What's Next After Ozempic? New Obesity Drugs for 2026
The era of single-hormone weight loss injections is ending, making way for highly potent multi-receptor drugs and unrestricted daily pills. At the 2026 American Diabetes Association Scientific Sessions, researchers revealed that triple-agonist injections like retatrutide can drive up to 30% weight loss, rivaling bariatric surgery. Meanwhile, the newly FDA-approved oral pill Foundayo eliminates the strict fasting rules of older medications, drastically expanding real-world access for millions of patients.
The Shifting Landscape of Obesity Medicine
For the last several years, glucagon-like peptide-1 (GLP-1) receptor agonists like semaglutide (Ozempic, Wegovy) and the dual-agonist tirzepatide (Mounjaro, Zepbound) have dominated the medical landscape and public consciousness. However, as thousands of endocrinologists, researchers, and pharmaceutical executives gather in New Orleans from June 5 to June 8 for the 85th annual ADA Scientific Sessions, the conversation has officially moved past this first wave of treatments 123.
Medical science increasingly understands obesity not as a failure of willpower, but as a complex, chronic neurometabolic disease 24. Successfully treating it requires pharmacological interventions that target multiple biological pathways simultaneously. When we eat, the human gut releases a symphony of peptides - often referred to as nutrient-stimulated hormones (NuSH) or incretins - that regulate satiety, insulin production, and our resting metabolic rate 56.
The ADA 2026 program highlights a clear divide in how the pharmaceutical industry plans to harness these hormones moving forward. Developers are pursuing two distinct strategies. The first involves poly-agonists (dual and triple agonists) that activate two or three different hormone receptors at once to achieve profound, synergistic weight loss 78. The second strategy focuses on small-molecule oral pills, which survive the human digestive tract to offer the efficacy of an injection in a highly accessible daily tablet 910.
Understanding Nutrient-Stimulated Hormones
To fully grasp the significance of the drugs debuting at ADA 2026, it is helpful to understand the distinct roles of the four primary hormones targeted by next-generation therapeutics:
| Hormone Target | Primary Origin | Core Metabolic Function | Next-Generation Drugs Targeting This |
|---|---|---|---|
| GLP-1 | Intestines | Increases insulin secretion, slows gastric emptying, and signals the brain to suppress appetite 56. | Retatrutide, CagriSema, Survodutide, Foundayo |
| GIP | Intestines | Increases meal-stimulated insulin, facilitates fat breakdown (lipolysis), and regulates fat storage 56. | Retatrutide |
| Glucagon | Pancreas | Increases hepatic glucose output, prevents low blood sugar, and promotes significant energy expenditure 567. | Retatrutide, Survodutide |
| Amylin | Pancreas | Co-secreted with insulin; acts on the brainstem to induce profound satiety and delays gastric emptying 910. | CagriSema |
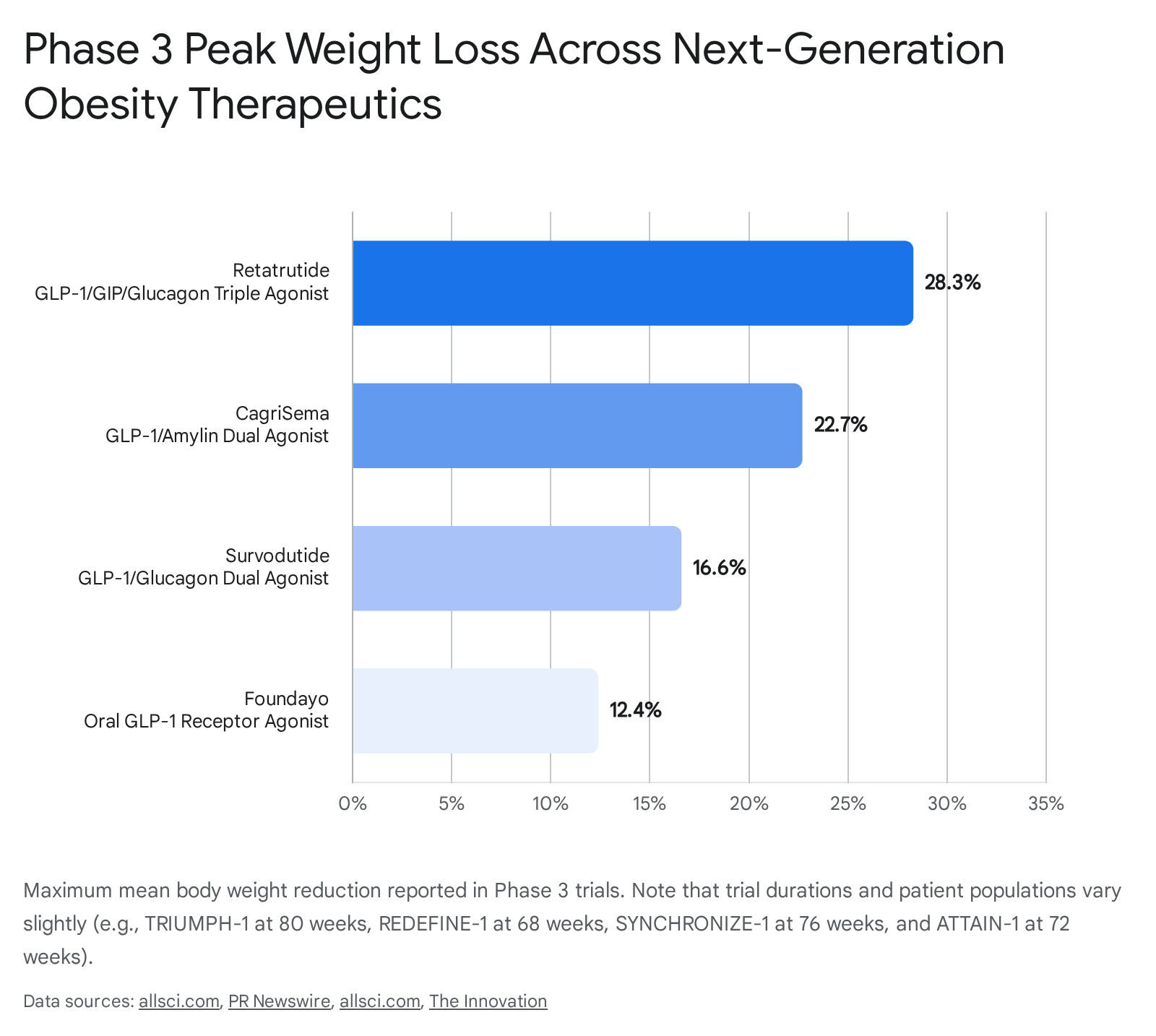
As illustrated in the visual below, combining these hormone targets has allowed researchers to push the boundaries of what non-surgical weight loss can achieve.
Retatrutide: The "Triple-G" Agonist Pushing 30% Weight Loss
The most anticipated clinical data of 2026 belongs to Eli Lilly's investigational drug, retatrutide. Dubbed a "Triple-G" agonist, retatrutide is a single synthetic peptide engineered to activate the GLP-1, GIP, and glucagon receptors concurrently 513.
Historically, adding a glucagon agonist to an obesity drug was viewed with caution because glucagon naturally raises blood sugar levels 5. However, metabolic researchers discovered that when paired with the powerful insulin-boosting effects of GLP-1 and GIP, these glycemic risks are effectively neutralized. What remains is glucagon's unique ability to significantly increase the body's resting metabolic rate and burn fat directly from the liver 67.
The TRIUMPH-1 Phase 3 Results
In late May 2026, Eli Lilly released the long-awaited topline results from TRIUMPH-1, a flagship Phase 3 trial involving 2,339 adults with obesity or overweight without diabetes 1112. The results redefine what is possible with pharmacotherapy.
At 80 weeks, participants taking the highest dose (12 mg injected weekly) lost an average of 28.3% of their body weight, equating to roughly 70.3 pounds 4. Even more remarkably, a pre-specified extension of the trial followed a subset of patients with severe obesity (a baseline BMI of 35 or higher) out to 104 weeks. Those patients saw their weight loss continue without plateauing, reaching an astonishing average loss of 30.3% (85 pounds) 4.
To put this into medical context, 30% weight loss is the historical threshold associated with invasive bariatric surgery 411. In the TRIUMPH-1 trial, 45.3% of all participants on the 12 mg dose achieved this surgical-level weight loss 4. Furthermore, nearly two-thirds of patients (65.3%) on the highest dose fell entirely below the BMI threshold for obesity by week 80, transitioning to a normal or simply overweight classification 412.
Beyond the Scale: Joint Pain, Diabetes, and Liver Fat
While extreme weight loss captures headlines, retatrutide's broader health impacts were a major focus at the ADA sessions. In the related Phase 3 TRIUMPH-4 trial, which specifically enrolled patients suffering from obesity and knee osteoarthritis, the 12 mg dose drove a 28.7% weight reduction over 68 weeks 1311. This massive weight offloading translated to a 75.8% reduction in patient-reported joint pain 13.
The drug also demonstrated profound cardiovascular and metabolic benefits. Across the TRIUMPH program, researchers noted an approximate 20% drop in LDL "bad" cholesterol, likely driven by glucagon-receptor activity 13. In a population of patients with prediabetes, 72% reverted to normal blood glucose levels 13. Furthermore, in the TRANSCEND-T2D-1 Phase 3 trial targeting adults with established type 2 diabetes - a group historically resistant to pharmacological weight loss - patients lost 16.8% of their body weight at 40 weeks and saw their HbA1c drop by up to 2.0% 11.
Earlier Phase 2 liver sub-studies provided clues to how retatrutide achieves these metabolic resets, showing that the 12 mg dose can reduce liver fat by an incredible 86% within 48 weeks, returning 93% of participants to normal liver fat levels 17.
The Dysesthesia Side Effect
With unprecedented efficacy comes necessary biological scrutiny. Retatrutide shares the common gastrointestinal side effects typical of the GLP-1 class - nausea, diarrhea, constipation, and vomiting, which typically peak during dose escalation steps 41819. However, Phase 3 trials have firmly established a novel safety signal not seen with Ozempic or Zepbound: dysesthesia 1820.
Dysesthesia is a neurological condition characterized by abnormal skin sensations. Patients often describe it as a tingling, crawling, prickling, or hyper-sensitive burning feeling on the skin 182021.
- In the Phase 3 TRIUMPH-4 trial, dysesthesia occurred in 20.9% of participants on the 12 mg dose, and 8.8% on the 9 mg dose 1820.
- In the broader TRIUMPH-1 trial, the incidence was slightly lower but still notable, occurring in 12.5% of patients on the 12 mg dose, compared to just 0.9% of those on a placebo 412.
Researchers currently hypothesize that this tingling is linked directly to the drug's glucagon receptor activity, which may affect peripheral nerve signaling 1820. Fortunately, trial data indicates that the events were generally mild to moderate, mostly resolving over time, and rarely caused patients to abandon the treatment 418.
Additionally, retatrutide caused a dose-dependent increase in resting heart rate of roughly 5 to 10 beats per minute, which tends to peak around week 24 before declining 1819. This chronotropic effect is under careful observation in the ongoing TRIUMPH-3 cardiovascular outcomes trial 2013.
Regulatory Timeline and Expected Availability
Despite the flood of successful Phase 3 data, retatrutide is an investigational drug. It is not approved by the FDA, the European Medicines Agency (EMA), or the UK's MHRA 1317. Due to massive public interest, unregulated copies are being sold online for "research purposes," prompting warnings from obesity medicine specialists regarding the dangers of using such potent medications without strict medical supervision 13.
Eli Lilly is expected to compile the safety and efficacy data from the core TRIUMPH trials and submit a New Drug Application (NDA) to the FDA in late 2026 (likely Q4) 1714. Because drug approval is a multi-stage process requiring extensive review of manufacturing logistics and safety data, the standard 10-month FDA review timeline places actual commercial availability in late 2027 or the first half of 2028 1425.
CagriSema: Pairing GLP-1 With Amylin
While Eli Lilly pursues the triple-agonist strategy, Novo Nordisk - the pioneer behind Wegovy - has placed its future obesity bets on a different combination therapy: CagriSema.
CagriSema is a fixed-dose, once-weekly injection that combines semaglutide (a GLP-1 agonist) with cagrilintide, a long-acting analog of the hormone amylin 19. Like insulin, amylin is naturally secreted by the pancreas. While GLP-1 primarily handles blood sugar regulation and slows digestion, amylin works directly on distinct pathways in the brainstem to induce a profound sense of fullness and satiety 910. By pairing the two, Novo Nordisk aims to create an additive, synergistic "semaglutide squared" effect 1015.
REDEFINE Trial Results and Market Expectations
At the ADA 2026 symposium, the medical community gained its deepest look yet at the REDEFINE 1 and REDEFINE 2 Phase 3 trials.
In REDEFINE 1, led by Dr. W. Timothy Garvey, researchers randomized 3,417 adults with overweight or obesity (without diabetes) to receive either CagriSema, semaglutide alone, cagrilintide alone, or a placebo 101516. The results demonstrated that CagriSema delivered a mean body weight reduction of 22.7% at 68 weeks for patients who adhered to the treatment plan, compared to 16.1% for semaglutide alone and just 2.3% for the placebo group 101617. In absolute terms, patients lost an average of 21.6 kg (about 47.6 lbs) 1015.
Scientifically, proving that CagriSema is vastly superior to semaglutide monotherapy was a massive clinical success. Financially, however, the pharmaceutical market reacted harshly. When the topline data was initially announced, Novo Nordisk's stock plunged 17%, erasing roughly $60 billion from the company's valuation 17.
This massive sell-off occurred because Wall Street analysts had priced in a "near unanimous expectation" that CagriSema would drive 25% or more absolute weight loss, definitively beating Eli Lilly's Zepbound (tirzepatide) 17. Instead, a 22.7% weight loss puts CagriSema essentially on par with Zepbound, leaving Novo Nordisk with a highly effective drug, but a more complicated market positioning battle against its primary rival 1729.
Managing Gastrointestinal Tolerability
A major question surrounding combination therapies is whether stacking multiple drugs increases side effects. In the REDEFINE 1 trial, gastrointestinal adverse events occurred in roughly 80% of the CagriSema group, primarily manifesting as nausea (55%), diarrhea, and constipation 1015.
However, a recent Bayesian network meta-analysis presented to the scientific community highlighted a distinct advantage for the drug. The analysis found that across all efficacy endpoints, CagriSema ranked first compared to its individual components. Crucially, it also ranked best for overall gastrointestinal tolerability, including nausea, vomiting, and adverse events leading to treatment discontinuation 18. This suggests that stimulating two complementary satiety pathways simultaneously might actually be better tolerated than pushing a single pathway (like GLP-1 alone) to its absolute maximum limit 2918.
CagriSema also proved highly effective for patients with type 2 diabetes. In the REDEFINE 2 trial, patients lost an average of 15.7% of their body weight and saw a mean HbA1c reduction of 2.3 percentage points, significantly outperforming individual monotherapies in achieving glycemic targets 1031. These diabetes-specific outcomes are the focus of the REIMAGINE 1, 2, and 3 trials, featured prominently in dedicated ADA 2026 symposiums 9.
Survodutide: A Dual-Agonist With a Liver Focus
Not to be outdone by the duopoly of Eli Lilly and Novo Nordisk, Boehringer Ingelheim, in partnership with Zealand Pharma, is advancing its own heavy-hitting compound: survodutide.
Survodutide is a dual agonist that activates both the GLP-1 and glucagon receptors 1920. In late April 2026, the company announced positive Phase 3 results from the global SYNCHRONIZE-1 trial. The study was highly diverse, enrolling 725 adults living with obesity or overweight (without diabetes) across 14 countries - with 47.3% from North America, 21.0% from Europe, and 20.0% from East Asia 192122.
The SYNCHRONIZE-1 Efficacy Data
Participants treated with weekly subcutaneous injections of survodutide experienced an average sustained weight loss of 16.6% over 76 weeks, a statistically significant decrease versus the 3.2% loss seen in the placebo arm 2022. Impressively, up to 85.1% of adults treated with survodutide achieved a clinically meaningful body weight reduction of at least 5% 20. Initial body composition analyses indicate that this weight reduction was driven predominantly by the loss of fat tissue, effectively preserving lean muscle mass 20.
Targeting MASH and Visceral Fat
While 16.6% weight loss does not reach the towering statistical heights of retatrutide or CagriSema, survodutide is carving out a vital, specific niche in metabolic medicine. The addition of glucagon agonism makes the drug highly effective at mobilizing visceral fat and lipid deposits directly from the liver 2021.
Excess visceral fat is a primary contributor to metabolic dysfunction and impaired liver function 20. In earlier Phase 2 studies, survodutide demonstrated the ability to reduce liver fat by up to 86% in just 48 weeks 17. Consequently, Boehringer Ingelheim is heavily evaluating survodutide in the parallel LIVERAGE trials for patients suffering from metabolic dysfunction-associated steatohepatitis (MASH) and moderate to advanced liver fibrosis 20. If ultimately approved, survodutide may become the preferred, specialized treatment for obese patients whose primary comorbidity is advanced liver disease.
Foundayo (Orforglipron): The Unrestricted Oral Pill Revolution
While injectable drugs chase maximum weight loss percentages, an entirely different revolution in obesity care was realized on April 1, 2026, when the FDA officially approved Eli Lilly's Foundayo (orforglipron) for chronic weight management 1023.
Overcoming the Peptide Problem
Until the approval of Foundayo, effectively delivering a GLP-1 drug into the bloodstream required a subcutaneous injection 9. The only previous exception on the market was Novo Nordisk's oral semaglutide (sold as Rybelsus for diabetes and oral Wegovy for obesity) 1024. Because semaglutide is a peptide - a small protein chain - it is rapidly destroyed by harsh stomach acid and digestive enzymes 9.
To make the semaglutide pill work, it relies on absorption-enhancing formulations. Patients must take it on a strictly empty stomach upon waking, swallow it with no more than 4 ounces of water, and wait exactly 30 minutes before eating, drinking, or taking any other medications 910. Even with these strict rules, absorption remains highly variable from patient to patient.
Foundayo solves this biological hurdle entirely. It is the first non-peptide, small-molecule GLP-1 receptor agonist approved for weight loss 310. Because it is chemically stable in acidic environments, it does not require complex absorption enhancers 9. Patients can take the Foundayo tablet at any time of day, with or without food, and with no water restrictions 31038.
ATTAIN and ACHIEVE Efficacy Data
Foundayo trades the extreme weight loss seen in next-generation injectables for unparalleled real-world convenience. The FDA approval was supported by the massive ATTAIN clinical trial program.
In the ATTAIN-1 trial, which enrolled over 3,100 adults with obesity or overweight, participants taking the highest dose of Foundayo (17.2 mg daily) lost an average of 12.4% of their body weight (roughly 27.3 pounds) at 72 weeks, compared to just 0.9% with a placebo 102338. The drug also proved highly effective across diverse age and demographic groups. Post-hoc analyses presented at recent conferences demonstrated a 13% body weight reduction in adults aged 65 and older, and over 14% weight reduction in women experiencing peri-menopause or post-menopause 324.
For patients with type 2 diabetes, Foundayo's efficacy was evaluated in the ACHIEVE-3 head-to-head trial against oral semaglutide. Foundayo won decisively on both primary endpoints, dropping HbA1c by 2.2% (versus 1.4% with semaglutide) and driving 9.2% weight loss (versus 5.3% for the semaglutide pill) over 52 weeks 3938.
| Feature | Foundayo (Orforglipron) | Oral Wegovy (Semaglutide) |
|---|---|---|
| Molecule Type | Small Molecule (Non-peptide) 10 | Peptide 910 |
| Administration Rules | Any time, with or without food/water 31025 | Empty stomach, sip of water, 30-min wait 910 |
| Trial Weight Loss | 12.4% at 72 weeks (ATTAIN-1) 2338 | ~13.6% - 16.6% (OASIS trials) 2641 |
| FDA Status | Approved April 2026 1023 | Approved December 2025 1024 |
Step-by-Step Dosing and Side Effects
Like all GLP-1 medications, Foundayo's primary side effects are gastrointestinal. The most commonly reported adverse reactions include nausea, stomach pain, heartburn, constipation, diarrhea, and vomiting 272829.
To mitigate these issues, Foundayo utilizes a deliberately slow, six-month dose escalation schedule. Patients start at 0.8 mg daily for a month, slowly stepping up through 2.5 mg, 5.5 mg, 9 mg, and 14.5 mg, before eventually reaching the target maintenance dose of 17.2 mg 382829. Trial data consistently shows that patients who rush this escalation experience far more nausea, while those who adhere to the monthly steps tolerate the drug much better 1838.
Foundayo also carries standard FDA boxed warnings for the class, specifically regarding a potential increased risk of thyroid C-cell tumors based on preclinical rodent studies 2729. It is contraindicated for patients with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 2930.
Patient Access, Costs, and Real-World Impact
The most impressive clinical trial results in the world mean little if patients cannot afford the medication. The ADA 2026 sessions are deeply focused on patient-centric care, optimizing outcomes, and expanding affordability 231.
Expanding Insurance Coverage
Historically, high price tags and strict insurance hurdles have kept GLP-1 therapies out of reach for many. In the UK, Eli Lilly recently implemented wholesale price increases for Mounjaro, prompting some patients and telehealth providers to switch to Wegovy for better cost-efficiency 32.
However, in the United States, patient access is undergoing a rapid, massive expansion. By June 1, 2026, CVS Caremark - one of the largest pharmacy benefit managers (PBMs) in the country, controlling access for tens of millions of Americans - will add the newly approved Foundayo pill to its commercial formularies 254833. This will be followed by the reinstatement of Zepbound coverage by October 1 4833. With this announcement, Lilly's obesity portfolio is now covered by all three major national PBMs 25.
For eligible patients with commercial insurance, these medications can now cost as little as $25 a month out-of-pocket 254834. Furthermore, a new Medicare GLP-1 Bridge program launching on July 1, 2026, will allow eligible Medicare Part D beneficiaries to access the drugs for a capped cost of $50 a month, marking a paradigm shift in public health accessibility for older populations 254834.
Weighing Rare Risks and Benefits
As millions of Americans gain access to these drugs, researchers are tracking long-term, rare safety signals. Recent large-scale observational studies have pointed to a slight, albeit rare, increased risk of ocular complications associated with semaglutide use.
One study found that patients taking semaglutide had an estimated 1.3 times higher risk of developing a rare condition called nonarteritic anterior ischemic optic neuropathy (NAION) compared to those not taking the drug 35. Another study noted a slightly elevated risk of wet age-related macular degeneration (AMD) in patients over 65 35. However, the absolute risk remains exceptionally low - NAION affects roughly 10 in 100,000 people annually 35. Medical experts emphasize that patients must balance these rare, potential side effects against the guaranteed, severe, and compounding long-term health risks of living with untreated cardiovascular disease, type 2 diabetes, and severe obesity 35.
Bottom line
The ADA 2026 Scientific Sessions highlight a profound evolution in metabolic medicine. Poly-agonists like retatrutide are pushing boundaries by achieving nearly 30% body weight loss, effectively rivaling bariatric surgery, while oral innovations like Foundayo are dismantling the adherence barriers of injectables and fasting restrictions. However, the emergence of novel side effects like dysesthesia, alongside ongoing insurance and pricing battles, ensures that while the basic science of obesity is rapidly advancing, the complex logistics of treating the global epidemic are only just beginning.