How to Read Cardiovascular News Without the Jargon
The anticipated outcomes from the European Society of Cardiology (ESC) Congress 2026 herald a transition from generalized cardiovascular management to targeted metabolic and genetic interventions, defined by the expected validation of Lipoprotein(a) gene-silencers like pelacarsen. Simultaneously, the congress is poised to consolidate multi-receptor incretin agonists and non-steroidal mineralocorticoid receptor antagonists as the undisputed foundational therapies for hard-to-treat heart failure phenotypes. These results represent a fundamental shift from reactive symptom control to proactive, disease-modifying therapies that target the underlying genetic and metabolic drivers of atherosclerosis and myocardial stiffening.
The findings announced at this conference often dictate the blood pressure or cholesterol medications your doctor will prescribe for years to come. Because the decisions made in the wake of this congress will reshape global clinical guidelines, understanding the rigorous science behind these imminent headlines is paramount - not just for practitioners adjusting their clinical algorithms, but for patients actively managing their lifelong cardiovascular risk trajectories.
As of this writing in May 2026, the ESC Congress in Munich is scheduled to occur in late August 2026 11. Because the conference has not yet taken place, the full, embargoed datasets from the event's premier "Hot Line" trials remain unpublished. Therefore, this exhaustive research report pivots to analyze the rigorous preparatory data, the anticipated readouts of field-defining trials, and the evolving cardiometabolic landscape leading up to the congress. Furthermore, this document serves as a comprehensive media-literacy toolkit designed to help clinicians, analysts, and patients accurately interpret the impending wave of cardiovascular news.
What makes a trial 'late-breaking'?
Every year, the ESC Congress attracts tens of thousands of healthcare professionals, researchers, and pharmaceutical analysts, cementing its status as the largest and most influential cardiovascular gathering globally 12. The scientific core of this congress revolves around its "Late-Breaking Science" and "Hot Line" sessions. In clinical research, a trial is designated as "late-breaking" when its primary data are so novel, impactful, and recently completed that they bypass standard abstract submission deadlines, ensuring the medical community receives practice-changing information as rapidly as possible 1.
The "Hot Line" sessions at the ESC Congress represent the absolute pinnacle of this category. Reserved exclusively for the first public presentation of the primary endpoints of large-scale, novel clinical trials, these sessions are highly orchestrated events 13. Typically, the principal investigator presents the data live in the main auditorium, immediately followed by an independent review from a renowned expert who contextualizes the findings 13. Because these trials possess the statistical power and methodological rigor to alter global clinical practice guidelines - such as the ESC Guidelines for the Management of Heart Failure or Cardiovascular Disease - they are subject to strict media embargoes 15.
To guarantee data integrity, the findings are often published simultaneously in top-tier peer-reviewed journals, such as The New England Journal of Medicine or The Lancet. This synchronization ensures that the global medical community can scrutinize the methodology the exact moment the headline hits the news cycle 64. The scrutiny applied to these trials is intense and necessary. For example, previous highly publicized studies like the EXCEL trial (comparing stents to open-heart surgery) faced rigorous post-publication investigation by journalists and independent medical boards over outcome definitions and mortality signals, highlighting exactly why unblinded, peer-reviewed data must accompany any bold clinical claims 8. The rigorous structure of the ESC Hot Line sessions is specifically designed to withstand this level of global scrutiny.
Translating the Science: A Cardiology Jargon Glossary
To interpret the anticipated data from ESC 2026 accurately, one must first demystify the dense statistical and physiological jargon utilized by trialists. Understanding these terms is essential for distinguishing between a drug that merely changes a laboratory value and a drug that actively extends human life. The following table translates the most critical terms into plain English using accurate, real-world analogies.
| Clinical Jargon | Medical Definition | Real-World Analogy |
|---|---|---|
| Ejection Fraction (EF) | The volumetric fraction of fluid (blood) pumped out of the heart's left ventricle with each contraction. Normal is typically $\geq 50\%$. | Squeezing a wet sponge. If the sponge is full of water and you squeeze out half of it, your "ejection fraction" is 50%. A weak squeeze (HFrEF) leaves too much water behind, while a stiff sponge (HFpEF) cannot fill with enough water in the first place. |
| Hazard Ratio (HR) | A statistical measure representing the relative risk of an event happening in a treatment group compared to a control group over time. An HR of 0.80 means a 20% risk reduction. | Two runners racing. If Runner A has a hazard ratio of 0.80 compared to Runner B for crossing the finish line, Runner A is crossing the finish line at 80% of the speed of Runner B. |
| Composite Endpoint | A single metric that combines multiple clinical outcomes (e.g., cardiovascular death, non-fatal stroke, or heart attack) to increase the statistical power of a trial. | Failing a car safety inspection. A car fails if the brakes are bad, or the tires are bald, or the engine stalls. The "composite" outcome is the failure, regardless of which specific part caused it. |
| MACE | Major Adverse Cardiovascular Events. Typically a 3-point composite of cardiovascular death, non-fatal myocardial infarction (heart attack), and non-fatal stroke. | The "Big Three" disasters. It is the ultimate scorecard used by regulatory bodies like the FDA and EMA to prove a new drug actually prevents catastrophic events, rather than just changing a surrogate lab number. |
| Observational Study | Research that observes the outcomes of patients in real-world settings without randomly assigning them to a treatment or placebo. Prone to confounding variables. | Watching shoppers at a grocery store. You might notice people buying organic food also buy more yoga mats. You observed a link, but you haven't proven that eating organic food causes you to do yoga. |
How can I spot overhyped heart news?
When major conferences like the ESC Congress occur, global media outlets are inundated with press releases from pharmaceutical companies and academic institutions. In the rush to publish, nuanced scientific findings are frequently reduced to sensational headlines. A critical component of modern medical literacy is recognizing the profound difference between a highly controlled, randomized clinical trial (RCT) that proves causality, and an exploratory observational finding that merely suggests a correlation.
Explicitly correcting common public misconceptions is vital. For instance, the public often confuses an early-stage Phase 1 trial - designed purely to test if an experimental drug is safe in a few dozen healthy volunteers or highly selected patients - with a proven cure ready for the neighborhood pharmacy. Similarly, relative risk reductions are frequently highlighted by public relations departments to make effects sound larger than they genuinely are in clinical practice (e.g., proclaiming a "Drug cuts heart attack risk by 50%!" when the absolute risk only dropped from a 2% baseline to a 1% baseline).
The following media literacy toolkit is designed to help readers navigate the upcoming barrage of cardiology news, contrasting typical media sensationalism with actual clinical context based on recent and anticipated trial readouts.
| Media Headline | Actual Clinical Finding | The Missing Context & Corrected Misconception |
|---|---|---|
| "New Gene Editing Shot Cures High Cholesterol Forever!" | A Phase 1 trial of CRISPR-Cas9 (e.g., CTX310 targeting ANGPTL3) safely reduced LDL cholesterol and triglycerides by roughly 50% in 15 humans 9. | Misconception: The drug is a proven cure available today. Reality: This represents proof-of-concept for safety. It requires years of Phase 3 testing on thousands of patients to ensure it actually prevents heart attacks without off-target genetic effects 9. |
| "Smartwatches Can Now Diagnose Heart Failure!" | An AI algorithm analyzing wearable ECG and photoplethysmography data identified patients at risk for left ventricular dysfunction with high sensitivity 9. | Misconception: Your consumer watch replaces your cardiologist. Reality: Wearables are excellent population-level screening tools that flag potential issues, but formal diagnosis and treatment initiation still require clinical echocardiography and physician evaluation 9. |
| "Popular Weight Loss Drug Halves Heart Disease Risk!" | An observational analysis (e.g., using the TriNetX network) showed patients initiating tirzepatide had fewer acute heart failure hospitalizations than those not on the drug 10. | Misconception: Observational data equates to definitive proof. Reality: While likely true, observational studies cannot account for the "healthy user bias" (people who seek expensive weight loss drugs may also have better baseline healthcare). Only randomized trials like SUMMIT provide definitive proof 10115. |
| "Common Blood Pressure Pill Found Useless After Heart Attacks" | The REBOOT and REDUCE-AMI trials showed routine beta-blockers offered no prognostic benefit to patients whose heart function remained normal after an uncomplicated heart attack 6. | Misconception: Everyone should immediately stop taking beta-blockers. Reality: Beta-blockers are still absolutely lifesaving for patients with reduced ejection fraction or malignant arrhythmias. This finding only applies to a very specific, low-risk subset of patients 6. |
The Global Media Landscape: How Geography Shapes the Narrative
The interpretation of the data emerging from ESC 2026 will vary dramatically depending on the geographic origin of the media outlet. Analyzing these diverse perspectives reveals how different regional health systems prioritize medical innovation, allocate healthcare spending, and address their unique demographic challenges.
North American Media: The Financialization of Innovation
Media outlets in the United States, alongside specialized financial biopharma publications, generally view major clinical trials through the lens of commercial implications, market dominance, and cutting-edge biotechnology. Coverage will heavily emphasize the GLP-1 and dual-agonist market wars between Eli Lilly (tirzepatide) and Novo Nordisk (semaglutide). With Eli Lilly generating approximately $16.4 billion in combined Mounjaro and Zepbound revenue in 2024, North American reporting often frames clinical outcomes - such as tirzepatide's success in the SUMMIT trial - as catalysts for stock prices and drivers of national healthcare expenditure debates 1114. Additionally, US media closely tracks the rapid advancement of CRISPR gene-editing technologies and novel RNA-interference drugs, viewing them as paradigm-shifting - albeit incredibly expensive - cures that challenge the traditional insurance reimbursement models 9.
European Media: Public Health and Systemic Equity
European coverage, driven by publicly funded healthcare systems and guided by the ethos of the ESC itself, tends to prioritize public health, preventive medicine, and systemic inequalities over raw commercial success. Reports from European outlets frequently highlight data from the ESC Atlas of Cardiology, an extensive epidemiological effort that recently revealed cardiovascular disease remains responsible for over 3 million deaths and 68 million healthy life-years lost annually in ESC member nations 7.
European media also sharply focuses on care disparities; recent press releases emphasize the profound female disadvantage in cardiac care, noting that while 40% of cardiologists are women, only 11.5% of interventional cardiologists and 8.8% of cardiac surgeons are women 7. Furthermore, European reporting places significant weight on the environmental determinants of cardiovascular health, frequently covering trials and registry data linking air pollution and ultra-processed foods to the rising burden of cardiometabolic disease 78. Consequently, expect European media to heavily scrutinize whether expensive new therapies presented at the Hot Line sessions are cost-effective enough to be adopted equitably by national health services.
Asian Media: Aging Demographics and Technological Integration
Geographically diverse coverage from Asia reveals a strong focus on precision medicine, artificial intelligence, and managing the monumental burden of rapidly aging populations. In Singapore, media outlets like The Straits Times emphasize proactive, population-level screening initiatives, such as "Project Reset." This ambitious $25 million program leverages artificial intelligence and cardio-liver-metabolic biomarkers to uncover silent, asymptomatic heart disease in over 10,000 seemingly healthy individuals aged 40 to 70 9. The region also closely follows minimally invasive technological advancements, such as the implementation of the Pascal transcatheter valve repair system at the National Heart Centre Singapore, which allows elderly, high-risk patients to undergo mitral valve repair without the trauma of open-heart surgery 10.
Furthermore, Japan's media landscape reflects its unique demographic challenges. Outlets like the Asahi Shimbun and The Japan Times have provided extensive coverage of the ethical complexities surrounding new national guidelines proposed by the Japanese Association for Acute Medicine. These guidelines focus on procedures for determining when to end life-sustaining treatments for patients with end-stage heart failure - a stark contrast to Western media's near-exclusive focus on acute, life-prolonging interventions, highlighting a cultural and medical necessity to balance technological capability with dignified palliative care 11.
Anticipated Major Trials at ESC 2026: The "Hot Line" Watchlist
While the final data from the Munich congress remains under embargo, the cardiovascular community's expectations are firmly anchored on several key therapeutic areas. Based on preceding Phase 2 data, trial design publications, and interim analyses, the following developments are poised to dominate the scientific narrative and subsequently rewrite clinical guidelines.
The Lipoprotein(a) Revolution: The Lp(a)HORIZON Trial
Perhaps the most universally anticipated event in preventive cardiology for 2026 is the readout of the Lp(a)HORIZON trial. For decades, Lipoprotein(a) - or Lp(a) - has been the most frustrating "silent killer" in clinical lipidology.
Lp(a) is structurally similar to standard low-density lipoprotein (LDL), but it is covalently bound to a highly atherogenic, pro-inflammatory, and pro-thrombotic protein called apolipoprotein(a) 1221. The size of this particle is determined largely by the number of Kringle IV type 2 repeats in the LPA gene 2113. Because Lp(a) levels are up to 90% genetically determined, they remain stubbornly resistant to lifestyle modifications; no amount of diet, exercise, or traditional statin therapy will meaningfully lower it 2114. Elevated Lp(a) affects roughly 20% of the global population and is recognized by the European Atherosclerosis Society as a causal, independent risk factor for premature atherosclerosis, myocardial infarction, and rapid progression of aortic valve stenosis 131415.
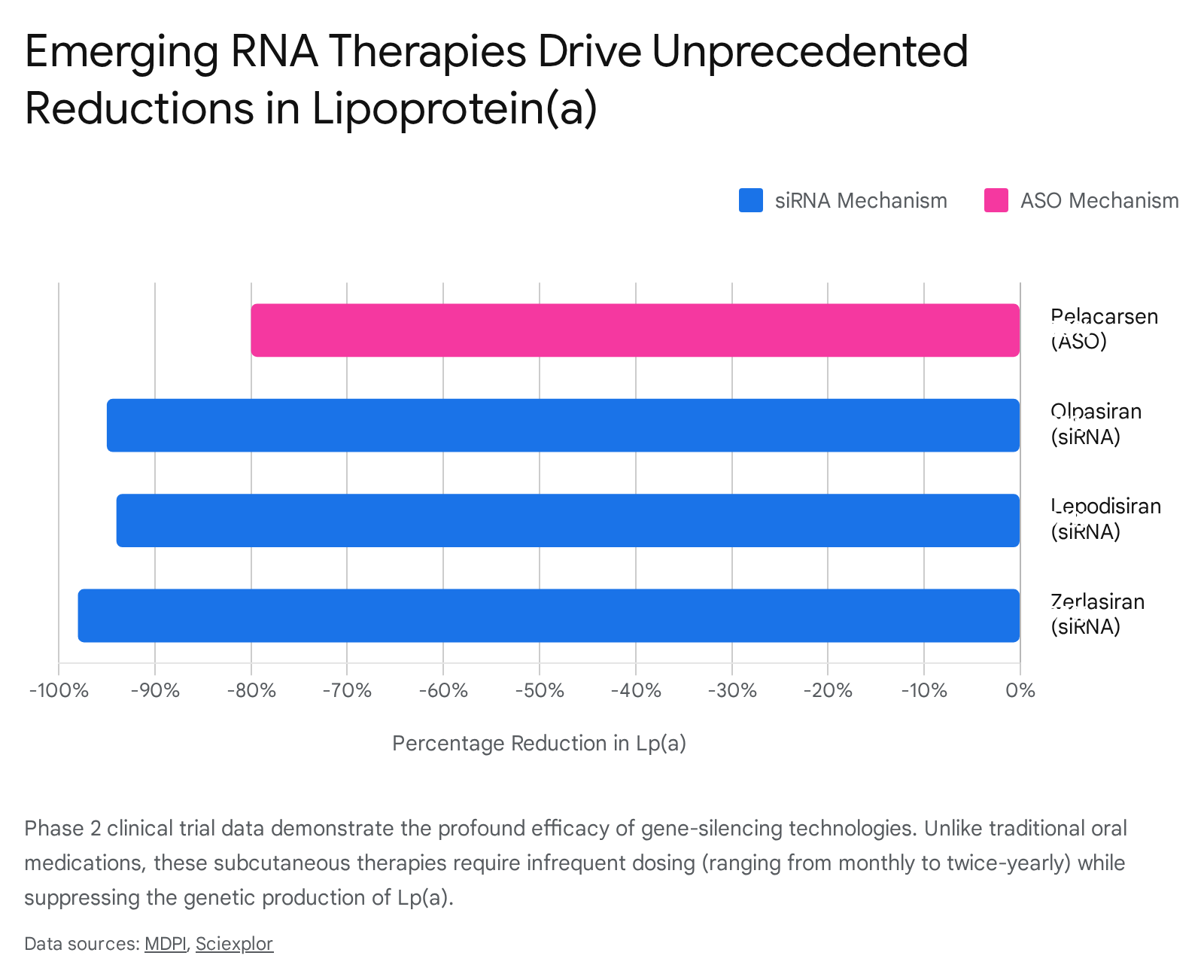
Until now, there have been no targeted pharmacological therapies approved to lower Lp(a) 16. Pelacarsen, developed by Novartis, is an investigational antisense oligonucleotide (ASO). Administered via a monthly subcutaneous injection, pelacarsen selectively binds to the apo(a) mRNA in the hepatocytes of the liver, preventing the synthesis of the protein and thereby silencing the production of the Lp(a) particle entirely 2116. In Phase 2 trials, pelacarsen safely reduced Lp(a) levels by approximately 80%, normalizing levels in an astonishing 98% of treated patients 1427. Furthermore, the recent Lp(a)FRONTIERS APHERESIS Phase 3 trial demonstrated that pelacarsen reduced the need for highly invasive lipoprotein apheresis by 72% in high-risk patients in Germany 16.
However, successfully lowering a biomarker does not automatically equate to preventing heart attacks. Thus, the Lp(a)HORIZON trial was initiated to provide definitive proof 14. This pivotal Phase 3 cardiovascular outcomes trial enrolled over 8,300 patients with established cardiovascular disease and elevated Lp(a) 14. It is an event-driven trial, designed to accrue 993 major adverse cardiac events before unblinding 27. Topline results are confirmed to be available in the first half of 2026, making a major presentation at the ESC Congress highly probable 2728. The trial is powered to detect a 15-20% relative risk reduction 27. If successful, it will incontrovertibly prove the "Lp(a) hypothesis" and unlock a massive new pillar of preventive cardiology.
The success of pelacarsen will also pave the way for a highly competitive class of small interfering RNA (siRNA) therapies, which utilize slightly different mechanisms to degrade apolipoprotein(a) mRNA. Drugs like olpasiran, lepodisiran, and zerlasiran are showing sustained Lp(a) reductions of over 90% with dosing intervals that stretch from every three months to twice a year, representing a staggering leap forward in patient convenience and therapeutic durability 2115.
The Heart Failure Paradigm: Finerenone and the MRA Renaissance
Heart failure is fundamentally categorized into two distinct types: Heart Failure with reduced Ejection Fraction (HFrEF, characterized by a weak pump) and Heart Failure with preserved Ejection Fraction (HFpEF, characterized by a stiff pump that cannot fill adequately) 29. For decades, HFpEF was a notorious graveyard for clinical trials; virtually no drug could prove a mortality benefit because the pathophysiology - driven by stiffening of the extracellular matrix, systemic inflammation, and profound metabolic dysfunction - was far more complex than simple pump failure 1429.
That grim reality changed recently with the advent of sodium-glucose cotransporter-2 (SGLT2) inhibitors. Now, a second robust pillar is emerging: non-steroidal mineralocorticoid receptor antagonists (nsMRAs).
At the previous ESC Congress, the FINEARTS-HF trial made international headlines by demonstrating that finerenone significantly reduced the composite risk of cardiovascular death and worsening heart failure events by 18% in patients with HFpEF/HFmrEF ($LVEF \geq 40\%$) 1718. Finerenone achieves this by selectively blocking the overactivation of the mineralocorticoid receptor, a key pathway that drives inflammation, fibrosis, and adverse remodeling in both the heart and kidneys 32. Unlike older, steroidal MRAs like spironolactone, finerenone boasts a far superior safety profile, carrying a much lower risk of causing severe hyperkalemia (dangerously high blood potassium) or side effects like gynecomastia 1920.
Moving into ESC 2026, the medical community anticipates highly consequential data from Bayer's broader "MOONRAKER" clinical trial program. The upcoming REDEFINE-HF trial is particularly crucial 1821. While FINEARTS-HF studied stable, ambulatory outpatients, REDEFINE-HF will report on the efficacy of initiating finerenone in 5,200 high-risk patients during hospitalization for an acute heart failure exacerbation, a highly vulnerable period for readmission 1821.
Additionally, the massive FINE-HEART participant-level meta-analysis, which pools data from nearly 19,000 patients across three pivotal trials (FIDELIO-DKD, FIGARO-DKD, and FINEARTS-HF), is expected to provide definitive, heavily powered answers on finerenone's ability to reduce all-cause mortality and preserve renal function across the entire spectrum of what is now recognized as Cardiovascular-Kidney-Metabolic (CKM) syndrome 223738. Other heart failure investigations, such as the VICTOR trial, will seek to expand the role of vericiguat - a soluble guanylate cyclase stimulator - into broader populations of chronic HFrEF patients, further expanding the pharmacological arsenal against the disease 2.
Cardio-Metabolic Synergy: The GLP-1/GIP Revolution
The convergence of obesity, diabetes, and cardiovascular disease has necessitated a conceptual shift away from isolated organ treatment toward systemic metabolic management. The multi-receptor incretin agonists have violently disrupted the cardiology landscape, rendering old treatment algorithms obsolete.
Tirzepatide, a dual GIP/GLP-1 receptor agonist famously known for its profound weight-loss capabilities, has been rigorously tested as a primary cardiovascular therapeutic. The Phase 3 SUMMIT trial evaluated tirzepatide in obese patients with HFpEF 1114. The results were staggering: over 52 weeks, tirzepatide reduced the composite risk of major cardiovascular complications (urgent heart failure visits, hospitalizations, or cardiovascular mortality) by 38% compared to placebo 11514.
Importantly, secondary and post-hoc analyses expected to mature by 2026 are proving that the cardiovascular benefits of incretin therapies extend far beyond mere weight loss or reductions in epicardial fat. Mechanistic data suggest that tirzepatide directly attenuates systemic inflammation (evidenced by a ~39% reduction in high-sensitivity C-reactive protein), improves endothelial function, lowers systolic blood pressure, and reduces myocardial wall stress 9523. As these drugs gain formal FDA and EMA approval for cardiovascular risk reduction, the focus at ESC 2026 will shift toward optimizing their use alongside existing therapies like SGLT2 inhibitors. Trialists will also debate the anticipated impacts of next-generation agents, such as retatrutide - a triple agonist showing up to 28% weight loss in Phase 2 - and the advent of highly accessible oral GLP-1 agents like orforglipron and oral semaglutide (Rybelsus) 11.
Advanced Interventions: Structural Heart and Hemodynamic Monitoring
While pharmacology dominates outpatient cardiology, interventional cardiology is witnessing parallel, awe-inspiring leaps. The RHEIA trial recently highlighted that Transcatheter Aortic Valve Implantation (TAVI) yielded superior one-year composite outcomes (reducing death, stroke, or rehospitalization to 8.9% versus 15.6%) compared to open-heart surgical aortic valve replacement (SAVR) exclusively in women - a historically underrepresented demographic in severe aortic stenosis trials 40.
Moving forward, newer iterations of minimally invasive treatments are dramatically altering risk profiles. The Pascal transcatheter valve repair system for leaky mitral valves is drastically reducing hospital recovery times from weeks to mere days, even for high-risk elderly patients with heavy comorbidity burdens 10. Similarly, the ENCIRCLE trial demonstrated striking success in Transcatheter Mitral Valve Replacement (TMVR) using the Edwards Sapien M3 device, achieving surgical-like results in inoperable patients 41.
Furthermore, device-based heart failure management is shifting into the home. Remote hemodynamic monitoring using implanted pulmonary artery sensors, such as the CardioMEMS device evaluated in the MONITOR-HF trial, allows clinicians to detect rising pressures and adjust diuretics weeks before a patient feels breathless 921. This integration of remote physiological data with AI-assisted screening represents a profound shift toward preventive, ambulatory heart failure management, extending the reach of specialists and reducing the strain on hospital infrastructure 9.
Challenging Old Dogmas: De-escalation and Residual Risk
The ESC Congress is not solely about introducing new therapies; it is equally focused on identifying when traditional treatments are no longer necessary. The recent REBOOT trial severely disrupted 40 years of medical dogma by demonstrating that routine beta-blockers offered no prognostic benefit to patients whose heart function remained normal after an uncomplicated heart attack 6. Similarly, upcoming trials like TARGET FIRST and DUAL-ACS will test the earlier withdrawal of aspirin or oral anticoagulants to reduce bleeding risks, simplifying regimens for patients who no longer require aggressive antiplatelet therapy 24.
Conversely, researchers are identifying hidden pockets of residual risk in patients thought to be well-treated. Post-hoc analyses of the landmark REDUCE-IT trial have shown that in statin-treated patients with controlled LDL cholesterol but elevated triglycerides, assessing risk-weighted apolipoprotein B (RW-apoB) is far superior at identifying residual cardiovascular risk than traditional lipid biomarkers 4344. Treating this residual risk with therapies like high-dose icosapent ethyl (a highly purified EPA fish oil derivative) has been shown to significantly reduce total hospitalizations and days lost to death or illness 2526.
Furthermore, therapies to lower LDL cholesterol are becoming more aggressive and less frequent. The VICTORION-Difference and VICTORION-Mono trials will present further data on inclisiran, a twice-yearly siRNA injection that slashes LDL cholesterol by silencing the PCSK9 gene, providing long-term durability that bypasses the adherence issues associated with daily statin pills 248.
What do these new treatments mean for patients?
For the everyday patient managing hypertension, high cholesterol, or heart failure, the rapid influx of new clinical data can induce whiplash. It is essential to apply calibrated uncertainty to separate treatments that are ready for the clinic today from those that require years of further research.
Ready for the Clinic Today
If you suffer from obesity-related heart failure with preserved ejection fraction (HFpEF), the landscape has officially shifted. GLP-1 and dual GLP-1/GIP agonists (like semaglutide and tirzepatide) are no longer categorized merely as "weight loss drugs"; they are evidence-based, guideline-directed cardiovascular therapeutics proven to keep patients out of the hospital, lower systemic inflammation, and significantly improve physical capacity 111423. Similarly, if you have chronic kidney disease or heart failure, non-steroidal MRAs like finerenone are available now to protect your kidneys and heart without the severe potassium-related side effects of older steroid-based drugs 1949.
Ready in 1 - 3 Years
If you are among the 20% of the population with highly elevated Lipoprotein(a), your era of waiting is nearly over. Assuming the Lp(a)HORIZON trial reports positive outcomes in 2026, therapies like pelacarsen or the bi-annually injected siRNA drugs (olpasiran, lepodisiran) could hit the global market shortly after, offering the first-ever pharmacological defense against this genetic risk factor 122128. For now, the most critical takeaway is to ask your primary care physician to test your Lp(a) levels at least once in your lifetime, as traditional, routine cholesterol panels do not measure it 1327. Additionally, novel hypertension treatments like zilebesiran - an RNAi therapeutic that controls blood pressure with a single injection every six months - are advancing rapidly through Phase 3 trials and could soon eliminate the need for daily blood pressure pills 2428.
Ready in 5 - 10 Years
CRISPR and in vivo gene editing to permanently cure high cholesterol or inherited cardiomyopathies remain firmly in the realm of clinical trials. While early Phase 1 data - such as using CRISPR to edit the ANGPTL3 gene - is miraculously promising and demonstrates profound lipid reductions 929, safety follow-ups over many years are absolutely required. Regulators must ensure that altering the human genome does not result in off-target mutations or long-term oncological risks before these "one-and-done" cures become widely accessible.
Bottom line
The upcoming ESC Congress 2026 signifies a monumental pivot in cardiovascular medicine, definitively shifting the paradigm from reactive crisis management to precision, disease-modifying prevention. We are transitioning away from daily, broad-spectrum pills toward highly targeted, infrequent genetic silencers and potent systemic metabolic modulators. Anticipated readouts from the Lp(a)HORIZON trial hold the potential to neutralize the last great unaddressed lipid risk factor, while finerenone and tirzepatide are successfully dismantling the historic complexities of heart failure with preserved ejection fraction. As global media translates these dense, highly technical clinical findings for the public, maintaining strict medical literacy - distinguishing between observational hype and randomized, hard-outcome proof - will be essential for integrating these breakthroughs safely, equitably, and effectively into patient care.