What the Science Says About the Placebo Effect
The placebo effect is a measurable, neurobiological phenomenon where the brain produces real symptom relief in response to the context, rituals, and meaning of a medical treatment. Rather than being a mere psychological trick or a reporting bias, placebos trigger the brain's internal pharmacy to release natural painkillers and neurotransmitters like endorphins and dopamine. Current research demonstrates that this effect can be intentionally harnessed by healthcare providers through clinical empathy, realistic optimism, and open-label treatments to significantly improve patient outcomes.
Beyond Sugar Pills: Reframing the Meaning Response
For much of modern medical history, the placebo effect was viewed as a statistical nuisance. It was considered a baseline of experimental noise that scientists had to filter out in randomized controlled trials to prove a pharmaceutical drug's true efficacy. Patients in the control group were given an inert substance, such as a sugar pill or a saline injection, and any subsequent improvement in their condition was often dismissed. Researchers historically attributed these improvements to the patient simply imagining they were better, reporting biases, or the natural, episodic resolution of the illness over time 12.
Today, the scientific consensus has dramatically shifted, redefining the placebo effect from a nuisance to a legitimate, targetable biological response. Experts now recognize that the placebo effect is not a single, monolithic phenomenon, but a complex tapestry of biological responses governed by expectation, conditioning, and context. Ted Kaptchuk, a pioneering researcher and director of the Program in Placebo Studies and the Therapeutic Encounter (PiPS) at Harvard Medical School, suggests that the term "placebo effect" is actually an oxymoron. The phrase implies that an inert substance is causing an effect, which is scientifically impossible. Instead, Kaptchuk and contemporary medical anthropologists advocate for the term "meaning response" 334.
This framework posits that the healing effect comes from everything surrounding the pill. The clinical environment, the therapeutic interaction between patient and provider, the symbols of healthcare such as a doctor's white coat or a stethoscope, and the conscious and subconscious expectations of recovery all contribute to this meaning response 335. When a patient interacts with a trusted physician, undergoes the familiar ritual of a medical examination, and receives a formal diagnosis along with a treatment plan, their brain interprets these social and environmental cues as signals that healing is imminent. This profound social interaction can effectively potentiate the physiological effects of real pharmaceutical drugs, or in the case of placebo administration, trigger profound relief all on its own 23.
The Neurobiology: Opening the Internal Pharmacy
The paradigm shift from viewing placebos as a psychological quirk to a hard-science reality was driven largely by the advent of modern neuroimaging and physiological monitoring. Fabrizio Benedetti, a leading neurophysiologist at the University of Turin, has spent decades mapping what he terms the brain's "internal pharmacy." This concept describes the endogenous chemical faculties that explain our capacity to recognize and biologically respond to the therapeutic context of medicine 68.
Benedetti's extensive body of research demonstrates that placebos activate the exact same biochemical pathways as active drugs. In pain management, for instance, the sheer expectation of pain relief triggers the release of endogenous opioids, such as endorphins, and activates the body's endocannabinoid system. This biochemical cascade effectively dampens activity in the brain's pain-sensitive regions, providing measurable, physical analgesia 97.
One of the most compelling and direct demonstrations of this internal pharmacy occurred during Benedetti's research on patients with Parkinson's disease who were undergoing deep brain stimulation surgery. While patients were awake during the procedure, electrodes monitored the real-time firing of individual neurons in the subthalamic nucleus. When patients were given a simple saline injection but were explicitly told it was a powerful anti-Parkinson's drug called apomorphine, the monitoring equipment captured an immediate, dramatic decrease in the erratic firing of neurons. This neural shift was accompanied by a visibly measurable reduction in muscle rigidity 811. The brain, anticipating an influx of dopamine from the promised medication, simply mobilized its own internal dopamine reserves to achieve the predicted clinical outcome.
The mechanisms of the placebo effect are a double-edged sword. Just as positive expectations can trigger healing, negative expectations can trigger the "nocebo effect." If a patient is explicitly warned about severe side effects, or if they harbor a deep lack of trust in their healthcare provider, the brain activates cholecystokinin (CCK) and cyclooxygenase networks. These networks amplify anxiety and augment pain signaling 978. Neuroimaging studies further reveal that while positive placebos modulate pain reception areas, nocebos heavily activate the hippocampus and the amygdala, which are brain regions deeply tied to memory, threat detection, and fear processing 8.
Decoding the Placebome: Why We Respond Differently
A persistent challenge in both clinical medicine and pharmacological research is the vast heterogeneity of the placebo response. An inert pill accompanied by a doctor's reassurance might completely cure one patient's chronic migraine while doing absolutely nothing for another patient with the exact same condition. Recent advances in systems pharmacogenomics suggest that an individual's unique genetic makeup plays a massive, previously unrecognized role in their susceptibility to context-driven healing. This has given rise to the concept of the "placebome" 2910.
The placebome comprises a network of genetic variants that dictate the synthesis, signaling, and metabolism of the specific neurotransmitters involved in expectation and reward 9. By isolating these genes, researchers are beginning to understand why the meaning response is highly active in some demographic groups and dormant in others.
| Genetic Biomarker | Primary Neurotransmitter System | Mechanism of Action in the Placebo Response | Clinical Implications |
|---|---|---|---|
| COMT Gene | Dopamine | Regulates how quickly dopamine is cleared from the prefrontal cortex. Slower clearance means higher dopamine retention during a therapeutic encounter. | Individuals with certain COMT variants exhibit exceptionally strong placebo responses, particularly in pain and psychiatric trials 910. |
| OPRM1 Gene | Endogenous Opioids | Encodes the mu-opioid receptor, which is the primary site of action for pain modulation and endorphin binding. | Polymorphisms in this gene dictate an individual's baseline ability to produce and utilize natural painkillers when they expect a treatment to work 29. |
| HTR2A Gene | Serotonin | Modulates serotonin receptor sensitivity, impacting mood regulation, anxiety, and the cognitive processing of clinical rituals. | Variations influence the magnitude of placebo-induced mood improvements in clinical trials for major depressive disorder 29. |
Understanding the placebome holds profound implications for the future of pharmaceutical development and clinical trial design. Unrecognized differences in placebo-response genetics between a treatment arm and a control arm can inadvertently lead to false-negative trial failures. In these scenarios, a potentially life-saving drug might appear statistically ineffective simply because the specific cohort of patients randomly assigned to the placebo group happened to be genetically predisposed to an exceptionally high natural healing response 10. This phenomenon is actively being studied as a potential factor in the high failure rates of Alzheimer's disease therapeutics, where genetic background effects and trial heterogeneity may mask true drug efficacy 10.
The Impact of Ritual, Cost, and Culture
Because the placebo effect is fundamentally a meaning response, the physical properties of the treatment and the deeply ingrained cultural background of the patient drastically alter its efficacy. The brain essentially acts as a predictive engine, calculating the value and power of a medical intervention based on accumulated social learning, media narratives, and sensory input 1516.
Decades of data reveal that the physical theater of medicine matters deeply to the human nervous system. Studies consistently show a hierarchy of placebo effectiveness based on the perceived invasiveness of the procedure. Fake surgeries and sham acupuncture generally produce stronger and longer-lasting placebo effects than placebo injections. Placebo injections, in turn, are universally more powerful than oral placebo pills 23. Furthermore, aesthetics and dosage manipulate the brain's expectations. Two placebo pills work significantly better than one. Large pills are perceived as stronger than small ones. Even color drives specific biological expectations: pink or red placebo pills yield stronger stimulant effects, while blue pills are vastly more effective when prescribed as sedatives or sleep aids 1516. Cost is another powerful driver. Patients given a placebo that is branded as an expensive, newly released painkiller report significantly higher pain tolerance than those given the exact same placebo but told it was a heavily discounted, generic drug 316.
The Anthropology of Healing
The placebo effect is heavily mediated by cultural norms, religious contexts, and national belief systems. A well-documented anthropological review of placebo treatments for gastric ulcers found astonishing geographic variance for the exact same sham intervention. The placebo healing rate was a remarkable 59 percent in Germany, roughly 22 percent in Denmark and the Netherlands, and a mere 7 percent in Brazil 1711. Researchers posit that these differences stem from how different cultures internalize medical authority and the meaning of clinical rituals.
Cultural preferences also dictate how patients interact with providers, directly impacting the therapeutic bond that fuels the placebo effect. Studies investigating physician bedside manner show that individuals of European descent in North America often derive better subjective well-being and health information retention from physicians who project high-arousal, "excitement-focused" optimism. In stark contrast, Asian American populations tend to respond more favorably to "calm-focused" physicians. This aligns with specific cultural norms that value balanced, low-arousal emotional states, demonstrating that a doctor's demeanor must match the patient's cultural expectations to maximize the meaning response 1213.
Similarly, cross-cultural studies reveal a strong "naturalness bias" - a global preference for treatments labeled as natural over synthetic - that influences vaccine and drug acceptance. However, data indicates that Chinese populations show a significantly heightened sensitivity to this naturalness bias in the context of vaccination compared to North American cohorts, meaning their placebo or nocebo responses to vaccines are more heavily influenced by the perceived origin of the medicine 14. Furthermore, deep-seated traditional beliefs can manifest in literal life-or-death nocebo effects. A study examining Chinese Americans who held traditional beliefs associating specific birth years with specific organ vulnerabilities (e.g., the lung) found that these individuals died several years earlier than comparable European Americans when they contracted diseases matching their astrological vulnerability. The researchers concluded this was driven heavily by the psychosomatic burden of expecting a fatal outcome based on cultural transmission 17.
How Placebos Perform Across Medical Conditions
The placebo effect is not a cure-all. It does not shrink cancerous tumors, cure severe viral infections, or mend broken bones. Its domain is primarily illnesses that are heavily mediated by the central nervous system, where subjective experience, autonomic regulation, and conscious perception intersect. The most profound placebo responses are documented in chronic pain, fatigue, nausea, depression, and anxiety 27.
The Pain Paradox: Growing Placebo Responses
In the realm of neuropathic pain, a fascinating and somewhat troubling phenomenon is occurring: the placebo effect is actively getting stronger. Recent systematic reviews have highlighted that the placebo response in clinical trials for neuropathic pain analgesics has steadily increased over the last two decades, but this inflation is almost entirely isolated to trials conducted in the United States 1523.
This geographical inflation makes it increasingly difficult for new pharmaceutical drugs to statistically outperform placebos in the American regulatory environment. Researchers attribute this specifically to US-based trials becoming vastly larger and significantly longer in duration. The rigorous attention, compassionate care, and frequent medical monitoring that trial participants receive in these extended modern studies act as a massive, continuous placebo intervention in itself 152316. The sheer volume of positive psychosocial interaction essentially out-muscles the pharmacological effects of the novel drugs being tested.
Psychiatric Disorders: A 2024 Meta-Analysis
In psychiatry, the placebo effect is foundational to both historical and modern treatment outcomes. A landmark 2024 systematic review and meta-analysis published in JAMA Psychiatry quantified the exact magnitude of the placebo response across 90 high-quality randomized controlled trials. This massive undertaking encompassed nearly 10,000 placebo-treated participants across nine major psychiatric diagnoses 16251718.
The researchers utilized Cohen's d to measure effect sizes, a statistical standard where a value above 1.2 is considered a very large and highly clinically significant change.
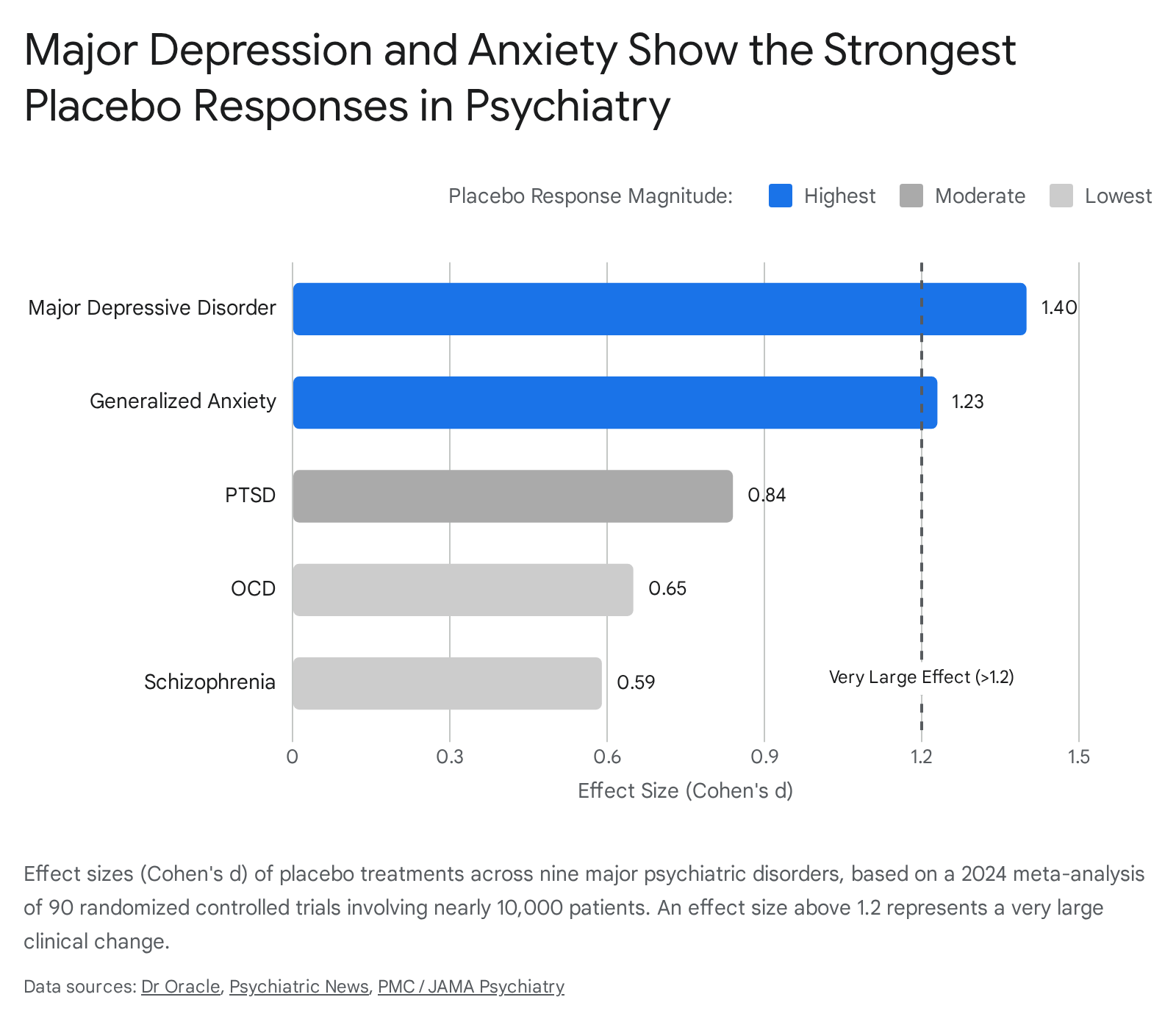
The data definitively revealed that while all nine psychiatric conditions showed statistically significant symptom improvement under placebo treatment, the magnitude of that improvement varied wildly depending on the specific diagnosis 1617.
| Psychiatric Diagnosis | Placebo Effect Size (Cohen's d) | 95% Confidence Interval | Clinical Response Category |
|---|---|---|---|
| Major Depressive Disorder (MDD) | 1.40 | 1.24 - 1.56 | Highest |
| Generalized Anxiety Disorder (GAD) | 1.23 | 1.06 - 1.41 | Highest |
| Mania | ~0.92* | 0.68 - 0.92 (Range) | Moderate |
| Social Phobia | ~0.88* | 0.68 - 0.92 (Range) | Moderate |
| Posttraumatic Stress Disorder (PTSD) | 0.84 | 0.68 - 0.92 (Range) | Moderate |
| ADHD | ~0.75* | 0.68 - 0.92 (Range) | Moderate |
| Panic Disorder | ~0.68* | 0.68 - 0.92 (Range) | Moderate |
| Obsessive-Compulsive Disorder (OCD) | 0.65 | 0.51 - 0.78 | Lowest |
| Schizophrenia | 0.59 | 0.41 - 0.76 | Lowest |
(Note: Exact point estimates for Moderate category disorders fall within the provided 0.68 - 0.92 range based on the pooled meta-analysis data 2517).
Cognitive Architectures: Why OCD and Schizophrenia Resist Placebos
The stark contrast in the 2024 meta-analysis data begs a deeper physiological question: why do patients with major depression and anxiety exhibit massive, curative responses to placebos, while patients with schizophrenia and obsessive-compulsive disorder (OCD) derive the absolute least benefit? Furthermore, these latter two conditions suffer the highest dropout rates in clinical trials due to a perceived lack of efficacy from the patients 1625.
Researchers posit that the underlying neurological architecture of these specific conditions fundamentally disrupts the cognitive mechanisms required to process a placebo. To understand this, one must look at how the brain learns. The placebo effect relies heavily on "model-based" or goal-directed learning. This is the brain's ability to take in new contextual information - such as a doctor handing over a pill and explaining its benefits - and actively update its internal model of the world to predict a positive, pain-free outcome 1929.
Extensive neurocognitive research, particularly a foundational study by Voon et al. (2015), demonstrates that individuals with OCD suffer from severe deficits in this exact type of model-based control. Their neural circuitry, specifically the frontostriatal connectivity involving the dorsal caudate and the ventromedial prefrontal cortex, biases them heavily toward "model-free" or habitual learning 1920. Because their brains are essentially locked into deeply ingrained, rigid stimulus-response habits, they severely struggle to dynamically update their expectations based on the positive psychosocial cues of a clinical trial. When an OCD patient receives a placebo, their brain lacks the cognitive flexibility to rewrite its threat-estimation model, blocking the meaning response from taking root 19.
Similarly, patients with schizophrenia often exhibit a distinct and pervasive cognitive bias where they allocate their neural resources toward loss avoidance rather than reward pursuit 3132. The therapeutic encounter relies on a patient anticipating a reward - specifically, the reward of healing. Because early psychosis and schizophrenia trigger a reallocation of cognitive resources away from reward processing, the expectation of getting better simply does not compute biologically. Coupled with the impaired interpersonal functioning and blunted affect common in schizophrenia, these patients are significantly less likely to internalize the personal attention, empathy, and non-specific care elements that traditionally drive robust placebo responses in other populations 1631.
Harnessing the Placebo Effect Ethically in Practice
If the placebo effect is a powerful, neurobiological mechanism that drives a massive portion of healing in depression, anxiety, and pain, a vital ethical question emerges for modern medicine: How can doctors intentionally use it? For decades, clinical guidelines and medical ethics boards strictly prohibited the use of placebos in routine practice because it required outright deception. Lying to a patient to trick them into feeling better violates the core modern medical tenet of informed consent 2.
However, modern research has pioneered novel pathways to bypass this ethical dilemma entirely, bringing the power of the placebo into the light.
Open-Label Placebos
Ted Kaptchuk's team at the Harvard Program in Placebo Studies shocked the medical establishment by demonstrating the robust efficacy of "open-label placebos" (OLPs). In these groundbreaking trials, doctors give patients entirely inert pills but tell them explicitly and honestly what they are. A physician might say, "These are sugar pills with absolutely no active medication in them. However, rigorous clinical trials have shown that taking them can trigger the body's natural self-healing processes through the mind-body connection" 821.
Counterintuitively, the placebo effect survives the disclosure. Patients with a variety of conditions ranging from irritable bowel syndrome to severe chronic lower back pain experienced significant, measurable relief despite knowing with absolute certainty that they were taking a fake pill 22235. The physical ritual of taking a daily pill, combined with a scientifically grounded rationale that the body possesses an internal pharmacy capable of healing itself, is enough to engage the brain's neurobiological response without relying on any deception 336.
The Empathico Approach and Clinical Empathy
The most practical and widely applicable way to harness the placebo effect does not involve prescribing dummy pills - open-label or otherwise. It involves maximizing the "meaning response" alongside real, evidence-based pharmacological treatments. The total efficacy of any standard drug is essentially its pure pharmacological effect plus the placebo effect generated by the context in which it is prescribed 2338.
To formalize and teach this skill, researchers at the University of Southampton developed a digital training intervention called "Empathico." This evidence-based protocol is designed to train primary care practitioners to optimize the placebo response during routine, time-constrained consultations 383924. Focused initially on patients suffering from osteoarthritis, Empathico trains doctors to systematically deploy two core behaviors: 1. Clinical Empathy: This involves active listening, validating the patient's lived experience, providing explicit emotional support, and displaying physical warmth through eye contact, a calming tone of voice, and appropriate reassuring touch. 2. Realistic Optimism: This involves framing treatments positively rather than defensively. Instead of saying, "Let's try this painkiller, though there's a 30 percent chance it won't work and it might cause nausea," the physician is trained to say, "I am prescribing this medicine to help your body heal; the vast majority of my patients see great improvement with this exact treatment."
By merging an empathetic understanding of the patient's specific values with a confident, supportive delivery, clinicians can drastically lower patient anxiety. This builds deep interpersonal trust and reliably cues the brain's reward and pain-modulation systems to optimize the physical response to the actual drugs being prescribed 36233825.
This optimization extends into digital medicine as well. Recent trials of digital cognitive-behavioral therapeutics, such as the app "reclarit" used in rheumatoid arthritis care, have shown that delivering structured psychological support and positive reframing can yield immediate and sustained improvements in mental health and fatigue. These digital platforms act as a highly effective placebo delivery mechanism, proving that the meaning response can be digitized and delivered alongside standard pharmacological care to alleviate symptoms that disease-modifying drugs fail to fix 42264427.
Bottom line
The placebo effect is a profound neurobiological process where the brain translates the psychosocial context of a therapeutic encounter into measurable physiological changes, such as the release of endogenous opioids and dopamine. While its efficacy varies significantly - proving incredibly potent for mood disorders like depression and anxiety but less effective for conditions like OCD and schizophrenia due to their rigid cognitive architectures - it remains a pervasive force in all medical interventions. Moving forward, the medical community's challenge is not to eliminate the placebo effect as a nuisance, but to ethically maximize its power through genetic insights, open-label transparency, and the intentional, systemic application of clinical empathy.