Why Pelacarsen is the Heart Trial to Watch in 2026
The upcoming Phase 3 Lp(a)HORIZON trial readout at the ESC Congress 2026 in Munich is a landmark event because it is the first cardiovascular outcomes study to test a therapy specifically designed to lower Lipoprotein(a). If the results demonstrate that pelacarsen reduces major adverse cardiovascular events, it will definitively prove that drastically lowering this genetic lipid prevents heart attacks and strokes. This readout promises to transform cardiovascular care by validating a new, targetable pathway for the millions of patients who remain at risk despite receiving optimal standard-of-care treatments.
What is Lipoprotein(a) and Why is it the "Hidden" Cholesterol?
For decades, public health initiatives and preventative cardiology have focused relentlessly on lowering low-density lipoprotein (LDL), commonly known as "bad" cholesterol. However, despite achieving target LDL-C levels through aggressive statin therapy and optimal lifestyle modifications, a significant proportion of patients continue to suffer from recurrent myocardial infarctions and ischemic strokes 12. This phenomenon of residual cardiovascular risk has increasingly been linked to a genetically determined, highly atherogenic lipid known as Lipoprotein(a), or Lp(a) 34.
Lp(a) acts as a "hidden" cholesterol because it operates entirely outside the boundaries of traditional cardiovascular risk factors. It is the strongest genetic risk factor for heart disease, affecting approximately 20% of the global population - amounting to roughly 1.4 billion people worldwide 156. Meaning that up to 1 in 5 individuals carry elevated levels of this dangerous particle 16. The defining and most frustrating characteristic of Lp(a) is its resistance to conventional interventions. Because Lp(a) serum concentrations are almost entirely dictated by the LPA gene, lifestyle modifications such as adopting a heart-healthy diet, maintaining a healthy weight, or initiating rigorous exercise programs have virtually no impact on its levels 278.
Furthermore, standard lipid-lowering medications, including statins, ezetimibe, and bempedoic acid, are entirely ineffective at reducing Lp(a); in some documented cases, traditional statins may even cause a slight, paradoxical increase in Lp(a) concentrations 689. Until recently, therapeutic options were limited to lipoprotein apheresis - a costly, burdensome, dialysis-like procedure reserved for the most extreme cases of recurrent cardiovascular disease 210.
Why Do Standard Lipid Panels Fail to Detect Lp(a)?
A widespread and dangerous clinical misconception is the assumption that routine, annual blood work accounts for all dangerous lipids. It is crucial to explicitly correct the misconception that standard lipid panels check for Lp(a) 7. Routine panels measure total cholesterol, high-density lipoprotein (HDL), triglycerides, and calculated LDL-C. Because an Lp(a) particle contains a cholesterol core, its cholesterol mass is inextricably lumped into the standard LDL-C measurement 411.
Therefore, a standard lipid panel cannot distinguish between normal LDL cholesterol and the highly atherogenic Lp(a) cholesterol. A patient could present with seemingly pristine traditional cholesterol metrics while unknowingly harboring dangerously high levels of Lp(a) 713. Unless a physician explicitly orders a specific, standalone blood assay for Lipoprotein(a) - typically billed under CPT® Code 83695 in the United States - this genetic risk factor remains completely invisible, leaving patients to walk a tightrope of cardiovascular risk without a safety net 71314.
How Does the "Sticky Velcro" Particle Drive Heart Disease?
To understand why Lp(a) is uniquely destructive to the cardiovascular system, one must examine its molecular architecture. Structurally, an Lp(a) particle begins as a standard LDL particle, containing a lipid core and a primary surface protein known as apolipoprotein B-100 (apoB) 1512. However, what distinguishes Lp(a) is the presence of an additional, highly specialized protein called apolipoprotein(a), or apo(a), which is covalently bound to the apoB protein via a single disulfide bridge 2412.
This extra apo(a) tail effectively transforms a standard cholesterol molecule into a "sticky velcro" particle. The apo(a) component shares a striking structural and genetic similarity to plasminogen, a naturally occurring proenzyme responsible for dissolving blood clots (fibrinolysis) 413. Because of this structural mimicry, Lp(a) competes with plasminogen for binding sites, interfering with the body's natural clot-dissolving processes and creating a highly prothrombotic environment 24.
Simultaneously, the "sticky velcro" nature of the apo(a) protein causes the particle to aggressively adhere to the endothelial walls of blood vessels. Once trapped within the arterial intima, Lp(a) acts as a trojan horse, carrying highly reactive oxidized phospholipids (OxPL) directly into the tissue 1311. These oxidized lipids are potent instigators of localized vascular inflammation, driving rapid plaque accumulation (atherogenesis), plaque vulnerability, and eventually, calcific aortic valve stenosis 23. Therefore, Lp(a) delivers a devastating triple-threat to cardiovascular health: it accelerates the buildup of arterial plaque, stokes chronic systemic inflammation, and prevents the breakdown of dangerous blood clots 24.
What is Pelacarsen and How Does its RNA-Targeting Mechanism Silence the Gene?
Because the "sticky velcro" tail of Lp(a) makes it a structurally complex and genetically locked target, traditional small-molecule pharmacology struggled for decades to find a viable mechanism to neutralize it. The breakthrough arrived through the advent of RNA-targeted therapeutics, specifically antisense oligonucleotides (ASOs). Pelacarsen, developed jointly by Ionis Pharmaceuticals and Novartis, represents the vanguard of this new class of genetic medicines 1418.
Pelacarsen acts directly at the source of Lp(a) production: the liver 3619. Rather than attempting to clear Lp(a) from the bloodstream after it has already been manufactured, pelacarsen functions as a molecular "stop order" on the genetic assembly line. The drug is engineered using proprietary ligand-conjugated antisense (LICA) technology, featuring a specialized triantennary N-acetylgalactosamine (GalNAc3) delivery system 315. This GalNAc complex acts as a molecular homing beacon, binding exclusively to asialoglycoprotein receptors found heavily on the surface of hepatocytes (liver cells). This ensures the drug is delivered directly into the liver while minimizing off-target systemic exposure and significantly enhancing its potency 315.
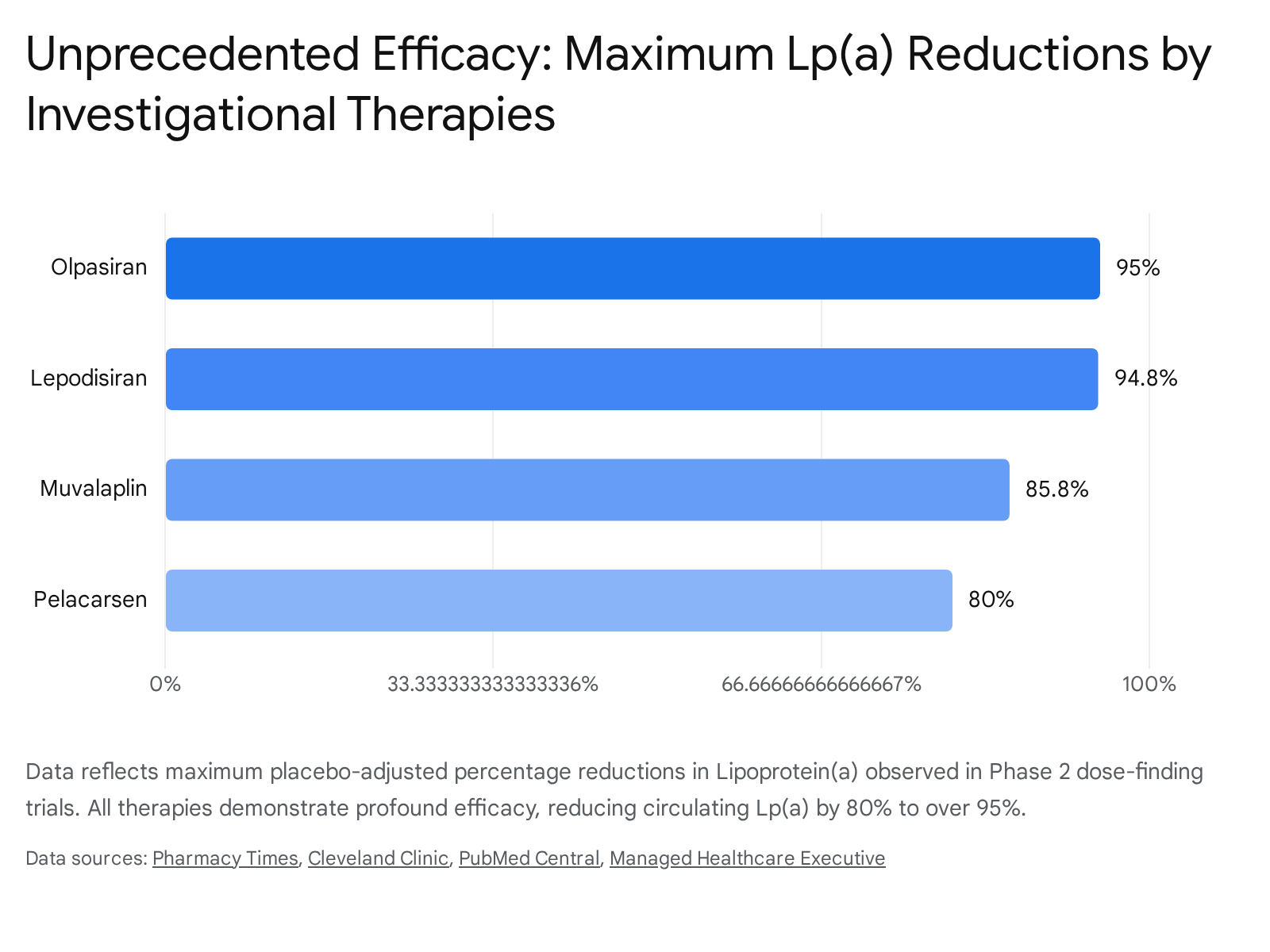
Once inside the liver cell's nucleus, the antisense oligonucleotide binds with high precision to the specific messenger RNA (mRNA) that carries the genetic blueprint for the apolipoprotein(a) protein 319. This binding forms an abnormal DNA-RNA heteroduplex. The cell's innate defense systems recognize this hybrid as unnatural and deploy an enzyme called RNase H to cleave and destroy the targeted mRNA 31915. By silencing the gene and destroying the mRNA blueprint, the liver cannot synthesize the apo(a) protein. Because the "sticky velcro" tail is never manufactured, the complete Lp(a) particle cannot be assembled 318. As a result, circulating serum concentrations of Lp(a) plummet. In Phase 2 dose-finding trials, subcutaneous administration of pelacarsen reduced Lp(a) by approximately 80%, with 98% of patients achieving levels below the 50 mg/dL risk threshold 4611. Furthermore, the Phase 3 Lp(a)FRONTIERS APHERESIS trial demonstrated that pelacarsen reduced the need for invasive lipoprotein apheresis sessions by 72% over a 52-week period 101622.
What Can We Expect from the Lp(a)HORIZON Trial at ESC Congress 2026?
The European Society of Cardiology (ESC) Congress, scheduled for August 28 to 31, 2026, in Munich, Germany, is widely recognized as the world's premier cardiovascular medicine event, routinely drawing over 30,000 scientists, clinicians, and health policy leaders 172425. The 2026 congress will feature a thematic spotlight on the integration of artificial intelligence in cardiology, focusing on digital workflows, risk prediction, and automated imaging analysis 181920. However, the undisputed focal point of the scientific program will be the highly anticipated Late-Breaking Science Hot Line sessions, held in the main auditorium 192122.
These Hot Line sessions are reserved exclusively for the first-time presentations of primary endpoints from transformative, recently completed clinical trials 22. It is here that the global cardiovascular community expects to witness the unblinding of the pivotal Phase 3 Lp(a)HORIZON trial (NCT04023552) 142324.
Initiated in December 2019, Lp(a)HORIZON is an event-driven, randomized, double-blind, placebo-controlled cardiovascular outcomes trial. The study enrolled 8,323 patients globally who possess established atherosclerotic cardiovascular disease (ASCVD) - defined by a prior myocardial infarction, ischemic stroke, or symptomatic peripheral artery disease - and markedly elevated Lp(a) concentrations of at least 70 mg/dL (approximately 175 nmol/L) 62433. Patients were randomized to receive either an 80 mg subcutaneous injection of pelacarsen once a month or a matching placebo, added on top of maximally tolerated standard-of-care medical therapies like high-intensity statins 1125.
The primary endpoint of the trial is the time to the first occurrence of major adverse cardiovascular events (MACE), a composite that includes cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, and urgent coronary revascularization requiring hospitalization 2535.
The significance of the Lp(a)HORIZON readout in Munich cannot be overstated. While Phase 2 trials have already proven that pelacarsen safely lowers the biological marker of Lp(a), the medical community requires definitive proof that this biochemical reduction translates into actual clinical survival benefits 626. If the trial meets its primary endpoints, Novartis intends to submit a New Drug Application (NDA) in the second half of 2026 614. A successful outcome will not only validate pelacarsen as a first-in-class therapy but will also validate the entire "lipid hypothesis" for Lp(a), proving that the particle is a highly actionable therapeutic target.
What Are the Competing Therapies in the Lp(a) Pipeline?
While pelacarsen benefits from a first-mover advantage, it is far from the only therapy progressing toward clinical implementation. Recognizing the massive unmet need, several major pharmaceutical developers are advancing competing technologies that broaden the pipeline by offering distinct advantages regarding dosing frequency, mechanisms of action, and administration routes.
Olpasiran (Amgen)
Rather than utilizing an ASO mechanism, Amgen's olpasiran is built on small interfering RNA (siRNA) technology 637. While both ASOs and siRNAs ultimately degrade apolipoprotein(a) mRNA, siRNA operates by harnessing a different cellular pathway, known as the RNA-induced silencing complex (RISC), which can sometimes offer highly durable, prolonged gene silencing with less peak-to-trough variability 3839. In Phase 2 trials (OCEAN(a)-DOSE), olpasiran demonstrated astonishing potency, lowering Lp(a) concentrations by more than 95% at doses of 75 mg or higher 63727. Due to this durability, olpasiran requires administration via subcutaneous injection only once every 12 weeks 6. Amgen's Phase 3 cardiovascular outcomes trial, OCEAN(a)-Outcomes (NCT05581303), is currently tracking 7,297 patients, with a primary completion date projected for March 2028, though early data reads may surface sooner 4128.
Lepodisiran (Eli Lilly)
Following closely in the GalNAc-conjugated siRNA class is Eli Lilly's lepodisiran. Early trial data suggests lepodisiran achieves massive, long-lasting reductions in Lp(a) levels - up to 94.8% below baseline after just two doses 29. The extreme durability of this siRNA therapy allows for highly infrequent dosing: injections can be administered as sparsely as once every six months, dramatically reducing the clinical burden on patients compared to monthly injections 629. Eli Lilly has initiated the massive Phase 3 ACCLAIM-Lp(a) outcomes trial (NCT06292013), which expects to enroll over 17,000 patients and notably includes both secondary prevention cohorts and primary prevention cohorts (patients aged 55 or older who have high risk factors but have not yet suffered a cardiovascular event) 26293031.
Muvalaplin (Eli Lilly)
Perhaps the most disruptive entry in the pipeline is muvalaplin, also developed by Eli Lilly. Unlike pelacarsen, olpasiran, and lepodisiran, which are injectable RNA-targeted therapies that act in the nucleus, muvalaplin is an oral, once-daily small molecule pill 5646. It operates through an entirely different mechanism: rather than silencing the gene, muvalaplin physically blocks the non-covalent bonding of apo(a) to apoB, preventing the final assembly of the "sticky velcro" Lp(a) particle entirely 13346. In the Phase 2 KRAKEN trial, the highest daily dose (240 mg) reduced Lp(a) levels by up to 85.8% with little to no safety or tolerability concerns 525. Muvalaplin recently entered the Phase 3 MOVE-Lp(a) trial (NCT07157774), aiming to enroll 10,450 patients globally 2532. As a daily oral medication, muvalaplin could bypass the apprehension some patients have regarding injections, drastically expanding global therapeutic access 1333.
| Drug Candidate | Developer | Mechanism / Class | Dosing Method & Frequency | Current Trial Phase | Trial Name (Registry ID) |
|---|---|---|---|---|---|
| Pelacarsen | Novartis / Ionis | Antisense Oligonucleotide (ASO) | Subcutaneous injection, Monthly (80 mg) | Phase 3 | Lp(a)HORIZON (NCT04023552) |
| Olpasiran | Amgen | Small Interfering RNA (siRNA) | Subcutaneous injection, Every 12 weeks | Phase 3 | OCEAN(a)-Outcomes (NCT05581303) |
| Lepodisiran | Eli Lilly | Small Interfering RNA (siRNA) | Subcutaneous injection, Every 6 months | Phase 3 | ACCLAIM-Lp(a) (NCT06292013) |
| Muvalaplin | Eli Lilly | Small Molecule Inhibitor | Oral pill, Once daily | Phase 3 | MOVE-Lp(a) (NCT07157774) |
| Zerlasiran | Silence Therapeutics | Small Interfering RNA (siRNA) | Subcutaneous injection, Every 16-24 weeks | Phase 2 Completed | ALPACAR-360 (NCT05305664) |
What Are the Current Medical Guidelines for Lp(a) Screening?
While the medical community awaits the definitive outcome data from ESC 2026, preventative strategies are already shifting to accommodate the imminent arrival of Lp(a) therapies. Recognizing that knowledge is the crucial first step to prevention, major international cardiology guidelines have fundamentally rewritten their stance on Lp(a) screening.
The 2025/2026 Focused Update of the ESC and European Atherosclerosis Society (EAS) guidelines on dyslipidemia explicitly establishes elevated Lp(a) as a powerful cardiovascular risk-enhancing factor 4934. Because Lp(a) levels are nearly 90% determined by genetics and remain stubbornly stable throughout a person's adult life, the guidelines formally recommend that every adult should undergo an Lp(a) test at least once in their lifetime 2735. The practical takeaway is straightforward: this test is easily achieved by asking a healthcare provider to append the Lp(a) specific blood assay to a routine lipid panel 71314.
According to the latest consensus, Lp(a) concentrations are interpreted via absolute risk thresholds, prioritizing molar measurements. The ESC/EAS guidelines specify that an Lp(a) concentration greater than 50 mg/dL (or ≥105 nmol/L) should actively reclassify a patient's risk profile, pushing intermediate-risk patients into higher risk categories that require more aggressive preventive management under the new SCORE2/SCORE2-OP risk prediction algorithms 495236. Similarly, the American College of Cardiology and the American Heart Association (ACC/AHA) recognize a threshold of ≥125 nmol/L as a significant risk-enhancing factor 712.
Until specific Lp(a)-lowering drugs like pelacarsen or muvalaplin secure regulatory approval, clinical guidelines advise that patients with elevated Lp(a) must be subjected to ultra-intensive management of all other modifiable risk factors. This involves aggressively driving down LDL-C with statins or PCSK9 inhibitors to baseline reductions of 50% or more (often targeting <40 mg/dL for extreme risk), strictly controlling blood pressure, managing diabetes, and entirely avoiding tobacco 2754. Furthermore, because Lp(a) is highly heritable, discovering elevated levels in one individual should trigger "cascade screening" - systematically testing the patient's parents, siblings, and children to identify and manage hidden risk within the family tree 7.
Bottom Line
The field of cardiology is standing on the precipice of a major paradigm shift. For generations, Lipoprotein(a) has lurked in the background as an untreatable, hidden genetic driver of heart attacks, strokes, and aortic stenosis. The development of advanced gene-silencing technologies and small molecule inhibitors has finally provided the pharmacological tools necessary to dismantle this dangerous "sticky velcro" particle.
When the ESC Congress 2026 convenes in Munich, the global medical community will look to the Phase 3 Lp(a)HORIZON data for definitive proof that reducing Lp(a) with pelacarsen translates to tangible human survival benefits. If successful, the trial will not only validate a first-in-class therapy but will fling open the doors for an entire pipeline of innovative, highly potent drugs - from ultra-long-acting injectables like olpasiran and lepodisiran to accessible daily pills like muvalaplin. Ultimately, the successful neutralization of Lp(a) represents one of the most promising frontiers in the ongoing battle to conquer residual cardiovascular risk and eradicate preventable heart disease.