How the Placebo Response Affects Your Brain and Body
The placebo response is not an illusion or a trick of the mind, but a measurable biological event where your expectations and conditioned habits trigger the release of the body's natural painkillers, dopamine, and mood-elevating chemicals. When you anticipate healing, specific neural circuits - including a newly mapped pathway linking the prefrontal cortex to the brainstem - physically activate to reduce pain, improve motor function, and modulate your immune system. While placebos cannot cure objective pathologies like infections or tumors, they profoundly alter how your brain and body construct the experience of illness, proving that the context of care is an active medical ingredient.
The Evolution of Placebo Science
For the better part of the twentieth century, modern medicine treated the placebo effect as an annoyance. Researchers viewed it as a statistical ghost - an inconvenience that needed to be subtracted in clinical trials so the true, molecular mechanisms of an active drug could be clearly measured 1. Placebos were seen merely as deceptive tools designed to trick a control group, ensuring that patients could not consciously bias the outcome of a study 22. Under this outdated paradigm, the body was considered a passive recipient of treatment, and healing was thought to be reducible exclusively to pharmacology and physical intervention 13.
However, the advent of advanced functional neuroimaging, genetic sequencing, and psychoneuroimmunology has fundamentally rewritten this narrative. The placebo response is now universally recognized by researchers as a potent, psychobiological phenomenon 45. It reveals that the human nervous system is an active, predictive engine that continuously translates environmental cues - such as a doctor's reassuring tone, the sterile smell of a clinic, or the ritual of swallowing a pill - into profound physiological changes 16.
Far from being "just in your head," the placebo response is physically rooted in the biology of the brain and body. By tracing the exact neural circuits that light up during a placebo response and mapping the chemical neurotransmitters that flood the nervous system, scientists have proven that belief, expectation, and clinical context are physiological forces capable of altering the trajectory of chronic diseases 147.
The Anatomy of Belief: Mapping the Placebo Brain
When a patient takes an inert substance believing it to be a potent drug, their brain does not remain idle. Functional magnetic resonance imaging (fMRI) and positron emission tomography (PET) scans consistently show that placebo treatments fundamentally alter metabolic activity within distinct, measurable brain networks 8. The areas most consistently engaged involve complex matrices responsible for pain modulation, emotional regulation, and cognitive prediction.
The Prefrontal Cortex and the Expectation Engine
The genesis of the placebo response largely resides in the prefrontal cortex, the evolutionary seat of human reasoning, planning, and conscious expectation 89. When a medical professional provides a positive prognosis, the dorsolateral prefrontal cortex begins constructing a predictive model of healing 10.
Because the brain functions as a prediction machine - preferring that internal sensations match its external models - this expectation generates top-down signals that cascade into deeper, older regions of the brain. The prefrontal cortex communicates with the anterior insula, which processes bodily sensations, and the nucleus accumbens, which governs reward anticipation, effectively priming the nervous system to experience relief before any chemical has entered the bloodstream 811.
The Cortico-Ponto-Cerebellar Pathway
In 2024, researchers achieved a monumental breakthrough in understanding the exact physical architecture of placebo-induced pain relief, an effect known clinically as placebo analgesia. A landmark study published in the journal Nature managed to trace the underlying neural circuits of the placebo response with single-cell precision 121314.
To simulate the human expectation of pain relief, scientists conditioned laboratory mice by moving them from a painfully hot floor environment (48°C) to a comfortably cool chamber (30°C). Over several days, the mice learned to strongly expect relief upon entering the second chamber. When researchers subsequently heated the floors in both chambers to a painful level, the conditioned mice still exhibited prolonged pain relief behaviors in the second chamber - a classic, observable placebo response 1215.
By closely monitoring the brain activity of these mice in real-time, researchers identified a previously unknown pathway connecting the higher and lower brain. Neurons within the rostral anterior cingulate cortex (rACC) - a region at the front of the brain heavily tied to the expectation of pain relief - fired intensely, projecting signals down to the pontine nucleus (Pn) located in the brainstem 1314.
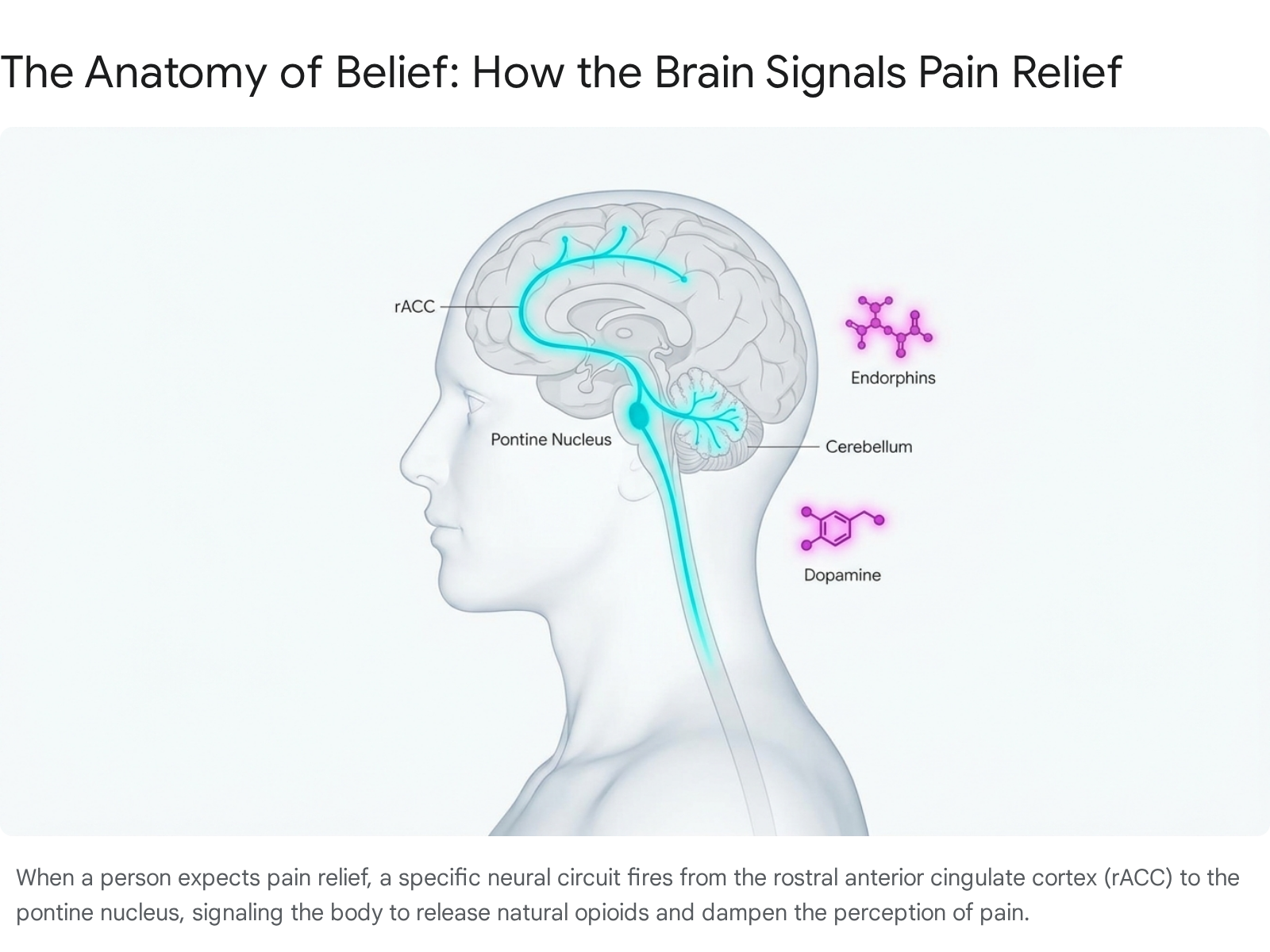
The pontine nucleus serves as a critical connector to the cerebellum, a region mostly famous for coordinating physical movement. Crucially, the researchers discovered that the pontine nucleus was exceptionally dense with pain-modulating opioid receptors (specifically, Oprd1-expressing neurons) 121315. When the scientists used advanced optogenetic tools to inhibit this specific rACC-to-Pn pathway, the mice completely lost their placebo pain relief. Conversely, artificially activating this exact circuit provided significant pain relief even when the mice had undergone no psychological conditioning at all 14. This discovery rewrote anatomical textbooks, demonstrating that the cerebellum is deeply involved in cognitive pain modulation and the physical manifestation of belief 1516.
Amygdala Downregulation and Emotional Control
Beyond managing pain, the placebo effect profoundly influences emotional and psychological distress. In clinical trials treating psychiatric conditions like social anxiety disorder (SAD) and generalized anxiety disorder (GAD), patients taking placebos often report massive, life-altering reductions in stress 817.
Neuroimaging reveals exactly how this happens. During placebo-induced anxiety relief, there is a sharp and sustained decrease in the metabolic activity of the amygdala, the almond-shaped cluster of nuclei that serves as the brain's primary fear, threat, and emotion processing center 717. The cognitive expectation of feeling calmer signals the prefrontal cortex to exert inhibitory control over the amygdala, effectively forcing the brain's alarm system to power down. This proves that placebo anxiolysis is not merely a change in attitude, but a functional deactivation of the brain's panic circuitry 717.
The Chemical Messengers of Healing
The complex physical circuits of the brain rely entirely on chemical messengers to communicate and exert their effects on the body. The placebo response is defined by the rapid release of several distinct neurotransmitters, and the specific cocktail of chemicals released depends heavily on the condition being treated and the precise expectations of the patient.
Endogenous Opioids and the Pain Matrix
The most rigorously studied and understood mechanism of the placebo effect is its ability to trigger the release of endogenous opioids. These are the body's natural, internally manufactured painkillers, which include endorphins and enkephalins 711.
When a patient takes a pill that they believe is a powerful analgesic for a severe headache or chronic back pain, the brain signals the release of these endorphins. They flood into the periaqueductal gray (PAG) and down into the spinal cord, binding tightly to mu-opioid receptors. This physical binding actually blocks nociceptive pain signals from traveling up the spinal cord to reach conscious awareness 718. This endogenous release is so identical to pharmaceutical pain relief that if a patient is given naloxone - a drug that blocks opioid receptors and is commonly used to reverse heroin overdoses - their placebo pain relief is instantly wiped out, proving the effect relies on actual opioid chemistry 718.
Dopamine, Reward, and Parkinson's Disease
While the opioid system primarily manages pain inhibition, the dopaminergic system governs reward anticipation, motivation, and motor control 719. Dopamine pathways are heavily activated when a patient anticipates a clinical benefit, acting as a massive neurochemical "reward" signal 20.
This mechanism is most vividly observable in Parkinson's disease, a severe neurodegenerative disorder caused by the progressive death of dopamine-producing neurons in the substantia nigra. When Parkinson's patients are given a placebo that they firmly believe to be their levodopa medication, PET scans reveal a massive surge of endogenous dopamine release in the striatum, specifically within the caudate and putamen 7181920.
This chemical surge displaces radioactive tracers on the scans by up to 19 percent, a physiological change so powerful that it visibly reduces the patients' muscle rigidity and physical tremors 1019. It provides undeniable proof that the strong expectation of a drug can command the brain to manufacture and deploy the missing chemical itself 711.
Serotonin, Cannabinoids, and Mood Regulation
The biological versatility of the placebo response allows it to hijack other major neurotransmitter systems depending on the context. In some specific forms of pain relief, placebos bypass the opioid system entirely and instead activate the body's endocannabinoid system, utilizing CB1 receptors to diminish pain 67. In treatments involving depression, mood disorders, and anxiety, placebos robustly engage the serotonin system to help regulate emotional distress, mimicking the exact pathways targeted by selective serotonin reuptake inhibitors (SSRIs) 8917.
The Nocebo Effect and Cholecystokinin (CCK)
This neurochemical versatility also possesses a darker, equally powerful counterpart. When a patient is informed that a treatment may cause harm, or when they hold deep anxieties about potential side effects, they frequently experience the nocebo effect 19.
Negative expectations physically trigger the release of cholecystokinin (CCK), a hormone and neurotransmitter that actively antagonizes and overrides the body's opioid system 61821. This release heightens the perception of pain (hyperalgesia) and can generate very real, debilitating side effects like severe nausea, dizziness, or jitteriness out of thin air 1823. The nocebo effect underscores a critical ethical dilemma in medicine: the words a doctor uses to describe a drug's potential side effects can literally synthesize those adverse events in the patient's body 123.
| Medical Condition / Context | Primary Neurotransmitters Involved | Key Brain Regions Activated/Modulated | Typical Symptoms Relieved or Altered |
|---|---|---|---|
| Pain Syndromes (Analgesia) | Endogenous opioids (Endorphins), Cannabinoids | rACC, Pontine Nucleus, PAG, Insula | Aching, hyperalgesia, surgical recovery 714 |
| Parkinson's Disease | Dopamine | Striatum (Caudate, Putamen), Nucleus Accumbens | Motor stiffness, resting tremors, bradykinesia 1819 |
| Anxiety & Depression | Serotonin, Dopamine | Amygdala (downregulated), Prefrontal Cortex | Emotional distress, acute fear response 817 |
| Negative Expectations (Nocebo) | Cholecystokinin (CCK) | Hippocampus, Amygdala (hyperactivated) | Increased pain sensitivity, nausea, fatigue 1823 |
Is the Placebo Effect in Your DNA? Unlocking the "Placebome"
If placebos are powerful enough to mimic opioids and synthesize dopamine, a persistent question arises: why doesn't everyone respond to a placebo equally? Some patients experience miraculous recoveries on sugar pills, while others feel absolutely nothing.
Researchers have recently discovered that the propensity to experience a placebo effect is heavily predetermined by human genetics - a burgeoning field of study that scientists have officially dubbed the "placebome" 82223. Because the placebo response relies entirely on specific neurochemical pathways, slight inherited variations in the genes that build those pathways can make a person exceptionally receptive, or completely immune, to placebo interventions 48.
Key Genetic Polymorphisms
Scientists have isolated a growing list of genetic polymorphisms that dictate placebo responsiveness, primarily focusing on the dopaminergic, opioid, serotonergic, and endocannabinoid systems 2122.
- OPRM1 (rs1799971): This specific gene codes for the mu-opioid receptor, the exact cellular lock that endogenous endorphins fit into. Individuals carrying a specific variant (the A/A carrier combination) produce receptors that bind much more effectively to the endorphins released during a placebo response. Consequently, these individuals experience dramatically higher levels of placebo-induced pain relief compared to those with other genetic combinations 222324.
- COMT (rs4680): This gene regulates an enzyme (catechol-O-methyltransferase) responsible for breaking down dopamine in the prefrontal cortex. People possessing a variant that results in higher, sustained dopamine levels (the met/met variant) tend to have much stronger and longer-lasting placebo responses across conditions ranging from irritable bowel syndrome (IBS) to idiopathic chronic pain 2224.
- FAAH (rs324420): This gene dictates the breakdown of natural endocannabinoids in the nervous system. Certain missense mutations (Pro129Thr) significantly increase the baseline amount of natural cannabinoids available in the brain, priming the patient for heightened placebo analgesia 22.
- TPH2: Polymorphisms in this serotonin-related tryptophan hydroxylase-2 gene have been directly linked to a patient's capacity to modulate amygdala activity. Patients with specific variants of this gene are significantly more likely to experience clinical anxiety relief from placebo treatments 1721.
Fascinatingly, these genes can interact. When individuals possess a combination of multiple high-responder variants - such as carrying both the COMT met/met variant and the OPRM1 A/A variant - they can report a magnitude of placebo-induced pain reduction that is four to six times higher than individuals with opposite, low-responder genetic profiles 2224.
Transcriptomics and Gene Expression
Inherited DNA is only part of the story; recent research has pushed the boundaries of the placebome by exploring gene expression - how genes are actively turned on or off in real-time.
In a recent highly sophisticated study, researchers took blood samples from chronic pain patients undergoing an intensive placebo conditioning trial. By performing total RNA sequencing, the researchers identified 667 differentially expressed genes (DEGs) that strongly correlated with placebo responsivity 22.
Patients who exhibited the strongest placebo relief showed significant upregulation in specific genes, including FBXL15, PI3, TNFRSF4, and CCDC85B 2224. Interestingly, many of these highly expressed genes are heavily involved in deeper biological processes entirely separate from the nervous system, such as cellular division, RNA metabolism, ribosome biogenesis, and the survival of immune T-cells 2224. This transcriptomic data strongly hints at a profound, systemic link between the brain's cognitive expectation of relief and the body's fundamental cellular environment.
Psychology of Healing: Expectation vs. Conditioning
The biological and genetic machinery of the placebo effect lies dormant until it is given a psychological spark. In clinical settings, this spark generally comes from two distinct, yet overlapping mechanisms: conscious expectation and unconscious conditioning 111925.
The Power of Conscious Expectation and Ritual
Expectation is the explicit, cognitive anticipation of a future clinical outcome 11. When an authoritative physician hands a patient a brightly colored capsule and confidently states, "This is a highly advanced, newly approved medication that will drastically reduce your pain," the patient's prefrontal cortex instantly builds a predictive model of healing and comfort 2.
Because the brain functions as a predictive organism, it deploys physiological changes to ensure the body aligns with this consciously expected outcome 1. The magnitude of this expectation is heavily influenced by what medical anthropologists call the "therapeutic ritual" - the perceived expertise of the provider, the gravity of the clinical environment, the branding on the pill bottle, and the invasiveness of the procedure 12.
Extensive studies consistently show that two placebo pills work better than one, that placebo injections produce significantly stronger effects than placebo pills, and that sham surgeries (where a patient is cut open and sutured without anything being repaired) produce the most massive placebo effects of all 28. This occurs because complex, invasive interventions carry a much heavier psychological weight of expected healing, commanding a larger neurochemical response from the brain.
Pavlovian Conditioning in the Body
While expectation requires conscious thought and belief, conditioning is entirely unconscious and autonomic. Just as Pavlov's famous dogs learned to salivate at the mere sound of a bell, the human body learns to associate the repetitive sensory cues of medical treatment - the antiseptic smell of a hospital room, the physical shape and taste of a pill, the sting of a needle - with a specific biological response 825.
If a patient takes an active pharmaceutical painkiller every day for two weeks, their body biologically associates the ritual of swallowing that pill with the onset of opioid receptor activation. If the active pill is secretly swapped for an identical sugar pill on the fifteenth day, the body will still release a flood of endogenous endorphins out of pure physiological habit 1119. Conditioning is incredibly powerful because it bypasses conscious skepticism. It is responsible for generating placebo responses in biological domains that patients cannot consciously control, such as hormone secretion, blood pressure, and immune system activity 1119.
Psychoneuroimmunology: Training the Immune System
The reality of autonomic conditioning proves that the placebo effect extends far beyond the central nervous system. The rapidly growing field of psychoneuroimmunology has demonstrated that the brain's activity maintains direct, mutual communication with the peripheral immune and endocrine systems 71925.
Through Pavlovian conditioning, the immune system can literally be "trained." In landmark medical experiments, subjects were repeatedly given a powerful immunosuppressive drug alongside a strongly flavored, novel drink (acting as the conditioned stimulus). After several days of pairing, the active drug was secretly removed, but the flavored drink was administered alone. Astoundingly, the subjects' immune systems still suppressed themselves 1925.
The brain had recognized the taste of the drink, activated the insular cortex and amygdala, and deployed noradrenaline to force the immune system to mimic the drug's effect based purely on sensory cues 1925. Furthermore, in clinical studies treating allergic rhinitis and asthma, placebo treatments have successfully reduced objective markers of inflammation, such as pro-inflammatory cytokines in the bloodstream, proving that the mind's expectations can alter the body's defensive chemistry 826.
How Placebos Impact Clinical Trials
The massive biological power of the placebo response presents a severe, multi-billion-dollar dilemma for modern medical research. In randomized controlled trials (RCTs), new drugs must prove they are significantly more effective than a placebo to gain regulatory approval 2. However, this is becoming increasingly difficult.
The Creeping Placebo Effect in Psychiatry
Over the last few decades, the baseline placebo response in clinical trials has grown steadily stronger, a phenomenon particularly acute in wealthy nations like the United States 227. As direct-to-consumer drug advertising has skyrocketed, societal expectations of medical miracles have vastly increased, inflating the placebo response and making it much harder to prove that new drugs actually work 230.
This challenge is most pronounced in psychiatry and neurology. In extensive meta-analyses of psychiatric trials, placebo treatments yield massive, clinically meaningful improvements in conditions like Major Depressive Disorder (MDD) and Generalized Anxiety Disorder (GAD) 830. Often, over half of the symptom improvement seen in antidepressant trials is driven entirely by the placebo effect 2530. Interestingly, the magnitude of the placebo response varies by the pathology of the illness; while it is exceedingly high in depression and anxiety, it remains much lower and more modest in trials for schizophrenia and Obsessive-Compulsive Disorder (OCD) 3028.
Geographic and Socioeconomic Influences
The context of care heavily influences trial outcomes globally. Recent large-scale analyses of clinical trials for conditions like Rheumatoid Arthritis, Psoriatic Arthritis, and Crohn's disease have uncovered a startling geographic gradient 2729.
Researchers found that in trials conducted in countries with a lower Gross National Income (GNI) or Human Development Index (HDI), the placebo response rates are significantly higher than in wealthier nations 27. This is theorized to be because trial participants in lower-resource settings receive a level of intensive, empathetic medical attention and frequent monitoring during the trial that vastly exceeds the standard background care available in their region. This dramatic upgrade in the context of care serves as a massive psychological expectation boost, inflating the placebo response and complicating the global evaluation of biologic drugs 27.
The Objective Limits of Placebo Healing
Despite its profound reach, the placebo effect is not magic, and it operates within strict biological boundaries. Placebos primarily influence symptom perception rather than fundamentally altering the underlying pathophysiology of a severe disease 2730.
Placebos are exceptionally effective for conditions mediated by the central nervous system's interpretation of bodily signals. This makes them powerful tools for alleviating pain, chronic fatigue, mild-to-moderate depression, nausea, irritable bowel syndrome, and subjective stiffness 82630.
For example, in a recent, rigorous trial treating patients suffering from severe Long COVID fatigue, a sham group receiving a placebo hyperbaric oxygen treatment (HBOT) showed massive, statistically significant improvements in health-related quality of life, energy levels, and social functioning, simply due to the intense ritual of entering a hyperbaric chamber 303132.
However, placebos cannot alter objective, non-neurological disease states. A placebo response cannot shrink a cancerous tumor, cure a bacterial infection, clear the COVID-19 virus from the lungs, reverse Alzheimer's plaques, or knit a broken bone back together 230. In trials for asthma, a placebo inhaler can make a patient subjectively feel that they are breathing much easier, relieving their panic and distress, but objective spirometry tests will show that their lung airways remain physically restricted 28.
| Medical Condition | Placebo Response Magnitude in Clinical Trials | Primary Impact Domain |
|---|---|---|
| Major Depressive Disorder (MDD) | Very High (Often >50% of drug efficacy) | Subjective mood, motivation, energy 82530 |
| Pain Syndromes (e.g., Osteoarthritis) | High (Consistent and robust) | Subjective pain intensity, mobility 82226 |
| Long COVID (Fatigue & Brain Fog) | High (Major quality of life improvements) | Subjective energy, cognitive clarity 3032 |
| Crohn's Disease | Moderate (approx. 18-33% clinical remission) | Subjective cramping, but rarely mucosal healing 2733 |
| Schizophrenia / OCD | Low | Limited impact on deep neurological pathology 3028 |
| Cancer / Bacterial Infections | Zero | No impact on objective tumor shrinkage or bacterial clearance 2 |
The Rise of Open-Label Placebos
Historically, the medical establishment believed that deception was strictly necessary for a placebo to work. The assumption was simple: if a patient knew the pill was a dummy, their expectation of healing would vanish, and the biological effect would break 23. This belief severely limited the clinical use of placebos, as lying to patients violates modern medical ethics.
Healing Without Deception
However, over the last decade, pioneering research into "Open-Label Placebos" (OLPs) has completely shattered this assumption. In an OLP trial, doctors hand patients a bottle of pills and explicitly say, "These are placebo pills made of inert substances like sugar. They contain no medicine. However, clinical studies show they can still produce significant relief through mind-body healing processes" 23.
Astonishingly, patients taking open-label placebos continue to experience significant, measurable symptom reductions. Meta-analyses of numerous randomized controlled trials (RCTs) confirm that OLPs yield positive effects across a variety of health-related outcomes, demonstrating profound efficacy in treating Irritable Bowel Syndrome (IBS), chronic lower back pain, migraine, allergic rhinitis, and depression 2826.
The Bayesian Brain and Embodied Cognition
How is it possible that the body heals itself when the conscious mind knows the treatment is fake? Neuroscientists and psychologists point to the concepts of the "Bayesian brain" and embodied cognition 2.
The brain acts as a Bayesian inference engine, constantly predicting sensory inputs based on past experiences. The mere physical act of engaging in a medical ritual - taking the time to swallow a pill twice a day, interacting with an empathetic healthcare provider, and stepping into the structured environment of a clinic - sends an enormous, unconscious signal of safety to the nervous system 12.
This ritual generates a "prediction error" that updates the brain's internal model from "I am in danger and sick" to "I am actively being cared for" 12. It grants the nervous system permission to stop sounding the biological alarm of chronic pain, nausea, or anxiety, successfully triggering the release of endorphins and dopamine regardless of the patient's conscious, intellectual skepticism about the sugar pill 1.
Bottom line
The placebo response is a genuine, measurable biological process where the brain translates the expectation of healing into physical reality. By triggering the release of endogenous opioids, dopamine, and serotonin, and by routing signals through specialized neural pathways like the cortico-ponto-cerebellar circuit, placebos can profoundly reduce pain, improve motor function, and ease psychological distress. While the effect is heavily constrained by an individual's genetics (the placebome) and cannot cure objective pathologies like cancer or infections, it provides undeniable proof that the context of medical care - trust, ritual, and communication - is a vital, active catalyst for human health.