What to Watch in the 2026 Retatrutide Obesity Trials
Eli Lilly's investigational obesity drug retatrutide is preparing for two crucial Phase 3 data readouts in 2026: TRIUMPH-2 for patients with type 2 diabetes and TRIUMPH-3 for high-risk cardiovascular patients. These results will definitively show whether the drug's record-breaking 28 percent weight loss holds true in harder-to-treat populations and whether its unique triple-hormone mechanism is safe for those with established heart disease.
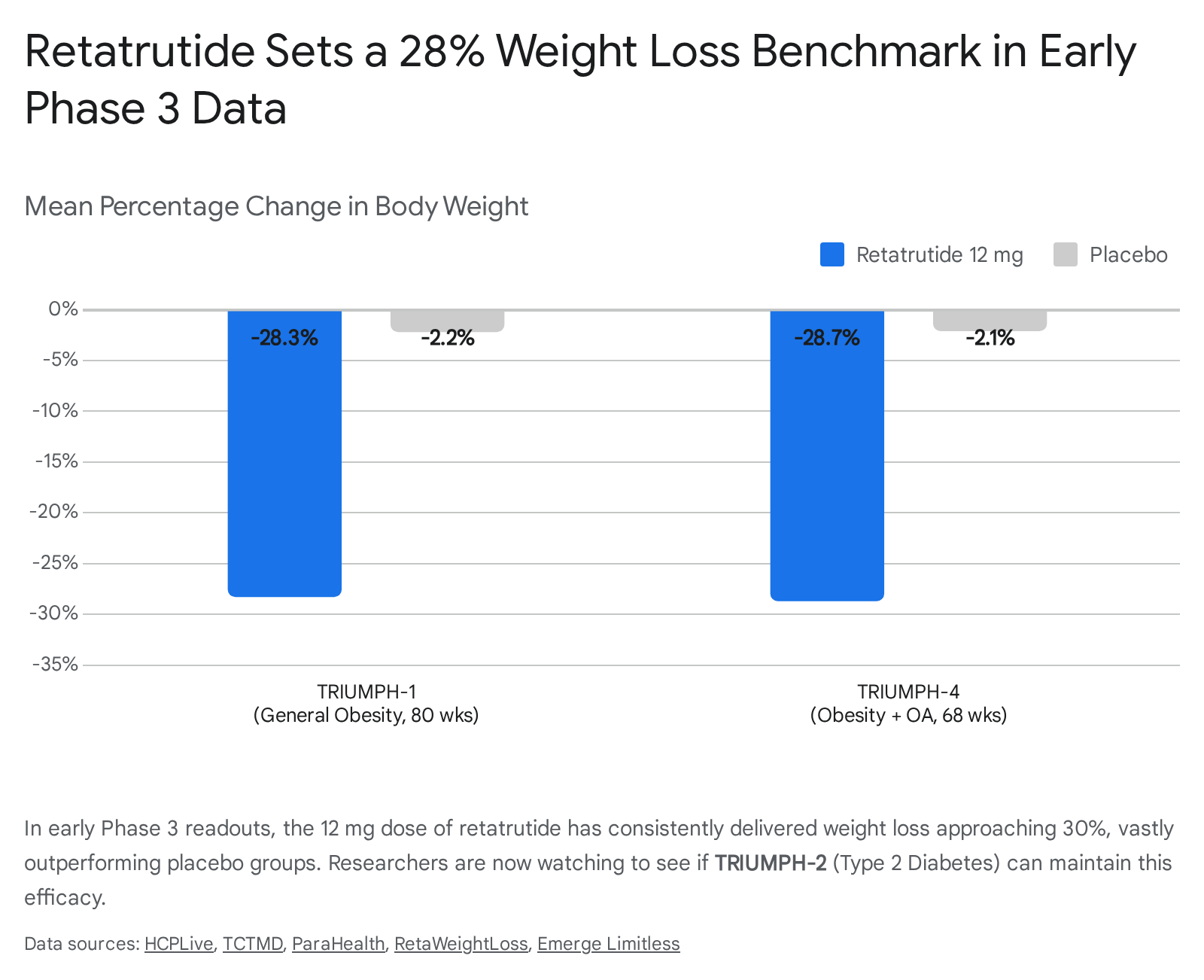
The commercial and clinical trajectory of obesity medicine was irrevocably altered in late 2025 and early 2026. Topline data from the TRIUMPH-4 (obesity with osteoarthritis) and TRIUMPH-1 (general obesity) trials revealed that retatrutide - often referred to as a "triple-G" agonist - could drive mean body weight reductions of 28.7% and 28.3%, respectively, at the highest 12 milligram doses 1234. These figures effectively shattered the efficacy ceiling previously established by dual-agonists like tirzepatide and mono-agonists like semaglutide.
However, general obesity is only one facet of the global metabolic crisis. To secure its position as the ultimate pharmacological tool for metabolic syndrome, retatrutide must prove its safety and efficacy in more medically complex patient populations. This is the primary objective of the ongoing TRIUMPH-2 and TRIUMPH-3 trials. With data expected to read out through the remainder of 2026, these two trials will clarify whether retatrutide can overcome the biological resistance to weight loss typically seen in diabetic patients, and whether its unique mechanism is safe for patients with a history of heart attacks and strokes.
The Mechanistic Advantage: Why Retatrutide Breaks Records
To understand the stakes of the upcoming 2026 readouts, it is essential to understand why retatrutide is achieving weight loss numbers historically reserved for surgical intervention 517.
First-generation incretin therapies, such as semaglutide (marketed as Wegovy and Ozempic), operate as single-receptor agonists. They target the glucagon-like peptide-1 (GLP-1) receptor, which slows gastric emptying and signals satiety to the brain, effectively reducing caloric intake 2. The next evolution in this therapeutic class was tirzepatide (marketed as Zepbound and Mounjaro), a dual-agonist that adds glucose-dependent insulinotropic polypeptide (GIP) receptor activation. GIP improves insulin sensitivity, modulates lipid metabolism, and appears to buffer some of the gastrointestinal side effects inherent to GLP-1 activation, allowing patients to tolerate higher, more effective doses 248.
Retatrutide takes the architectural foundation of tirzepatide and adds a third mechanism: glucagon receptor agonism 2910. Historically, elevating glucagon was considered counterproductive in metabolic disease because it naturally stimulates the liver to release stored glucose into the bloodstream. However, researchers discovered that when combined with the potent insulin-stimulating and appetite-suppressing effects of GLP-1 and GIP, the glucagon component acts as a massive accelerator for energy expenditure.
By combining GLP-1 for appetite suppression, GIP for improved insulin sensitivity, and glucagon for increased resting energy expenditure and liver fat clearance, retatrutide forces the body to burn stored fat while significantly reducing caloric intake 2411. Furthermore, glucagon receptor activation drives rapid clearance of hepatic fat, directly addressing liver-related metabolic dysfunctions like steatohepatitis 21112. This triad essentially attacks obesity from two sides simultaneously: drastically lowering calories coming in while increasing the calories being burned at rest.
This unique mechanism is exactly why TRIUMPH-2 and TRIUMPH-3 are being monitored so closely by endocrinologists and cardiologists worldwide. The addition of glucagon fundamentally changes how the drug interacts with blood sugar and cardiovascular tissue, meaning assumptions based on older GLP-1 drugs cannot simply be copy-pasted onto retatrutide.
Establishing the Bariatric Benchmark
Before projecting the outcomes of TRIUMPH-2 and 3, it is vital to contextualize the momentum Eli Lilly brings into 2026. The initial Phase 3 readouts from the TRIUMPH program have established a new high-water mark for pharmacological weight management.
In late 2025, the TRIUMPH-4 trial evaluated retatrutide in patients living with obesity and knee osteoarthritis. The 12 milligram dose produced an astounding 28.7% mean body weight reduction at 68 weeks, dwarfing the 2.1% reduction seen in the placebo group 2342. This was closely followed by the TRIUMPH-1 trial in May 2026, which studied over 2,300 adults with general obesity. In that trial, the 12 milligram dose resulted in a 28.3% weight reduction at 80 weeks 1514.
Even more remarkable was the long-term durability data. For patients who continued the drug in an extension phase up to 104 weeks, the average weight loss deepened to 30.3%, or roughly 85 pounds 5115. These metrics are highly consequential because 30% weight loss is the traditional threshold where pharmacological intervention meets the historical effectiveness of bariatric surgery. The question for the remaining 2026 readouts is whether this benchmark can be maintained across diverse, sicker populations.
The TRIUMPH Program Structure
To comprehend the full scope of what Eli Lilly is attempting in 2026, it helps to view the Phase 3 TRIUMPH program holistically. Rather than pursuing a sequential approval path where one indication is proven before moving to the next, Eli Lilly initiated multiple massive trials in parallel across varying clinical settings 101617. This parallel strategy accelerates the timeline to market but commits an immense amount of capital and resources upfront.
| Trial Name | Clinical Population Focus | Approximate Size | Duration | Current Status |
|---|---|---|---|---|
| TRIUMPH-1 | Obesity / Overweight without diabetes | ~2,339 | 80 weeks | Completed (May 2026 Readout) 1514 |
| TRIUMPH-2 | Obesity + Type 2 Diabetes | ~1,000 | 89 weeks | Expected Mid/Late 2026 33 |
| TRIUMPH-3 | Severe Obesity + Cardiovascular Disease | ~1,946 | 113 weeks | Expected Late 2026 456 |
| TRIUMPH-4 | Obesity + Knee Osteoarthritis | ~445 | 68 weeks | Completed (Dec 2025 Readout) 234 |
| TRIUMPH-Outcomes | Obesity + CVD or Chronic Kidney Disease | ~10,000 | ~5 years | Enrolling (Expected 2029) 723 |
As outlined above, TRIUMPH-1 and TRIUMPH-4 have already delivered their primary endpoints. The pharmaceutical industry's attention is now entirely locked onto the imminent results from TRIUMPH-2 and TRIUMPH-3.
TRIUMPH-2: Can Retatrutide Break the Diabetic Weight Loss Plateau?
Expected to read out in mid-to-late 2026, the TRIUMPH-2 trial (NCT05929079) is evaluating retatrutide in approximately 1,000 adults who suffer from both obesity and type 2 diabetes 83. The randomized, double-blind, placebo-controlled trial spans 89 weeks, making it one of the longest evaluation periods for metabolic control in the program 3.
The primary endpoint of TRIUMPH-2 mirrors the rest of the program: the percentage change in body weight from baseline to the end of the trial 17. However, the secondary endpoints are where the true clinical nuance lies. Investigators will be closely tracking the proportion of participants achieving categorical weight loss milestones (such as 10%, 15%, and 20% reduction), alongside changes in HbA1c, fasting plasma glucose, and the frequency of hypoglycemic events 1617.
The Challenge of Diabetic Weight Loss
In the realm of incretin-based weight management, patients with type 2 diabetes present a notorious clinical challenge. Across almost all major clinical trials for semaglutide and tirzepatide, patients with diabetes consistently lose significantly less weight than matched patients without diabetes. This biological resistance is well-documented in the literature, though the exact physiological mechanisms remain a subject of intense academic debate.
It is widely theorized that prolonged hyperinsulinemia - the chronic overproduction of insulin common in early-to-mid stage type 2 diabetes - promotes fat storage and alters metabolic setpoints. Additionally, the concomitant use of other diabetes medications, particularly insulin or sulfonylureas, inherently promotes weight gain, directly counteracting the effects of the weight-loss drugs 2316.
The central clinical question for TRIUMPH-2 is whether retatrutide's unique addition of glucagon receptor agonism can break through this diabetic resistance. Glucagon is the counter-regulatory hormone to insulin; it mobilizes stored energy. By simultaneously boosting insulin sensitivity via GIP and increasing energy expenditure via glucagon, retatrutide theoretically provides a more complete metabolic reset.
Early indicators are incredibly promising. In Phase 2 dose-finding studies, retatrutide demonstrated an impressive ~16.9% weight reduction at 36 weeks in patients with type 2 diabetes, alongside an average HbA1c reduction of over 2.0% 8825. If the 89-week TRIUMPH-2 trial can deliver weight loss exceeding 20% to 22% in a diabetic population, it will completely reset the standard of care for "diabesity," proving that the biological resistance of diabetes can be pharmacologically overridden.
The Nested Sleep Apnea Basket Trial
An innovative feature of Eli Lilly's TRIUMPH program is its use of "basket" or "nested" trial designs 109. Rather than running entirely separate, multi-year trials for common obesity comorbidities like joint pain or respiratory issues, the TRIUMPH master protocols include nested sub-studies. TRIUMPH-2 contains a nested protocol specifically evaluating a subset of participants who suffer from moderate-to-severe obstructive sleep apnea (OSA) 103.
Within this OSA sub-cohort, investigators will measure the change in the Apnea-Hypopnea Index (AHI) - the number of breathing pauses or shallow breaths per hour of sleep - from baseline to week 52 10169. Sleep apnea is largely a mechanical disorder exacerbated by excess adipose tissue in the neck and upper airway, which collapses during sleep. Weight loss is currently the most effective non-mechanical treatment for OSA. Because retatrutide has shown a profound ability to reduce overall body fat, including visceral and neck adiposity, experts anticipate dramatic reductions in the AHI score, potentially allowing patients to discontinue continuous positive airway pressure (CPAP) therapy 272810.
Securing a positive readout in this nested OSA trial is crucial for Lilly's commercial strategy. Payer coverage for anti-obesity medications remains a significant hurdle globally. By proving that retatrutide directly resolves a severe, costly medical condition like sleep apnea, Lilly can position the drug as a medically necessary intervention rather than a cosmetic lifestyle treatment, thereby forcing the hand of health insurers and national health systems.
TRIUMPH-3: Cardiovascular Safety and High-Risk Obesity
While TRIUMPH-2 focuses on overriding metabolic resistance, TRIUMPH-3 (NCT05882045) shifts the focus strictly to cardiovascular safety and efficacy in the highest-risk patient populations. Slated to conclude in late 2026, this 113-week trial enrolled roughly 1,946 participants 456.
To qualify for TRIUMPH-3, participants had to have severe obesity (defined as a BMI of 35 or higher) and, crucially, established cardiovascular disease. This means every patient in this trial has a documented history of a myocardial infarction (heart attack), an ischemic or hemorrhagic stroke, or symptomatic peripheral arterial disease 4530.
Clarifying the Cardiovascular Trials
It is vital for researchers and investors to distinguish TRIUMPH-3 from the similarly named TRIUMPH-Outcomes trial (NCT06383390), as they serve entirely different regulatory functions: * TRIUMPH-3 is a 113-week weight management and general safety trial. The primary endpoint remains the percentage change in body weight, with a heavy emphasis on cardiovascular risk markers 45. * TRIUMPH-Outcomes is a massive, 5-year, 10,000-patient cardiovascular outcome trial (CVOT). Its primary goal is not weight loss, but to determine if retatrutide actually reduces the incidence of Major Adverse Cardiovascular Events (MACE) - such as cardiovascular death or non-fatal myocardial infarction - and prevents the worsening of chronic kidney disease. TRIUMPH-Outcomes will not finish until 2029 72331.
Why Heart Rate is the Primary Concern
Because the definitive CVOT data from TRIUMPH-Outcomes is years away, regulatory agencies and the broader medical community will rely heavily on the 2026 TRIUMPH-3 readout to gauge the drug's near-term cardiovascular safety profile.
The unique triple-agonist mechanism of retatrutide demands this heightened scrutiny. Glucagon receptor activation is known to increase resting energy expenditure, but it has a well-documented side effect of elevating resting heart rate. In Phase 2 trials, retatrutide was associated with a modest but noticeable heart rate increase of 5 to 7 beats per minute at the 12 milligram dose 3132.
While a healthy adult easily tolerates a 7 bpm increase in resting heart rate, cardiologists require definitive proof that this chronic elevation does not pose a risk to ischemic heart tissue. An elevated heart rate increases myocardial oxygen demand, which could theoretically trigger arrhythmias, angina, or exacerbate heart failure in patients whose cardiovascular systems are already compromised.
The TRIUMPH-3 results will clarify this balance of risk and reward. If the trial demonstrates that high-risk cardiovascular patients can safely achieve 25% or greater weight loss without a corresponding increase in adverse cardiac events, it will clear a massive psychological and regulatory hurdle. Furthermore, researchers will be looking closely at secondary cardiometabolic endpoints, including reductions in systolic blood pressure, systemic inflammation (hsCRP), waist circumference, and highly atherogenic lipids (LDL cholesterol), all of which are expected to improve dramatically due to the drug's profound weight-loss effects 211416.
Navigating the Safety Profile: Dysesthesia and Tolerability
With efficacy essentially proven to be best-in-class in the general obesity population, regulatory bodies and prescribing physicians are turning a critical eye toward the safety and tolerability data emerging from the TRIUMPH program. The most potent drug in the world is useless if patients cannot tolerate its side effects.
The Dysesthesia Safety Signal
The most closely watched safety metric in the upcoming 2026 readouts involves a unique neurological side effect known as dysesthesia. Dysesthesia translates to an abnormal, distorted, and often unpleasant sense of touch. Patients frequently describe it as acute skin sensitivity, a burning sensation, tingling, or "pins and needles" in the extremities, occurring entirely without an external physical stimulus 3334.
This side effect first garnered widespread clinical attention following the TRIUMPH-4 readout in late 2025, where it was reported in 20.9% of patients taking the 12 milligram dose, compared to just 0.7% of the placebo group 333. In the subsequent TRIUMPH-1 readout in May 2026, the rate of dysesthesia improved somewhat, affecting 12.5% of patients on the 12 milligram dose 514.
Eli Lilly has consistently maintained that these dysesthesia events are generally mild to moderate in severity, typically transient, and rarely lead to patients discontinuing the medication 2143335. However, the TRIUMPH-2 trial will serve as the ultimate stress test for this specific side effect. Patients with long-standing type 2 diabetes frequently suffer from diabetic peripheral neuropathy - nerve damage in the hands and feet caused by chronically high blood sugar.
A critical challenge for researchers reviewing the TRIUMPH-2 data will be determining exactly how retatrutide-induced dysesthesia interacts with pre-existing diabetic neuropathy. If the drug significantly exacerbates nerve pain or causes profound discomfort in diabetic patients, it could limit its utilization in that specific demographic, forcing physicians to rely on older dual- or mono-agonists for those particular patients.
Gastrointestinal Tolerability and Discontinuation Rates
Beyond the novel dysesthesia signal, retatrutide displays a side effect profile highly consistent with the broader incretin class. Because the drug fundamentally alters gastric emptying rates and central satiety signaling, gastrointestinal adverse events are by far the most common side effects reported 3236.
Across the completed Phase 3 trials, researchers observed high rates of nausea (up to 42.4%), diarrhea (up to 34%), and vomiting (up to 25.3%) at the highest 12 milligram doses 32141533. Crucially, these side effects are intimately tied to the dose-escalation phase. Patients in the TRIUMPH program are initiated at a low 2 milligram weekly injection and slowly titrated upward over several months to allow the body to acclimate to the hormonal changes.
In terms of overall tolerability, the discontinuation rates due to adverse events provide the clearest picture of the patient experience. In TRIUMPH-1, 11.3% of patients in the 12 milligram arm stopped taking the drug due to side effects, compared to 4.9% in the placebo group 5211. While an 11% dropout rate is slightly higher than the 5 - 8% rates typically observed in semaglutide trials, market analysts and clinicians generally view it as a highly acceptable trade-off given that the drug provides weight loss equivalent to bariatric surgery 535.
Regulatory Timelines: The Path to Market Approval
The avalanche of clinical data arriving throughout 2026 is setting the stage for a massive, coordinated regulatory push by Eli Lilly. However, despite the intense public interest and the unprecedented Phase 3 data already published, as of mid-2026, retatrutide remains strictly an investigational molecule. It has not yet been submitted to the U.S. Food and Drug Administration (FDA) or the European Medicines Agency (EMA) for commercial approval 38.
Based on Lilly's public guidance, the structure of the TRIUMPH program, and the historical cadence of pharmaceutical approvals, the regulatory timeline is becoming highly predictable:
- Data Aggregation and Presentation (Mid 2026): Eli Lilly is utilizing major medical conferences, such as the American Diabetes Association (ADA) Scientific Sessions in June 2026, to present detailed subgroup analyses of TRIUMPH-1 and early diabetes data 112512. Behind the scenes, the company will spend the summer of 2026 compiling the massive datasets from TRIUMPH-1, 2, and 3 into a comprehensive safety and efficacy dossier.
- NDA Submission (Late 2026): Eli Lilly is heavily projected to file its formal New Drug Application (NDA) with the FDA in the fourth quarter of 2026 3840. This submission will bundle the obesity, osteoarthritis, and likely the type 2 diabetes data into a single, massive regulatory filing.
- FDA Review and Potential Approval (Late 2027 to Early 2028): Once the NDA is submitted, the FDA operates on a standard 10-month review clock under the Prescription Drug User Fee Act (PDUFA). Assuming no major safety signals delay the process, FDA approval and subsequent commercial launch in the United States is highly likely in late 2027 or the first quarter of 2028 3840.
- European and Global Approvals (2028 - 2029): The EMA and the UK's Medicines and Healthcare products Regulatory Agency (MHRA) generally operate on a slightly delayed timeline compared to the FDA. The requirement for centralized marketing authorization in Europe, followed by complex, country-by-country reimbursement negotiations (and NICE appraisals in the UK), will likely push widespread European availability into late 2028 and 2029 404113.
The Broader Market Context in 2026
While retatrutide aims to secure the absolute top tier of efficacy, the market it enters in 2028 will look vastly different than the market of today. Beyond injectable treatments, pharmaceutical companies are rapidly advancing oral GLP-1 therapies designed for convenience. Eli Lilly's own oral GLP-1 candidate, orforglipron, has shown weight loss of up to 15% in trials and operates without the strict food and water restrictions that encumber current oral options like Rybelsus 251444.
The introduction of highly effective daily pills will likely bifurcate the obesity market. Oral medications like orforglipron may become the first-line treatment for moderate overweight and maintenance phases, while incredibly potent injectables like retatrutide will be reserved for severe clinical obesity, diabesity, and patients requiring rapid, substantial weight reduction to prevent imminent cardiovascular events or joint replacements 1115.
The Gray Market and "Research-Grade" Risks
The massive hype surrounding retatrutide's 28% weight loss figures has generated a dangerous secondary market. Throughout 2026, social media platforms and unregulated telehealth sites have seen an explosion of vendors selling "research-grade" or compounded retatrutide directly to consumers 446.
Because the drug is not yet approved by any global regulatory body, and its long-term safety profile is still actively being audited through trials like TRIUMPH-Outcomes, these products are entirely unregulated. The FDA has issued stringent warnings regarding the illegal sale of unapproved incretin drugs, explicitly noting that any retatrutide acquired outside of a strictly registered, institutional clinical trial lacks fundamental sterility, identity, and potency verification 446. Using these unregulated gray-market peptides carries immense risk, particularly concerning the untested dysesthesia and heart rate side effects.
Bottom line
The upcoming TRIUMPH-2 and TRIUMPH-3 readouts in 2026 are poised to answer the final, most critical questions surrounding retatrutide before it faces regulatory review. TRIUMPH-2 will determine if the drug's triple-agonist mechanism can successfully break the stubborn biological resistance to weight loss seen in type 2 diabetes. Concurrently, TRIUMPH-3 will define its safety profile - particularly concerning heart rate elevation - in patients with established, high-risk cardiovascular disease. While unprecedented efficacy nearing 30% weight loss has already been confirmed in general obesity, the medical community will be watching closely to see if the unique neurological side effect of dysesthesia poses a meaningful barrier to long-term adherence, especially in diabetic populations with pre-existing neuropathy.