What Is Lipoprotein(a) and Why Cardiologists Focus on It
Lipoprotein(a) is a highly inflammatory, genetically inherited cholesterol particle that affects roughly one in five people globally and significantly increases the risk of heart attacks, strokes, and heart valve failure. Cardiologists are intensely focused on the particle in 2026 because updated clinical guidelines now mandate universal screening for it, and the first major clinical trials for revolutionary drugs designed to drastically lower its levels are finally publishing their results.
The invisible threat in the bloodstream
For decades, the standard approach to preventing cardiovascular disease has focused on a familiar checklist: a healthy diet, regular physical exercise, maintaining a healthy weight, controlling blood pressure, and keeping low-density lipoprotein (LDL) cholesterol - the traditional "bad" cholesterol - at a low level. While this model has saved millions of lives, it leaves a dangerous and highly prevalent blind spot.
Consider the common clinical scenario of an individual who eats a pristine diet, exercises daily, and maintains a perfectly normal standard lipid panel, yet still suffers a devastating heart attack in their forties or fifties. For years, these cases puzzled primary care physicians and frustrated patients who felt they had done everything right. Today, cardiovascular specialists recognize that the culprit in a massive percentage of these otherwise unexplained cardiovascular events is a stealthy particle known as lipoprotein(a), pronounced "lipoprotein little a" or simply Lp(a) 123.
High-profile cases have brought this into the public eye. For instance, when celebrity fitness trainer Bob Harper suffered a severe heart attack in 2017 despite his famously healthy lifestyle, genetic testing eventually revealed extremely high levels of Lp(a) 4. Similarly, patient advocates like Sandra Revill Tremulis, who almost died from a 95% coronary blockage at age 39 despite normal cholesterol levels, discovered Lp(a) was the underlying cause. Tremulis went on to establish a foundation that successfully lobbied the Centers for Disease Control and Prevention (CDC) to recognize high Lp(a) as a distinct clinical diagnosis in 2018 5.
Despite being discovered in the 1960s, Lp(a) remained on the fringes of routine medical practice for decades. That era has abruptly ended. In 2026, Lp(a) is the most closely watched biomarker in cardiovascular medicine. The global medical community has realized that it is impossible to accurately assess a patient's lifelong risk of heart disease without knowing their Lp(a) status, and the pharmaceutical industry is locked in a multibillion-dollar race to bring the first dedicated Lp(a)-lowering therapies to the market 6769.
The unique biology of lipoprotein(a)
To understand why Lp(a) is so damaging, one must examine its molecular structure. Lipoproteins are essentially the microscopic "ships" that transport lipids (fats) and cholesterol through the water-based environment of the bloodstream 34.
At its core, Lp(a) is very similar to a standard LDL cholesterol particle. It contains a lipid core wrapped in a structural protein called apolipoprotein B-100 (apoB-100), which is the hallmark of all atherogenic (plaque-causing) particles 357. However, what distinguishes Lp(a) from standard LDL is the addition of a second, unique protein called apolipoprotein(a), or apo(a). This extra protein is tightly bound to the apoB-100 moiety by a single covalent disulfide bond 57.
This addition fundamentally alters how the particle behaves in the human body. Medical professionals often use a "Velcro" analogy to describe the effect: the apo(a) protein makes the particle exceptionally sticky, allowing it to easily bind to the endothelial cells lining the walls of blood vessels 38.
The apo(a) protein itself is a fascinating evolutionary anomaly. It is found in only a few species, primarily humans and non-human primates 4. The protein contains tri-looped structural domains called "kringles." Specifically, differences in the number of identically repeated copies of the kringle IV domain give rise to significant size variations (isoform size heterogeneity) in the apo(a) protein from person to person 7. Paradoxically, individuals who inherit a genetic variant resulting in a smaller apo(a) isoform actually produce a higher concentration of Lp(a) particles in their blood, leading to greater cardiovascular risk 12.
A triple threat to cardiovascular health
Once trapped in the arterial wall, Lp(a) triggers a cascade of damage through three distinct mechanisms, making it significantly more dangerous than standard LDL cholesterol on an equimolar basis 29.
- Atherogenesis (Plaque Formation): Just like standard LDL, Lp(a) deposits cholesterol directly into the artery walls, accelerating the buildup of atherosclerotic plaque. This narrows the arteries and restricts blood flow over time 2312.
- Inflammation: Lp(a) serves as the primary molecular carrier for oxidized phospholipids in the bloodstream. These oxidized lipids are highly toxic and pro-inflammatory. They continuously irritate the blood vessel walls, causing existing plaques to become inflamed, unstable, and much more likely to rupture 210.
- Thrombosis (Clotting): The unique apo(a) protein shares a striking structural similarity to plasminogen, a natural enzyme the human body uses to dissolve blood clots. Because of this structural mimicry, Lp(a) acts as a competitive inhibitor. It interferes with the body's natural clot-busting machinery, making abnormal, life-threatening blood clots more likely to form and persist 27129.
Beyond the arteries, Lp(a) is deeply linked to the heart's mechanical structures. Long-term epidemiological and genomic data have revealed a powerful connection between high Lp(a) levels and calcific aortic valve disease (CAVS) 59. A major breakthrough in 2013 utilized Genome-Wide Association Study (GWAS) data to prove that the LPA gene (which encodes the apo(a) protein) is the only single gene significantly associated with the presence of CAVS 7. For patients developing aortic stenosis, the heart's main valve progressively thickens and calcifies. Currently, there is no medical treatment to stop its progression; the only solution for end-stage disease is open-heart surgery or mechanical valve replacement 715.
Epidemiology and genetic determinism
Lp(a) elevation is remarkably common. An estimated 1 in 5 people worldwide - approximately 20% of the global population, or over one billion adults - have elevated levels of Lp(a) 47812. Because the condition almost never causes physical symptoms until a catastrophic event like a stroke or heart attack occurs, the vast majority of these individuals live entirely unaware of their heightened risk 816.
Unlike many cardiovascular risk factors that develop over time due to lifestyle choices, a person's Lp(a) concentration is established at birth. The LPA gene accounts for roughly 90% of the variation in Lp(a) levels between individuals, making it one of the most highly heritable cardiovascular risk factors in modern medicine 12. Because the level is genetically hardwired, it remains relatively constant throughout an individual's adult life 1.
There are, however, minor fluctuations based on hormonal changes. Research indicates that Lp(a) levels often rise in women as they transition through menopause. Studies suggest that estrogen naturally suppresses the production of Lp(a); therefore, as estrogen levels steeply decline around the age of 50, female patients often see a corresponding bump in their Lp(a) concentrations 4. Furthermore, data from the Kangbuk Samsung Health Study and other demographic analyses suggest that certain populations, including South Asian and Black demographics, may carry higher baseline medians and potentially face greater relative risks at equivalent Lp(a) concentrations 911.
Debunking the myths: Why standard interventions fail
For patients newly diagnosed with high Lp(a), the standard medical advice of the past several decades - to eat better, exercise more, and take a statin - has been a source of immense frustration and confusion. Understanding why these traditional methods fail is critical for modern cardiovascular management 2.
The lifestyle limitation
Nutrition and physical activity are foundational for overall metabolic health, but Lp(a) is uniquely resistant to lifestyle modifications. Because the liver manufactures Lp(a) at a constant rate dictated by cellular DNA, dietary interventions result in little to no meaningful reduction 212. Low-fat diets, Mediterranean diets, extreme caloric restriction, and even intense aerobic or resistance training generally fail to lower the absolute concentration of the particle 112. Weight loss, which can dramatically improve insulin sensitivity and lower triglycerides, leaves Lp(a) completely unchanged 312.
A minor exception exists in highly specific dietary contexts: diets excessively rich in trans-unsaturated fatty acids have been shown to increase Lp(a), while some studies suggest that a relatively high intake of saturated fatty acids might slightly lower it. However, adopting a high-saturated-fat diet to lower Lp(a) is counterproductive, as it massively increases standard LDL cholesterol and overall cardiovascular risk 12. Similarly, supplements like coenzyme Q10, L-Carnitine, and flaxseed exert only a mild, clinically insignificant lowering effect on plasma Lp(a) 12.
While lifestyle changes cannot disarm the genetic trigger of Lp(a), they remain essential. Exercise and a healthy diet improve the overall biological terrain - lowering systemic inflammation, improving blood pressure, and widening the functional capacity of the blood vessels - which helps build a stronger defense against the damage Lp(a) attempts to cause 23.
The statin paradox
Statins, such as atorvastatin and rosuvastatin, are highly effective medications for lowering standard LDL cholesterol. They operate by blocking an enzyme involved in cholesterol synthesis in the liver. However, they were never designed to treat Lp(a) 2. Statins do not meaningfully affect the production of the apo(a) protein 2.
In a frustrating paradox for patients, robust clinical data shows that statins can actually increase Lp(a) levels by 10% to 20% in certain individuals 1212. This occurs because statins upregulate the production of certain receptors in the liver, which indirectly alters lipoprotein dynamics. While statins remain absolutely critical for patients with high Lp(a) to control their concurrent LDL risk, utilizing a statin with the primary goal of lowering Lp(a) is ineffective and provides a false sense of security 12.
Current limited pharmacological options
Before the anticipated breakthrough drugs of 2026, physicians have had very few tools to directly target the particle.
- PCSK9 Inhibitors: Injectable monoclonal antibodies like evolocumab (Repatha) and alirocumab (Praluent) are highly effective at lowering LDL. As a secondary benefit, they also lower Lp(a) by approximately 20% to 30% 31213. While not a complete solution, post-hoc analyses from trials like ODYSSEY OUTCOMES showed that alirocumab reduced major adverse cardiovascular events (MACE) to a greater degree in patients who had high baseline Lp(a) levels 913.
- Lipoprotein Apheresis: For extreme, treatment-resistant cases - such as patients with familial hypercholesterolemia, established coronary disease, and extremely high Lp(a) - patients can undergo apheresis 1514. This is a dialysis-like procedure performed every one to two weeks that physically filters atherogenic lipoproteins out of the blood, reducing levels acutely by 70% to 80%, though levels rebound between sessions 15.
- Niacin: High-dose niacin can lower Lp(a) by 20% to 25%. However, it has largely fallen out of favor in modern cardiology due to a lack of proven cardiovascular outcome benefits in modern trials, combined with significant side effects like severe flushing and impaired glucose tolerance 12.
- Ezetimibe: This cholesterol-absorption inhibitor produces only modest Lp(a) reductions of around 7%, which is too small relative to the magnitude of risk conferred by elevated levels 12.
Structural Comparison: LDL vs. Lp(a)
The table below summarizes the critical distinctions between standard LDL and Lp(a) that dictate modern treatment strategies.
| Feature | Low-Density Lipoprotein (LDL) | Lipoprotein(a) |
|---|---|---|
| Primary Structural Driver | Apolipoprotein B-100 | Apolipoprotein B-100 + Apolipoprotein(a) 57 |
| Determinant of Levels | Diet, lifestyle, and polygenic factors | 80 - 90% monogenic (LPA gene) 312 |
| Response to Lifestyle Changes | High (diet and exercise reduce levels) | Minimal to none 11212 |
| Response to Statin Therapy | Excellent (drastic reductions) | None (may slightly increase levels) 1212 |
| Pro-thrombotic (Clotting) Risk | No direct mechanism | Yes (via plasminogen mimicry) 7129 |
| Standard Lipid Panel Inclusion | Yes (always checked routinely) | No (requires a specific, separate assay) 412 |
| Recommended Testing Frequency | Annually or as directed by a physician | Once in a lifetime (levels remain stable) 11315 |
The 2026 ACC/AHA Dyslipidemia Guidelines: A paradigm shift
In March 2026, the American College of Cardiology (ACC), the American Heart Association (AHA), and nine other leading medical societies released a massive, unified update to the clinical guidelines for managing blood cholesterol and dyslipidemia 1522. This comprehensive document officially retired the older 2018 guidelines and instituted a major paradigm shift toward earlier, more aggressive, and highly personalized cardiovascular intervention 152216.
The 2026 guidelines brought Lp(a) out of the shadows of specialized lipid clinics and squarely into mainstream primary care.
Universal screening is now the standard
The most consequential update regarding Lp(a) is a "Class 1" recommendation - the strongest level of clinical endorsement - that every adult should have their Lp(a) measured at least once in their lifetime as part of a comprehensive atherosclerotic cardiovascular disease (ASCVD) risk assessment 14222425.
Because Lp(a) levels remain stable throughout a person's adult life, repeat testing to monitor the number is generally completely unnecessary, avoiding excess healthcare costs 11517. A single blood test can accurately map a patient's lifelong genetic risk trajectory 115. If a patient is found to have high Lp(a), the guidelines strongly urge "cascade screening" - testing their first-degree relatives, such as siblings and children, to uncover hidden inherited risk across the family tree before a cardiovascular event occurs 132718.
Defining risk thresholds
Lp(a) is typically measured in either milligrams per deciliter (mg/dL), which indicates particle mass, or nanomoles per liter (nmol/L), which indicates the actual particle count. The 2026 guidelines established clear, actionable thresholds for clinical risk stratification 1425:
- Low Risk: Less than 30 mg/dL (or <75 nmol/L). This represents the normal population baseline 1325.
- Intermediate Risk: 30 to 50 mg/dL (75 to 125 nmol/L). Clinicians are advised to monitor these patients more closely and optimize traditional risk factors 1325.
- High Risk: 50 mg/dL (125 nmol/L) or higher. At this threshold, which affects 20% of the population, a patient's relative risk of a cardiovascular event is roughly 40% higher than the baseline population 141527.
- Very High Risk: Above 100 mg/dL (250 nmol/L). At these extremes, the risk of heart attack or stroke is doubled, and climbs up to a four-fold increase at the highest percentiles, posing a severe threat equivalent to heterozygous familial hypercholesterolemia (HeFH) 1415.
Moving from 10-year to 30-year risk assessment
The 2026 AHA/ACC guidelines also retired the outdated "Pooled Cohort Equations," a risk calculator that had been in use since 2013 222418. The older tool was known to overestimate the 10-year risk of a heart attack and stroke by 40% to 50% in certain populations and failed to account for long-term exposure 1524.
It was replaced with the PREVENT-ASCVD risk calculator. PREVENT removes race as a biological variable, incorporates vital metrics like kidney health and blood sugar control, and generates both a 10-year and a 30-year risk estimate 2224. This shift is crucial for patients with high Lp(a). Recognizing that cardiovascular disease is a cumulative process, knowing a 30-year-old patient has had elevated atherogenic particles since childhood allows clinicians to intervene decades before irreversible arterial damage accumulates 2224.
Global perspectives: AHA/ACC 2026 vs. ESC 2025
The European Society of Cardiology (ESC) published their own focused update on dyslipidemia in late 2025. While both the American and European guidelines emphasize early intervention and aggressive lowering of atherogenic lipoproteins, their frameworks differ slightly 1930.
The ESC guidelines rely on the Systematic Coronary Risk Evaluation 2 (SCORE2) and SCORE2-OP models, maintaining a highly structured, target-driven approach based on predefined risk categories 1931. In contrast, the AHA/ACC 2026 guidelines introduce a more dynamic model incorporating PREVENT, extensive use of coronary artery calcium (CAC) scoring to reclassify borderline risk, and shared physician-patient decision-making 1930. However, both major international bodies are entirely aligned on the critical importance of evaluating Lp(a) as a major risk modifier 1920.
Interim clinical management in 2026
As of mid-2026, the medical community exists in a transitional paradigm: clinicians can universally diagnose high Lp(a), but the FDA has not yet formally approved a drug explicitly indicated to lower the particle itself. Therefore, current clinical management relies heavily on the concept of holistic risk mitigation 11321.
Because the residual risk of high Lp(a) is multiplicative with other traditional risk factors, cardiologists aim to aggressively optimize every other modifiable variable a patient possesses 1314.
Restoring strict LDL targets and ApoB focus
The 2026 guidelines brought back definitive LDL-C treatment goals, operating under the philosophy that "lower for longer is better" 151722. * For primary prevention in borderline or intermediate-risk patients, the goal is LDL <100 mg/dL 1517. * For high-risk primary prevention, the target drops to <70 mg/dL 1517. * For secondary prevention (patients who have already experienced clinical ASCVD), the goal is <55 mg/dL, utilizing high-intensity statin therapy, ezetimibe, and PCSK9 inhibitors if necessary 141522.
Furthermore, the guidelines elevate the role of Apolipoprotein B (ApoB) testing. Because every single atherogenic particle - including standard LDL, very-low-density lipoprotein (VLDL), and Lp(a) - contains exactly one molecule of ApoB-100, measuring total ApoB provides a much more accurate assessment of a patient's true cardiovascular risk than measuring LDL cholesterol alone 1527. This is particularly vital for Lp(a) patients, as the cholesterol content of Lp(a) is actually lumped into the standard calculated LDL-C metric on basic lab reports. Without ApoB testing, a patient might appear to have adequately controlled cholesterol while still harboring a dangerous concentration of atherogenic particles 1327.
The role of Coronary Artery Calcium (CAC) scoring
The 2026 guidelines also vastly expanded the role of the coronary artery calcium (CAC) scan - a specialized, non-invasive CT scan of the heart. CAC scoring acts as a tiebreaker for patients whose need for medication is uncertain. The guidelines tie specific CAC score ranges directly to treatment intensity 141524: * CAC Score of 0: Often supports deferring statin therapy and focusing on lifestyle, provided there are no other extreme risk factors 24. * CAC Score 1 to 99: Recommends moderate-intensity statin therapy to aim for an LDL <100 mg/dL 1424. * CAC Score 100 to 999: Triggers intensive LDL-C reduction targets (<70 mg/dL) 1424. * CAC Score ≥1,000: Warrants the most aggressive secondary-prevention targets (LDL <55 mg/dL) 2422.
The 2026 drug pipeline: A pharmaceutical revolution
The intense focus on Lp(a) in 2026 is driven by the imminent arrival of a new class of targeted therapies that can virtually eradicate the particle from the human bloodstream 67.
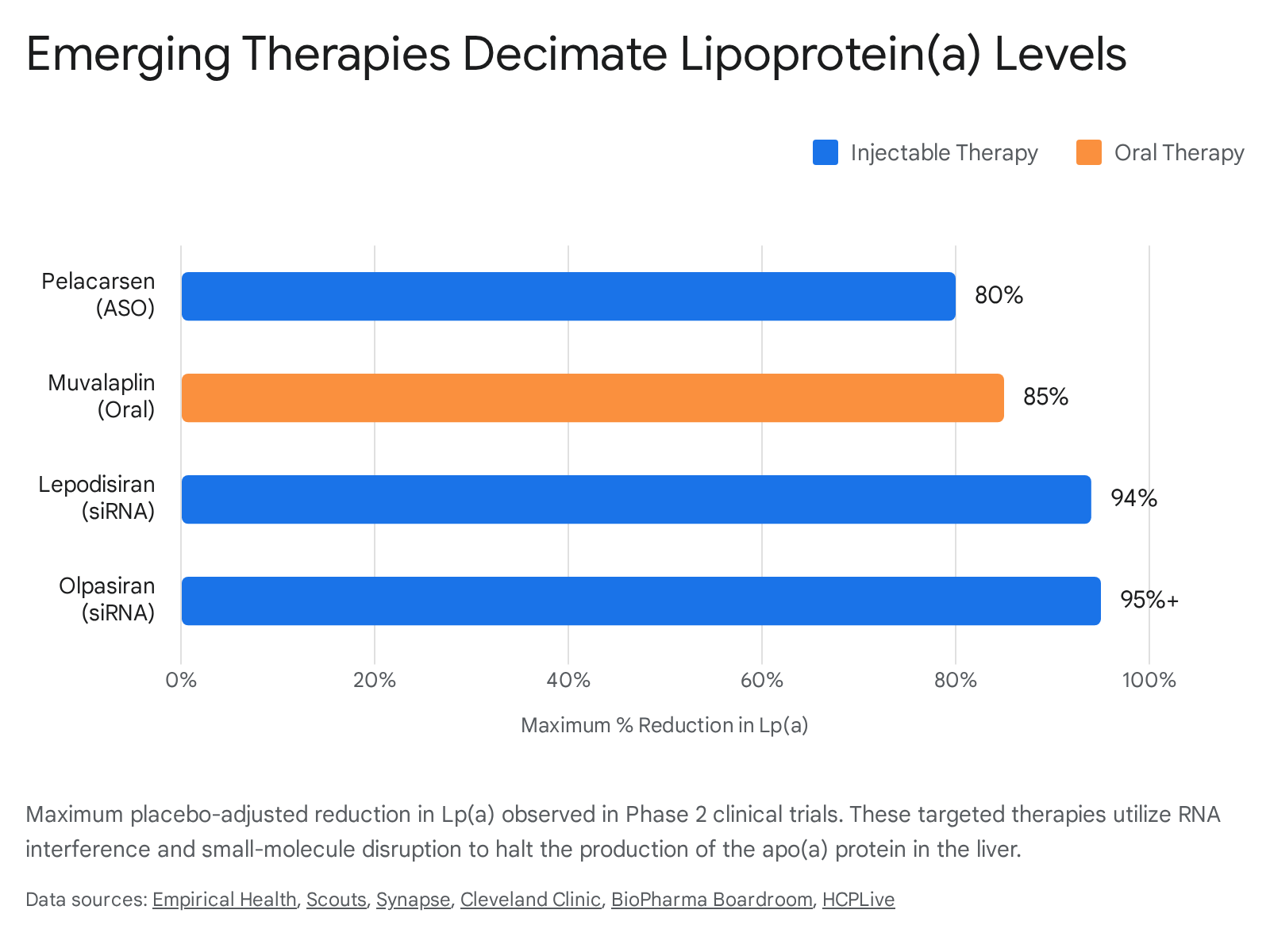
Using advanced genomic technologies, including RNA interference (RNAi) and targeted small molecules, pharmaceutical developers have finally discovered how to halt the liver from producing the problematic apo(a) protein in the first place 7. Four major therapies are currently progressing through late-stage clinical trials, demonstrating unprecedented reductions in Lp(a) ranging from 80% to over 95% 635.
1. Pelacarsen (Novartis / Ionis Pharmaceuticals)
Pelacarsen is an antisense oligonucleotide (ASO) therapy that reduces Lp(a) production directly in the liver. ASOs are short, synthetic strands of nucleotides designed to bind to specific messenger RNA (mRNA) sequences. When pelacarsen binds to the apolipoprotein(a) mRNA in hepatocytes, it triggers the degradation of the mRNA, completely preventing its translation into the apo(a) protein 7.
Administered via a monthly subcutaneous injection, pelacarsen lowered Lp(a) by up to 80% in Phase 2 trials 6736. The entire cardiology world is currently waiting on the results of the pivotal Lp(a)HORIZON trial 69. This massive Phase 3 cardiovascular outcomes study completed enrollment of 8,323 patients with established cardiovascular disease in 2023 636. Following a slight delay due to slower-than-expected cardiovascular event accrual, Novartis is expected to publish the highly anticipated readout in the first half of 2026, with regulatory submissions planned shortly thereafter if successful 6637. HORIZON is the first trial that will definitively validate or refute the entire class of Lp(a)-lowering medications 69.
2. Olpasiran (Amgen)
Olpasiran utilizes small interfering RNA (siRNA) technology to silence the LPA gene 6. While the end result is similar to pelacarsen, the siRNA molecular platform works through a different cellular mechanism, leading to a vastly different pharmacokinetic profile 7. Olpasiran offers incredibly durable effects, requiring an injection only once every 12 weeks 636.
In Phase 2 trials (OCEAN(a)-DOSE), olpasiran demonstrated astonishing potency, lowering Lp(a) by more than 95% at the highest doses 6. Amgen is currently conducting the Phase 3 OCEAN(a)-Outcomes trial, which tracks over 7,200 patients with established ASCVD, with an estimated primary completion date in early 2028 2339. Furthermore, Amgen initiated the OCEAN(a)-PreEvent trial to study the drug in patients who are at risk for a first major cardiovascular event, pushing into the primary prevention space 2425.
3. Lepodisiran (Eli Lilly)
Another highly potent siRNA therapy, lepodisiran, has demonstrated the potential for even less frequent administration. Following Phase 1 data, a Phase 2 trial revealed that a 400 mg dose of lepodisiran lowered Lp(a) levels by 94.8% after two doses, and impressively, levels remained 74.2% below baseline a full 360 days after the second dose 26. This extended duration suggests lepodisiran could eventually become a twice-a-year or even annual injection 26. Eli Lilly is actively advancing the Phase 3 ACCLAIM-Lp(a) trial, aiming to enroll 17,300 participants. Notably, ACCLAIM-Lp(a) includes high-risk primary prevention patients in addition to secondary prevention populations, broadening its potential future market applicability 262728.
4. Muvalaplin (Eli Lilly)
While RNA-based therapies show immense efficacy, they are universally administered via injection. Muvalaplin represents a completely different therapeutic modality: it is a traditional, once-daily oral pill 4546. Rather than preventing the liver from manufacturing the apo(a) protein, muvalaplin is a multivalent small molecule designed to physically block the initial interaction between the apo(a) protein and the apoB-100 particle, effectively disrupting the final assembly of the Lp(a) particle 45.
The Phase 2 KRAKEN trial, with results presented in late 2024 and early 2025, demonstrated that muvalaplin safely lowered Lp(a) by up to 85.8% (using an intact Lp(a) assay) with no major safety or tolerability concerns 454629. Following this success, Eli Lilly launched a massive 10,450-patient Phase 3 trial named MOVE-Lp(a) in late 2025 to definitively test its long-term cardiovascular benefits in both primary and secondary prevention cohorts 3049.
Summary Comparison: The 2026 Lp(a) Drug Pipeline
| Drug Candidate | Manufacturer | Modality & Delivery | Dosing Frequency | Max Phase 2 Lp(a) Reduction | Phase 3 Trial Name & Status |
|---|---|---|---|---|---|
| Pelacarsen | Novartis / Ionis | Antisense Oligonucleotide (Subcutaneous) | Monthly 67 | ~80% 636 | Lp(a)HORIZON (Readout expected H1 2026) 637 |
| Olpasiran | Amgen | siRNA (Subcutaneous) | Every 12 weeks 67 | >95% 6 | OCEAN(a)-Outcomes (Completion est. 2028) 2339 |
| Lepodisiran | Eli Lilly | siRNA (Subcutaneous) | Infrequent (up to annually) 26 | ~94% 626 | ACCLAIM-Lp(a) (Actively enrolling ~17,300 pts) 2627 |
| Muvalaplin | Eli Lilly | Small Molecule (Oral Pill) | Once Daily 4546 | ~85% 4529 | MOVE-Lp(a) (Actively enrolling ~10,450 pts) 3049 |
(Note: Another siRNA agent, Zerlasiran, demonstrated a 96.4% reduction in Phase 2 trials, but its Phase 3 program was placed on hold prior to 2026 50.)
The ultimate question: Does lowering it save lives?
Despite the monumental biochemical success of these emerging drugs in essentially erasing the particle from routine blood tests, one vital question remains scientifically unanswered in early 2026: Does artificially lowering Lp(a) actually translate into fewer heart attacks, strokes, and cardiovascular deaths? 669.
In the history of cardiovascular medicine, improving a surrogate biomarker does not automatically guarantee a clinical victory in human outcomes. An established and expanding body of high-quality epidemiological evidence and Mendelian randomization (genetic) data strongly supports a causal role of Lp(a) in cardiovascular disease 710. However, some complex genetic models have suggested that a therapy might need to lower Lp(a) by a massive absolute amount - perhaps by 100 mg/dL or more - to achieve the same clinical benefit observed from standard LDL-lowering therapies 3132.
Researchers modeling the potential public health impact estimate that more than 5.3 million US adults with established ASCVD and elevated Lp(a) could be eligible for these emerging treatments 33. If the therapies provide a 20% to 30% relative risk reduction, they could prevent between 25,000 and 74,000 recurrent cardiovascular events annually in the United States alone 33.
This lingering uncertainty is exactly why the Lp(a)HORIZON trial readout in mid-2026 is considered one of the biggest biotech events of the entire year 69. It is the first study powered and designed to definitively test the "Lp(a) hypothesis" in thousands of patients. If the data shows a significant reduction in major adverse cardiovascular events, it will validate the entire class of medications and usher in a new era of preventive cardiology 676. If it fails, it will force the scientific community to fundamentally reconsider the mechanisms of this dangerous genetic risk factor 7.
Bottom line
Lipoprotein(a) is a highly prevalent, genetically determined cholesterol particle that independently drives atherosclerosis, abnormal blood clotting, and heart valve disease, remaining completely unfazed by healthy diets or traditional statins. In 2026, major clinical guidelines formally demand that every adult be tested for Lp(a) at least once in their lifetime to uncover hidden cardiovascular risk decades before an event occurs. While the medical community eagerly awaits the pivotal 2026 clinical trial results to prove that novel, gene-silencing therapies can safely translate profound Lp(a) reductions into fewer heart attacks, patients today must work proactively with cardiologists to aggressively mitigate every other modifiable risk factor they carry.