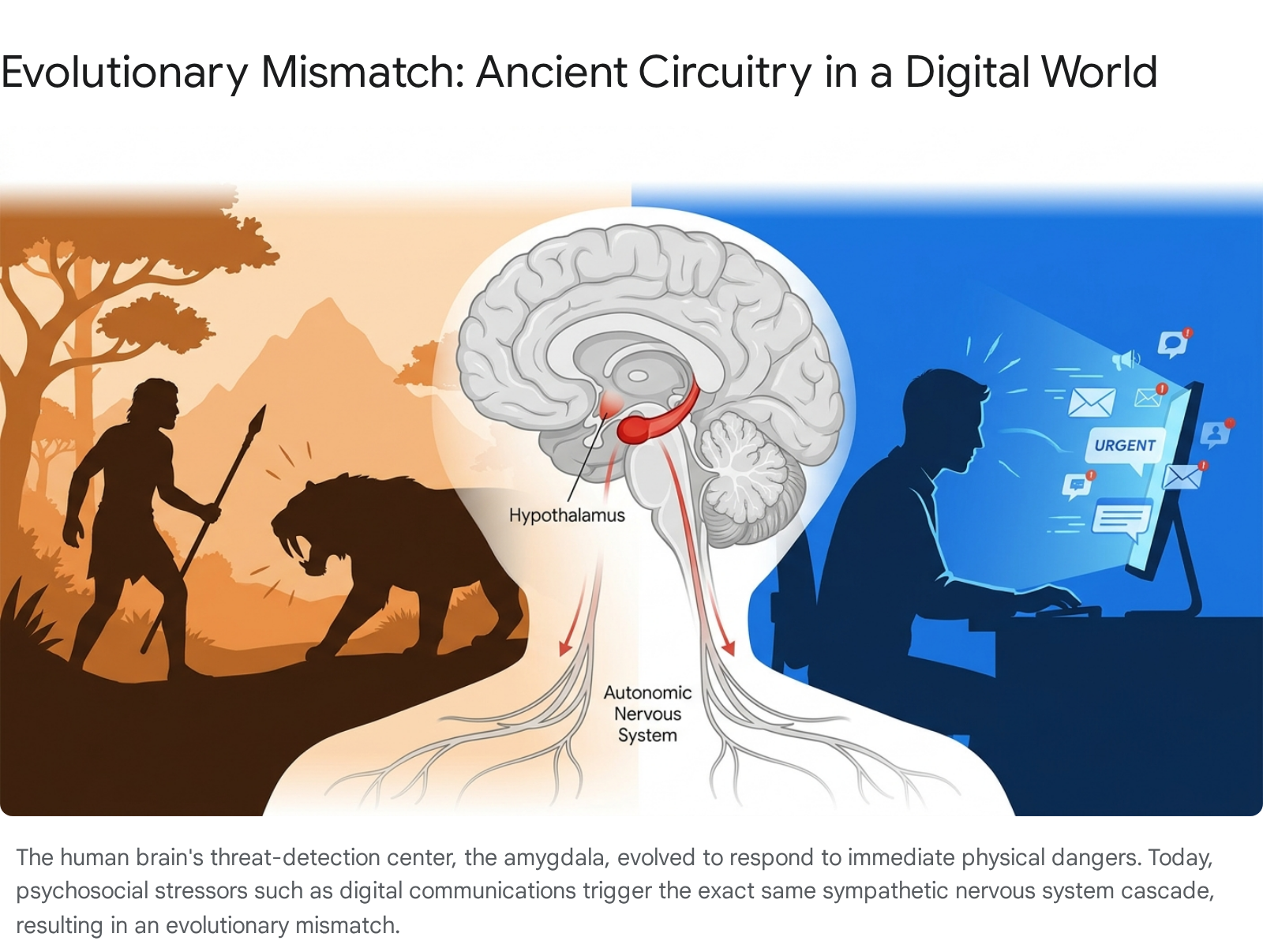
In the modern era, the sudden chime of an incoming email from an unhappy supervisor or the jarring alert of a calendar notification frequently elicits a profound physiological reaction: a racing heart, shallow breathing, and sudden muscular tension. Anthropological and evolutionary medicine research spanning 2024 to 2026 highlights a phenomenon known as "evolutionary mismatch," which explains why the human body responds to non-lethal digital stimuli with the same biological ferocity as it would to a physical predator 112.
For hundreds of thousands of years, the human nervous system evolved to detect and respond to immediate, life-threatening dangers in the physical environment, such as an ambush by a predator or a sudden environmental catastrophe 24. The survival mechanisms forged in these ancestral environments relied on massive, instantaneous mobilizations of metabolic resources to facilitate either a physical confrontation or a rapid escape. Humans evolved to live in kin-based, nomadic tribes of approximately 50 to 150 close-knit individuals, where social and physical threats were immediate but typically episodic 1. Civilization and technological acceleration, however, have occurred in a fraction of evolutionary time, leaving the paleolithic brain largely unchanged 2.
The brain's threat-detection circuitry, centered in the amygdala, remains fundamentally unable to differentiate between an existential physical threat and the psychosocial pressure of modern, high-velocity digital environments 23. The digital revolution happened in a single generation, exposing human neurobiology to a continuous stream of notifications, algorithmic evaluations, and AI-driven technostress that mimic the urgency of ancestral predators 23. When a stressful email arrives, the autonomic nervous system (ANS) interprets the psychological threat as a physiological emergency.
The ANS operates primarily through two opposing branches: the sympathetic nervous system (SNS) and the parasympathetic nervous system (PNS). In a widely utilized real-world analogy, the sympathetic nervous system functions as the body's "gas pedal," rapidly accelerating biological systems to mobilize energy and defend the organism. Conversely, the parasympathetic nervous system acts as the "brakes," promoting rest, digestion, and systemic recovery 648. Modern humans frequently experience chronic, low-grade activation of the sympathetic gas pedal without the subsequent physical exertion - the actual fighting or fleeing - required to metabolize the resulting biochemical surge. This persistent activation leads to an allostatic load, a state of chronic physiological wear and tear that disrupts homeostasis and contributes to the contemporary epidemic of anxiety and stress-related disorders 35.
What Exactly Triggers the Acute Stress Response?
The acute stress response is fundamentally a mechanism of neuroception, the unconscious and continuous scanning of the internal and external environment for cues of safety or danger. This process begins in the limbic system, specifically within the amygdala, an almond-shaped cluster of nuclei located deep within the medial temporal lobes 656. The amygdala functions as the brain's primary alarm system, evaluating emotional salience and threat probability. It receives sensory information - visual, auditory, and olfactory - directly from the thalamus, often before that information has been fully processed and contextualized by the conscious, rational centers of the medial prefrontal cortex (mPFC) 57.
Under normal, non-threatening conditions, the mPFC exerts "top-down" regulatory control over the amygdala, inhibiting its hyper-reactivity and allowing for measured, logical responses 5. However, during acute stress, the massive influx of excitatory neurotransmitters causes the amygdala to overpower this prefrontal inhibition. The basolateral amygdala amplifies fear and anxiety responses, signaling the central nucleus of the amygdala to initiate a systemic alarm 56.
If the amygdala perceives a stimulus as threatening, it instantly sends an electrical distress signal to the paraventricular nucleus (PVN) of the hypothalamus. The hypothalamus acts as the primary command center for both the autonomic nervous system and the endocrine system. It sits at the crucial physiological intersection between rapid neurological signaling and sustained hormonal release, tasked with translating the amygdala's electrical alarm into a widespread, multi-systemic physiological cascade 678. The hypothalamus initiates this defensive cascade through two distinct but highly coordinated pathways: the Sympathetic-Adrenal-Medullary (SAM) axis, which acts almost instantaneously, and the Hypothalamic-Pituitary-Adrenal (HPA) axis, which acts as a delayed, sustained secondary response 8131415.
How Does the Fast-Acting SAM Axis Hijack the Body?
The SAM axis represents the immediate, "fast-acting" component of the stress response, operating at the speed of electrical neural transmission. When the hypothalamus receives the distress signal from the amygdala, it immediately activates sympathetic preganglionic neurons that travel straight down the spinal cord and directly innervate the adrenal medulla, the inner portion of the adrenal glands situated atop the kidneys 14910.
Because the adrenal medulla is essentially composed of modified sympathetic ganglia acting as an extension of the central nervous system, it does not rely on slow hormonal synthesis to mount its initial defense. Instead, the cells of the adrenal medulla store pre-synthesized pools of catecholamines - namely epinephrine (adrenaline) and norepinephrine (noradrenaline) - in specialized vesicles known as chromaffin granules 1011. Upon neural stimulation via the neurotransmitter acetylcholine from sympathetic neurons, the adrenal medulla instantly dumps these massive stores of catecholamines directly into the systemic circulation 910.
The sudden surge of epinephrine and norepinephrine is responsible for the aggressive physiological hijacking associated with the fight-or-flight response. Within a matter of seconds, catecholamines bind to alpha and beta-adrenergic receptors distributed throughout the body, causing systemic alterations designed entirely to maximize physical exertion, energy mobilization, and sensory acuity 1019. The synthesis pathway for these hormones begins with the amino acid tyrosine, which is converted to DOPA, then dopamine, and subsequently norepinephrine. The adrenal medulla, however, expresses a unique enzyme, phenylethanolamine-N-methyltransferase (PNMT), which catalyzes the final conversion of norepinephrine to epinephrine 10.
Once released, these catecholamines drive dramatic cardiovascular and respiratory changes. The heart rate accelerates intensely, sometimes doubling or tripling its resting rhythm within seconds, drastically increasing cardiac output to pump highly oxygenated blood to skeletal muscles 9. The bronchioles in the lungs dilate to reduce airway resistance and allow maximal oxygen intake, resulting in rapid, shallow breathing patterns. Blood vessels undergo selective routing: vasoconstriction occurs in non-essential areas such as the skin and digestive tract, while simultaneous vasodilation occurs in major muscle groups to maximize strength and speed 139. Concurrently, epinephrine binds to receptors in the liver, stimulating rapid glycogenolysis - the breakdown of stored glycogen into free glucose - flooding the bloodstream with readily available cellular fuel. In adipose tissue, epinephrine stimulates hormone-sensitive lipase, promoting lipolysis to release fatty acids as an alternative energy source 1019.
Second-by-Second Timeline of the Acute Stress Response
The biological transformation from a resting state of homeostasis to maximum sympathetic arousal occurs in a highly orchestrated sequence. The interaction between sensory perception, neural firing, and chemical release dictates the exact moment a human being subjectively feels the physiological shifts of stress. The following table delineates the physiological events of the acute stress response from the initial millisecond of perception through the extended recovery phase.
| Time Elapsed | Biological Mechanism | Physical Sensation |
|---|---|---|
| 0.0 - 0.5 Seconds | Amygdala detects sensory threat (via thalamus) and signals the paraventricular nucleus of the hypothalamus. Sympathetic preganglionic neurons fire down the spinal cord. | Instantaneous startle reflex; momentary sensory hyper-focus; sudden cessation of previous thought patterns. |
| 0.5 - 3.0 Seconds | SAM Axis activation. Acetylcholine triggers the adrenal medulla to release stored epinephrine and norepinephrine from chromaffin granules into the bloodstream 910. | Sudden "jolt" of energy or electric feeling; rapid spike in heart rate; initial gasp or sharp, involuntary inhalation of air. |
| 3.0 - 10.0 Seconds | Catecholamines bind to systemic adrenergic receptors. Bronchioles dilate. Vasoconstriction diverts blood away from the splanchnic (digestive) and cutaneous (skin) beds 910. | Heart pounding intensely against the chest wall; breathing becomes rapid and shallow; visceral feeling of "butterflies" or the stomach dropping 91213. |
| 10.0 - 60.0 Seconds | Liver undergoes rapid glycogenolysis, dumping glucose. Adipose tissue undergoes lipolysis. Pupils dilate to enhance peripheral visual acuity 91019. | Extreme muscle tension and jitteriness; cold, pale, or clammy extremities; the mouth goes completely dry (xerostomia) 142315. |
| 1 - 5 Minutes | Hypothalamus initiates the HPA axis by releasing Corticotropin-Releasing Hormone (CRH), which signals the anterior pituitary gland 716. | Sustained hyper-arousal; stress-induced analgesia (pain suppression); tunnel vision; intense, overwhelming urge to fight or flee 1214. |
| 20 - 30 Minutes | HPA Axis peaks. Adrenocorticotropic hormone (ACTH) reaches the adrenal cortex, releasing glucocorticoids (cortisol) to sustain blood glucose and suppress immunity 1718. | Peak sustained alertness; difficulty concentrating on complex, logical cognitive tasks; lingering muscular tension and heightened vigilance. |
| 30 - 120+ Minutes | Negative feedback loop begins if the threat passes. Glucocorticoids bind to brain receptors to halt CRH. Parasympathetic nervous system begins to re-engage 7828. | Gradual decline in heart rate and respiratory rate; onset of physical fatigue, trembling, or exhaustion as circulating adrenaline clears 9. |
Why Is Cortisol Misunderstood, and How Does the HPA Axis Actually Work?
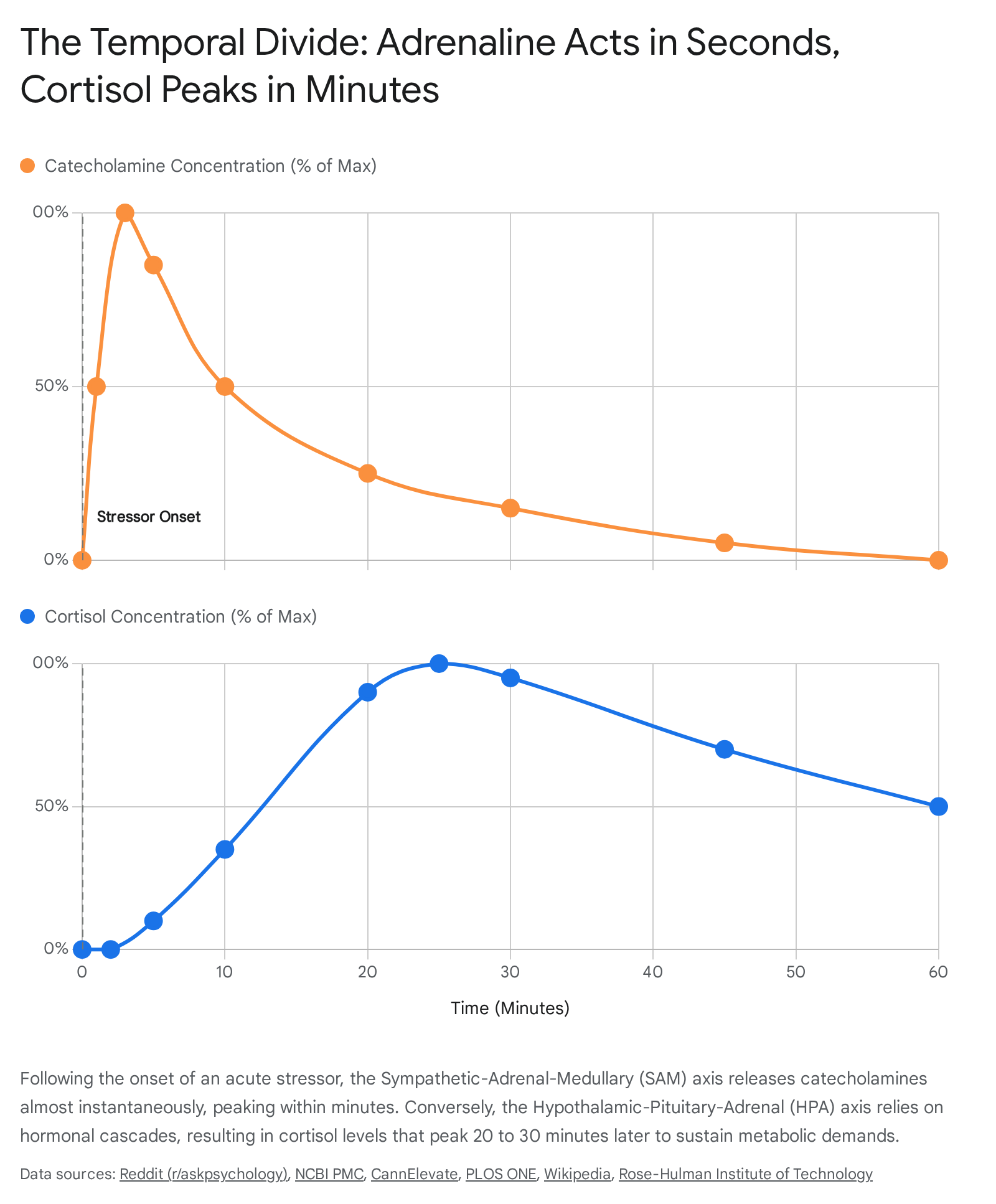
A pervasive misconception in popular psychology and broad wellness narratives is the idea that cortisol acts instantly as a "stress hormone" responsible for the immediate feelings of panic, jitteriness, and a racing heart upon facing a threat. In reality, cortisol is part of the "slow-acting" stress mechanism and has virtually no role in the instantaneous fight-or-flight sensations. Those initial, acute reactions are entirely the domain of the SAM axis and its rapid deployment of catecholamines 1319.
If the SAM axis is the body's rapid-response tactical team, the Hypothalamic-Pituitary-Adrenal (HPA) axis operates as the long-term logistics and supply chain. The HPA axis relies on a sequential cascade of hormonal signals transmitted through the blood rather than electrical impulses fired across synapses, which fundamentally dictates its slower timeline 1314. While the SAM axis acts in mere seconds, the induction of cortisol production requires several minutes, and the full elaboration of cortisol action - which involves altering DNA transcription within target cells - requires several hours. Peak blood concentrations of cortisol typically occur 20 to 30 minutes after the initial onset of the stressor 101719.
When a stressor persists beyond the initial seconds of the SAM response, neurons in the paraventricular nucleus (PVN) of the hypothalamus secrete Corticotropin-Releasing Hormone (CRH) 716. CRH travels via the local hypophyseal portal blood supply directly to the anterior pituitary gland. Here, it prompts the pituitary to synthesize and release Adrenocorticotropic Hormone (ACTH) into systemic circulation 161719. ACTH then travels through the bloodstream to the adrenal cortex - the outer layer of the adrenal glands - stimulating the synthesis and release of glucocorticoids, primarily cortisol in humans 161719.
Cortisol's primary evolutionary function is to keep the body fueled and metabolically adapted for a prolonged ordeal that the initial adrenaline rush could not immediately resolve. Because the brain relies heavily on glucose for energy, cortisol works aggressively to maintain blood sugar levels. It achieves this by stimulating gluconeogenesis - the creation of new glucose from non-carbohydrate sources like amino acids in the liver - and mobilizing fatty acids from adipose tissue for sustained energy 1919. Furthermore, in muscle and adipose tissue, cortisol actively inhibits glucose uptake, ensuring that the brain retains priority access to circulating energy supplies 19.
Simultaneously, cortisol serves as an overriding physiological triage system. It shuts down or suppresses biological processes that are highly energy-consumptive but not immediately critical for surviving the immediate crisis. Consequently, cortisol suppresses reproductive functions, impairs digestive efficiency, and dampens the immune system by reducing inflammation and immune cell activity 14192021. While this temporary immune suppression is adaptive in the short term, redirecting energy to skeletal muscles, chronic cortisol elevation leads to profound health consequences, including muscle wasting, fat redistribution, insulin resistance, and heightened susceptibility to infection 1920. Cortisol also easily passes the blood-brain barrier, directly binding to mineralocorticoid receptors (MR) and glucocorticoid receptors (GR) in the hippocampus and prefrontal cortex, heavily influencing working and long-term memory consolidation during stressful events 17.
How Does the HPA Axis Negative Feedback Loop Regulate Stress?
For the organism to survive long-term, the acute stress response must eventually be deactivated. Without a mechanism to shut off the alarm, the body would suffer from prolonged glucocorticoid toxicity, a condition that degrades cardiovascular tissues, impairs immune function, and causes measurable atrophy and shrinkage in the hippocampus 1632. This critical deactivation process is governed by a highly sensitive, closed-loop negative feedback system.
As circulating cortisol levels rise and fulfill their metabolic duties, the hormone travels back to the brain, crossing the blood-brain barrier. It binds to glucocorticoid receptors (GR) located densely within the hypothalamus, the anterior pituitary, and the hippocampus 81932. This binding acts as a chemical kill-switch. When these receptors detect sufficient levels of plasma cortisol, they send inhibitory signals that prompt the hypothalamus to cease CRH production and the pituitary to halt ACTH secretion. By effectively shutting off its own production line, cortisol successfully terminates the stress response and allows the parasympathetic nervous system to restore homeostatic balance 82819.
Recent neurobiological research from 2024 to 2026 has provided deeper insights into exactly how this negative feedback loop becomes compromised in individuals suffering from chronic stress, major depressive disorder (MDD), and post-traumatic stress disorder (PTSD). Under conditions of persistent, chronic stress, the continuous barrage of cortisol leads to the desensitization or downregulation of glucocorticoid receptors in target tissues, including the brain 162822. When these receptors lose their sensitivity, the brain fails to "hear" the stop signal, resulting in a dysfunctional neuroendocrine status characterized by hyperactivation of the HPA axis and unchecked cortisol secretion. This chronic state of elevated cortisol fuels systemic inflammation and neuroinflammation, driving symptoms of apathy, fatigue, and severe mood dysregulation 61620.
Furthermore, emerging research utilizing mathematical modeling of endocrine circuits has identified a phenomenon known as "dynamical compensation." Studies suggest that prolonged activation of the HPA axis causes HPA hormones to act as growth factors for their downstream glands 23. Over weeks of chronic stress input, the physical, functional mass of the adrenal glands and corticotroph cells in the pituitary actually increases 23. While this physiological adaptation initially attempts to buffer the variation in stress input and return CRH and ACTH to baseline levels, the enlarged glandular mass ultimately exacerbates HPA dysregulation. It alters the axis's sensitivity, deeply linking chronic stress pathophysiology to the structural remodeling of the endocrine system 1623.
The impact of trauma on the HPA axis is not uniform, as individual resilience varies significantly based on genetic predisposition and epigenetic modifications. Exposure to trauma, particularly early life stress (ELS) during sensitive periods of neurodevelopment, can become biologically consolidated. Severe trauma can disrupt the HPA axis's negative feedback loop by causing epigenetic changes - such as DNA methylation and histone modifications - in key genes encoding the glucocorticoid receptor (NR3C1) and its regulatory chaperones (FKBP5) 24. These epigenetic alterations modify receptor sensitivity, leading to diverging patterns of diurnal cortisol regulation. Research indicates that infants exposed to trauma often show delayed cortisol recovery from peak acute stress responses, demonstrating that adverse environmental stimuli can become biologically incorporated into the very structure and function of the developing brain, leaving individuals highly vulnerable to psychiatric illness later in life 525. Paradoxically, in some cases of PTSD, patients exhibit enhanced negative feedback sensitivity resulting in abnormally low baseline cortisol levels, which fails to suppress immune inflammation, creating a vicious cycle where inflammation acts as a further stressor 22.
Why Do the Mouth Go Dry and the Stomach Drop?
The sudden, deeply uncomfortable physical sensations experienced during acute stress - such as a mouth barren of saliva or the visceral feeling of the stomach "dropping" - are direct, mechanical results of the sympathetic nervous system forcibly overriding non-essential bodily functions to guarantee survival.
During the fight-or-flight response, biological priority is strictly assigned to systems necessary for immediate physical action. Saliva production, primarily a function of the parasympathetic "rest and digest" nervous system, is rapidly downregulated 1323. Epinephrine drastically alters local blood flow, causing acute vasoconstriction in the mucosal linings of the mouth and the major salivary glands 2337. Furthermore, cortisol directly blunts the glands' cellular responsiveness to normal neurological stimulation 23. Consequently, the unstimulated salivary flow rate nearly halts, and the pH of any remaining saliva drops, becoming more acidic. This results in acute xerostomia (dry mouth), a sticky, uncomfortable sensation that is universally correlated with high-stress or anxiety-inducing environments, such as public speaking or facing an immediate physical threat 131537.
Similarly, the sensation of the stomach dropping or experiencing "butterflies" is tied to the abrupt and massive diversion of systemic blood flow. The gastrointestinal tract requires immense amounts of highly oxygenated blood to perform the complex tasks of digestion and nutrient absorption. However, digestion is metabolically expensive and entirely useless if the organism is about to be killed. During acute stress, the SAM axis aggressively constricts the splanchnic blood vessels supplying the digestive system 139. This instant routing of blood volume away from the gut and toward the skeletal muscles, heart, and brain causes sudden ischemia (reduction in blood flow) in the gastrointestinal tract. The rapid cessation of gastric motility and the sudden drop in local blood pressure by the sympathetic nervous system manifest subjectively as a hollow, dropping, or fluttering sensation in the abdomen.
Is the Stress Response Strictly Binary? Understanding "Freeze" and "Fawn"
A widespread misconception in both public consciousness and basic biology education assumes that the acute stress response is strictly a binary choice: an organism must either engage in aggressive confrontation (fight) or execute a rapid escape (flight). In reality, evolutionary biology has equipped mammals with a much broader, highly nuanced defense cascade that includes the profound physiological states of "freeze" and "fawn" 6143826. Recognizing these responses is vital for trauma-informed psychology, as they represent adaptive survival strategies rather than signs of weakness or failure.
The Biology of the Freeze Response
When the brain's threat-detection systems identify an overwhelming danger where neither fighting nor fleeing is a viable survival strategy - such as being overpowered by a larger predator or trapped in an inescapable traumatic event - it may invoke the freeze response. Also referred to as tonic immobility, the freeze state is not a conscious cognitive choice; it is an involuntary, highly evolved neurobiological mechanism designed to minimize physical injury, conserve vital energy, and potentially cause a motion-responsive predator to lose interest 6143840.
Biologically, the freeze response represents a complex and highly taxing neurological paradox. It is heavily mediated by the dorsal vagal complex of the parasympathetic nervous system, specifically the unmyelinated dorsal vagal pathway 614. While the parasympathetic system is typically associated with calm relaxation, the dorsal vagal response induces extreme, life-preserving immobilization. However, this immobilization often occurs concurrently with intense sympathetic nervous system arousal. The result is a physiological system under extreme, competing tension - often likened to pressing a car's gas pedal and its brakes simultaneously to the floor 3826.
Physically, this dual activation manifests as extreme muscle rigidity and a dramatic increase in muscle tension, making voluntary movement difficult or impossible. Concurrently, the individual may experience a plunging heart rate (bradycardia) or alternating cardiac rhythms, profound emotional numbing, dissociation, time distortion, and the sensation of being physically paralyzed or mentally "stuck" despite a strong internal desire to act 121438.
The Neurobiology of the Fawn Response
Identified more recently within the context of complex trauma and extensively detailed through frameworks like the Polyvagal Theory, the "fawn" response is a sophisticated survival strategy based on social appeasement. Fawning occurs when an individual seeks safety by actively placating, submitting to, or anticipating the needs of a perceived threat to prevent conflict or harm 6124142.
Unlike the primitive, reptilian immobilization of freezing, the fawn response relies on higher-order social processing and cognitive functioning. It is primarily mediated by the mammalian "social engagement system," which utilizes the myelinated ventral branch of the vagus nerve alongside complex cortico-striatal pathways 4227. Fawning is heavily influenced by the neurobiology of attachment, specifically oxytocinergic and dopaminergic pathways. While oxytocin is frequently simplified in popular science as the "bonding" or "cuddle hormone," it serves a much more fundamental evolutionary purpose: it regulates social salience, meaning it amplifies the detection and processing of social cues to enhance survival through group cohesion and social appeasement 284529.
Current perspectives on the neurobiology of human prosociality suggest that oxytocin interacts intimately with the dopaminergic reward system and endogenous opioids in the striatum and nucleus accumbens 293048. In threatening environments - particularly instances of developmental trauma, chronic childhood abuse, or living with a domineering, volatile caregiver - the nervous system quickly learns that fighting, fleeing, or freezing will only elicit further harm 61440. Consequently, the brain adapts by deploying oxytocin and dopamine to motivate hyper-compliance, over-agreeableness, and the total abandonment of personal boundaries. The individual attempts to neutralize the threat by fusing with the abuser's needs, utilizing the brain's social reward circuitry to forge a trauma bond in a desperate bid for safety 61441. While highly adaptive and brilliantly effective for surviving inescapable interpersonal danger in the short term, chronic fawning profoundly reshapes neural circuitry. Long-term reliance on the fawn response leads to severe psychological distress, pervasive codependency, chronic self-abandonment, and a fractured sense of identity in adulthood 1241.
How Are Recent Neurobiological Breakthroughs Changing Stress Interventions?
Advancements in neurobiology and psychophysiology between 2024 and 2026 have increasingly shifted clinical focus away from strictly pharmacological suppression of symptoms and toward the vagus nerve as a primary intervention point for halting the acute stress response. The vagus nerve (the 10th cranial nerve) acts as the primary anatomical information superhighway of the parasympathetic nervous system, establishing a direct, bi-directional connection between the brain stem and the body's major visceral organs, including the heart, lungs, and digestive tract 484950. It is the biological conduit responsible for shifting the body out of fight-or-flight and into the "rest and digest" state, slowing the heart rate, and restoring internal homeostasis.
Traditionally, manipulating the autonomic nervous system relied heavily on long-term behavioral therapies or systemic psychiatric medications, which often presented side effects or proved inadequate for treatment-resistant populations. However, recent scientific breakthroughs have pioneered the use of neuromodulation technologies, specifically Transcutaneous Auricular Vagus Nerve Stimulation (tVNS), also termed Auricular Vagal Neuromodulation Therapy (AVNT) 495031. Because the auricular branch of the vagus nerve is uniquely accessible just beneath the skin of the outer ear, researchers discovered that applying precise, non-invasive electrical impulses to this specific area directly stimulates the parasympathetic nervous system, bypassing the need for surgical implants previously used only for epilepsy 849.
Robust randomized controlled clinical trials published in 2025 demonstrated the profound efficacy of these devices. Studies on individuals with Generalized Anxiety Disorder (GAD) revealed that just 30 minutes of daily tVNS over several weeks significantly decreased anxiety scores. More importantly, functional MRI (fMRI) brain scans detected actual neural activity regulation in the limbic regions associated with fear and anxiety, proving that the stimulation affects the emotional control centers of the brain directly 50.
Furthermore, data from 2026 highlights the ability of vagus nerve stimulation to address the physical toll of stress. Researchers demonstrated that tVNS activates the cholinergic anti-inflammatory pathway, reducing NF-kB signaling and drastically lowering systemic inflammation, a condition frequently driven by the chronic overactivation of the HPA axis and subsequent cortisol resistance 48. By directly modulating heart rate variability (HRV) and optimizing nervous system function at its root, these non-invasive neuromodulation devices are rapidly advancing from experimental trials to scientifically supported, drug-free modalities for addressing cognitive deficits, severe depression, and generalized anxiety spirals 503132.
What Are Evidence-Based Methods to Manually Signal Safety to the Nervous System?
While medical neuromodulation devices represent the cutting edge of clinical intervention, neurobiological research consistently points to highly practical, behavioral methodologies that allow individuals to effectively "hack" their own autonomic nervous system. By consciously engaging specific physiological and respiratory pathways, it is possible to manually signal safety to the amygdala, effectively halting the SAM axis cascade and preventing the prolonged, toxic activation of the HPA axis 53.
It is critical to note a degree of calibrated uncertainty regarding these behavioral interventions: While large-scale physiological data demonstrates robust efficacy in controlled clinical environments, individual autonomic flexibility varies significantly. Factors such as genetics, severe trauma histories, and baseline allostatic load can alter neuroplasticity and receptor sensitivity. Therefore, these practices may yield highly variable results across individuals and should be viewed as powerful, daily tools for autonomic regulation and resilience-building, rather than absolute, standalone cures for clinical psychiatric disorders.
The Physiological Sigh
Perhaps the most significant behavioral intervention supported by recent literature is the "physiological sigh." In a landmark 2023 randomized controlled trial conducted by neurobiologists at Stanford University School of Medicine (led by Dr. Andrew Huberman and Dr. David Spiegel), researchers sought to directly compare different breathing protocols against traditional meditation 543356. They found that just five minutes of cyclic physiological sighing - a specific, controlled breathing exercise - reduced cortisol levels, significantly decreased resting respiratory rates, and improved mood more effectively than mindfulness meditation of the same duration 5433.
The physiological sigh consists of a very specific respiratory pattern: two sharp inhales through the nose, immediately followed by one long, extended, slow exhale through the mouth 5457. The mechanism behind this practice is exquisitely specific to respiratory neurobiology. Under acute stress, breathing naturally becomes rapid and shallow. This shallow breathing causes the alveoli - the millions of tiny, balloon-like air sacs in the lungs responsible for gas exchange - to partially collapse 5458. When alveoli collapse, the surface area for oxygen exchange decreases, and carbon dioxide begins to build up in the bloodstream. Elevated CO2 is a primary chemical signal that triggers the brain's suffocation alarm, drastically heightening the panic and stress response 5433.
The first deep inhale brings air into the lungs, but the crucial second, shorter "sniff" or inhale mechanically forces the partially collapsed alveoli to pop open and reinflate, maximizing the lungs' internal surface area 5458.
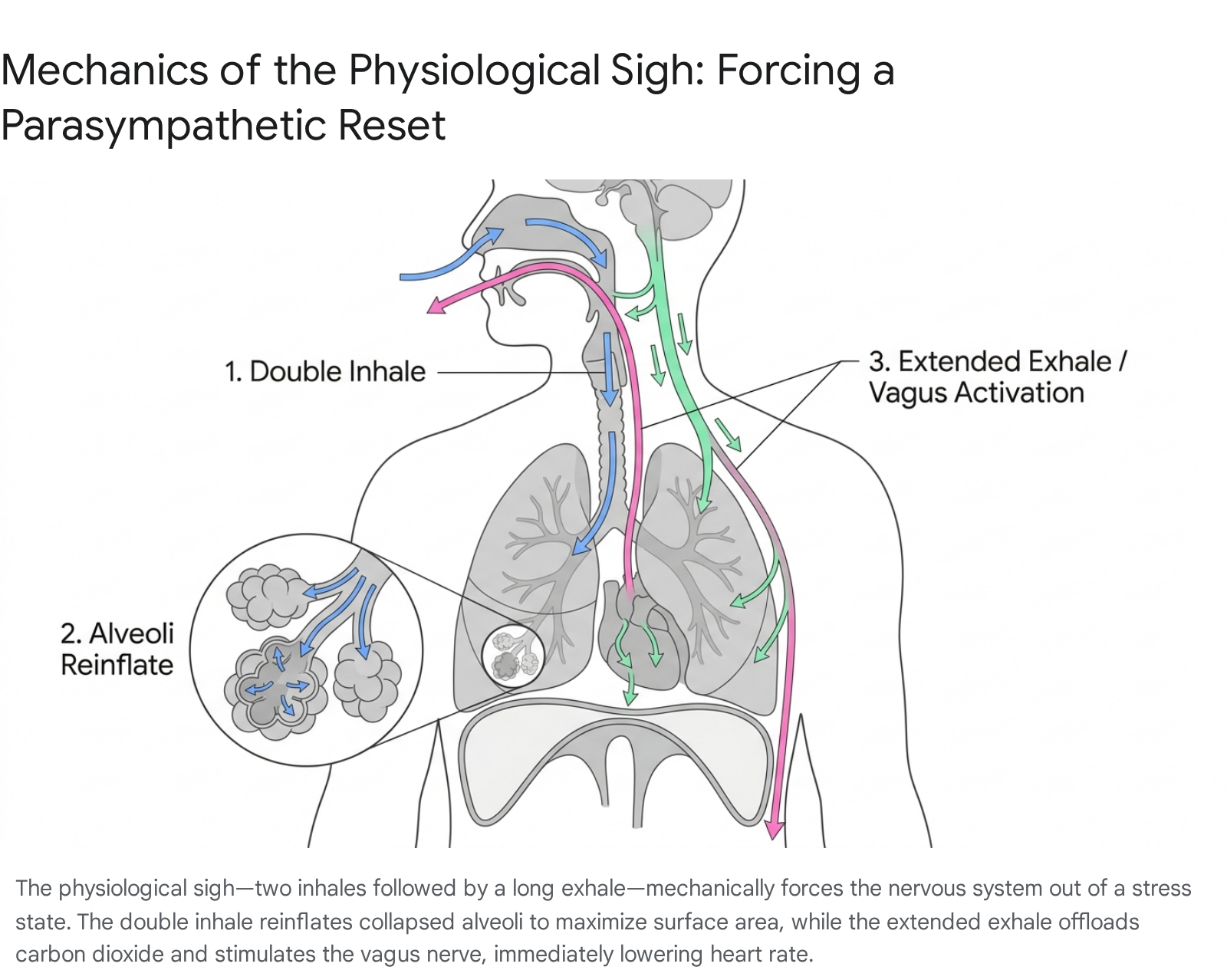
The subsequent extended, slow exhale serves two vital purposes: it rapidly and efficiently offloads the excess, panic-inducing carbon dioxide, and it mechanically stimulates the vagus nerve. As the diaphragm moves upward slowly during a long exhalation, it triggers parasympathetic signaling to the sinoatrial node of the heart, resulting in an immediate, measurable drop in heart rate 54335657.
Thermal and Tactile Interventions
Beyond breathwork, manipulating sensory input through temperature and touch offers additional pathways to neuro-regulation. Cold exposure is a highly effective modality for intercepting the stress response and improving vagal tone. Splashing cold water on the face, applying ice to the lateral pulse points of the neck, or engaging in short-term cold water immersion actively stimulates the trigeminal and vagus nerve pathways 44959. The sudden thermal shock to the skin prompts a physiological adaptation similar to the mammalian dive reflex. This reflex rapidly shunts blood flow away from the periphery to preserve core temperature, drastically slows down the heart rate, and dampens the sympathetic stress response at a systemic level, forcing the body into a state of physical conservation 459.
Furthermore, tactile stimulation mimicking social touch has profound neurobiological effects. Cutaneous perception, particularly slow, gentle stroking or massage of the neck, shoulders, and feet, activates sensory nerves that stimulate the release of endogenous oxytocin 445. Because oxytocin dampens amygdala reactivity and lowers cortisol levels, this sensory stimulation effectively signals safety to the brain, countering the HPA axis's stress cascade and promoting psychological resilience 284534.
Bottom Line
The acute stress response is a spectacular evolutionary achievement, perfectly tuned to prioritize immediate biological survival through a highly choreographed cascade of neural and endocrine events. However, our modern environment continually triggers these ancient SAM and HPA pathways with non-lethal psychosocial stressors, leading to systemic allostatic load, severe inflammation, and chronic neuroendocrine dysregulation. By understanding the exact physiological timeline - from the immediate, adrenal-fueled panic of the SAM axis to the sustained, cortisol-driven arousal of the HPA axis, as well as the nuanced reality of freeze and fawn adaptations - individuals and clinicians can move beyond symptom management. Utilizing targeted, evidence-based interventions, such as transcutaneous vagus nerve stimulation, cold exposure, and the physiological sigh, it is increasingly possible to manually override the nervous system, restore the negative feedback loop, and effectively signal biological safety to a paleolithic brain navigating a modern world.