How Semaglutide, Tirzepatide, and Retatrutide Compare
In 2026, the obesity treatment landscape is led by single-agonist semaglutide and dual-agonist tirzepatide, which offer up to 21% and 22% weight loss, respectively, and are now widely available following the resolution of global shortages. Meanwhile, the experimental triple-agonist retatrutide delivers an unprecedented 30% weight reduction but remains unapproved until at least 2027 and carries unique nerve-related side effects. The data firmly establishes that these medications require lifelong adherence to maintain metabolic benefits, as cessation results in rapid weight regain.
The Paradigm Shift in Obesity Pharmacotherapy
The conversation surrounding obesity management has shifted permanently from one of behavioral morality to one of chronic metabolic disease management. Just a few years ago, the medical community celebrated the arrival of a single drug capable of producing a 15% body weight reduction. Today, the pharmaceutical landscape has transitioned from a period of severe, chronic drug shortages into an era of unprecedented choice, fierce competition, and sophisticated multi-receptor targeting 12.
The question for patients and clinicians is no longer whether these drugs work, but rather which specific molecular approach is best suited to a patient's unique metabolic profile, cardiovascular risk, and tolerance for side effects 3. As the global obesity medicine market rockets toward a projected $92 billion valuation by the end of 2026, clinical guidelines are evolving 2. Leading medical bodies, such as the American Association of Clinical Endocrinology, have introduced the Adiposity-Based Chronic Disease (ABCD) model, replacing outdated BMI-centric classifications with staging systems based on obesity-related complications 1.
At the heart of this revolution are incretin mimetics - synthetic versions of hormones naturally produced in the gut that regulate blood sugar, digestion, and appetite. The rapid evolution of these medications has moved from "single agonists" (targeting one hormone receptor) to "dual agonists" (targeting two), and now to "triple agonists" (targeting three) 5. In 2026 alone, we have seen the approval of the first daily oral non-peptide pills, the release of long-term extension data on muscle mass preservation, and head-to-head trials directly comparing the heaviest hitters in the industry 374. Understanding the nuances of semaglutide, tirzepatide, and retatrutide requires looking past the brand names and examining the rigorous, peer-reviewed data defining their efficacy, safety, and real-world accessibility.
Mechanisms of Action: Single, Dual, and Triple Agonists
To understand why these three medications yield different clinical outcomes, it is essential to understand how they interact with the body's endocrine system. These drugs are essentially chemical keys designed to fit into specific cellular locks (receptors) in the pancreas, gut, liver, and brain.
The Single Agonist: GLP-1 (Semaglutide)
Semaglutide, marketed as Wegovy for obesity and Ozempic for Type 2 diabetes, is a single-receptor agonist 5. It mimics Glucagon-Like Peptide-1 (GLP-1), a hormone natively produced in the intestines. When a person eats, the gut naturally releases GLP-1, which prompts the pancreas to secrete insulin, lowers glucagon secretion (which stops the liver from releasing stored sugar), and drastically slows gastric emptying 611.
More importantly for weight loss, GLP-1 crosses the blood-brain barrier and binds to receptors in the hypothalamus, signaling profound satiety. The brain is tricked into feeling full, naturally driving down caloric intake and suppressing "food noise" 6. While highly effective, hitting a single receptor eventually leads to a physiological plateau as the body's metabolic adaptations attempt to halt further weight loss.
The Dual Agonist: GLP-1 + GIP (Tirzepatide)
Tirzepatide, known as Zepbound for obesity and Mounjaro for diabetes, takes the GLP-1 foundation and adds a second key: Glucose-Dependent Insulinotropic Polypeptide (GIP) 512. Originally, scientists were highly skeptical of GIP, as early data suggested it might actually be an obesogen (promoting fat storage). However, clinical application revealed that combining GIP with GLP-1 produces a powerful synergistic effect.
GIP enhances insulin secretion specifically when blood sugar is high and directly modulates how the brain processes fullness signals, reducing the nausea often associated with GLP-1 monotherapy 12. Furthermore, GIP receptor activation appears to improve how the body stores and utilizes fat. It promotes healthy subcutaneous lipid storage while reducing ectopic fat - the dangerous visceral fat stored in organs like the liver and pancreas. This synergistic dual-action approach is precisely why tirzepatide generally outpaces semaglutide in weight loss metrics 13.
The Triple Agonist: GLP-1 + GIP + Glucagon (Retatrutide)
Retatrutide represents the bleeding edge of this pharmacological arms race. Currently in Phase 3 clinical development by Eli Lilly, the compound acts on three distinct metabolic receptors: GLP-1, GIP, and Glucagon 57.
The addition of the glucagon receptor is the true paradigm-shifter. Historically, glucagon was viewed solely as the counter-regulatory hormone to insulin - raising blood sugar when levels dropped too low. However, at therapeutic doses combined with GLP-1 and GIP, glucagon receptor activation drastically increases energy expenditure. It stimulates the liver to burn stored fat (lipolysis) and increases the body's basal metabolic rate 58.
By simultaneously shutting down energy intake (appetite suppression via GLP-1/GIP) and revving up energy output (fat burning via glucagon), retatrutide mimics the physiological effects of aggressive cardiovascular exercise and fasting. This dual-pronged attack on energy balance leads to weight loss figures previously thought impossible without bariatric surgery 89.
The 2026 Head-to-Head Clinical Data
To synthesize the clinical trial data from 2025 and 2026, the following table benchmarks the three primary competitors based on their highest tested doses in obesity-specific clinical trials.
| Metric | Semaglutide (High Dose) | Tirzepatide | Retatrutide |
|---|---|---|---|
| Mechanism | Single (GLP-1) | Dual (GLP-1 / GIP) | Triple (GLP-1 / GIP / Glucagon) |
| Brand Names | Wegovy, Ozempic | Zepbound, Mounjaro | N/A (Investigational: LY3437943) |
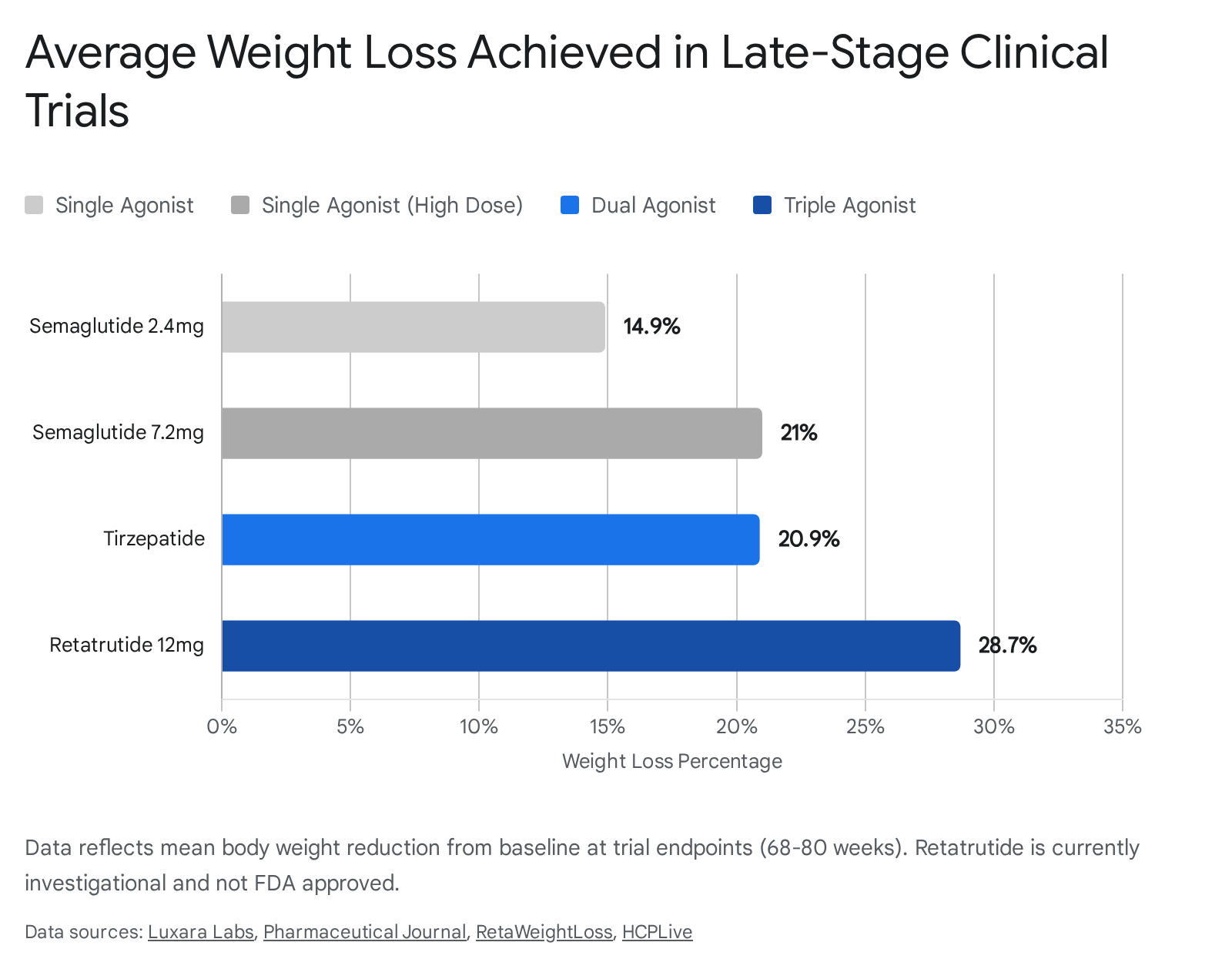
| Average Weight Loss | 20.7% - 21.0% (7.2mg) | 20.9% - 22.0% (15mg) | 28.3% - 30.3% (12mg) |
| Percentage Losing >25% | 33.2% | 31.6% | ~45% (achieved >30% loss) |
| FDA Approval Status | Approved (Label update pending) | Approved (2023) | Investigational (Expected 2027/2028) |
| Discontinuation Rate | 3.3% - 8.0% | 6.1% - 14.9% | 11.3% - 18.2% |
| Notable Unique Risk | Rare pancreatitis risk | Gallbladder events | Dysesthesia (nerve pain/tingling) |
(Data compiled from STEP-UP, SURMOUNT-1, SURMOUNT-5, and TRIUMPH-1/TRIUMPH-4 late-stage clinical trials) 5131011121321.
Semaglutide: Pushing the Ceiling with STEP-UP
Semaglutide, manufactured by Novo Nordisk, was the catalyst for the current obesity drug revolution. For years, the 2.4 mg weekly injection (Wegovy) served as the gold standard, producing an average weight loss of around 15% to 17% over 68 weeks 622.
However, as competitors entered the market with superior efficacy numbers, Novo Nordisk initiated the STEP-UP Phase 3b trial to explore whether pushing the dosage higher could close the competitive gap. The headline results, presented at the American Diabetes Association (ADA) Scientific Sessions in 2025, validated this approach. In the trial involving 1,407 adults with obesity, patients utilizing a massive 7.2 mg weekly dose of semaglutide achieved a mean weight reduction of 20.7% to 21.0% over 72 weeks 132114. Remarkably, 33.2% of the participants on the 7.2 mg dose lost 25% or more of their body weight, pushing semaglutide's efficacy ceiling firmly into tirzepatide territory 1315.
Despite the tripled dosage, Novo Nordisk reported that the safety and tolerability profile remained manageable. Discontinuation rates due to gastrointestinal events sat at just 3.3% for the 7.2 mg dose, compared to 2.0% for the 2.4 mg dose 16. Based on these robust results, Novo Nordisk is pursuing regulatory label updates globally in 2026 13.
Beyond sheer weight loss, semaglutide maintains a distinct, proven advantage in cardiovascular and renal outcome data. The historic SELECT trial demonstrated that long-term semaglutide use reduces the risk of major adverse cardiovascular events (MACE) by 20% in patients with existing heart disease 1517. Consequently, the European Association for the Study of Obesity (EASO) 2025 guidelines explicitly recommend semaglutide as a first-line treatment for individuals living with obesity accompanied by cardiovascular disease 18. Furthermore, semaglutide recently secured FDA and EMA approvals for chronic kidney disease, solidifying its status as a foundational whole-body therapy 1.
Tirzepatide: The Current Efficacy and Tolerability Champion
If semaglutide broke the dam, tirzepatide flooded the valley. By activating both GLP-1 and GIP receptors, tirzepatide consistently outperforms baseline 2.4mg semaglutide in real-world clinical settings.
Any lingering debate over which approved medication is more potent at standard doses was decisively settled by the SURMOUNT-5 trial. Published in 2025, this open-label, head-to-head study directly compared tirzepatide 15 mg against semaglutide 2.4 mg over 72 weeks 313. The results were stark: tirzepatide produced a mean weight loss of 20.2% (an average of 50 pounds), compared to 13.7% (an average of 33 pounds) for semaglutide 3. Furthermore, 31.6% of participants on tirzepatide lost at least a quarter of their body weight, almost double the 16.1% rate seen in the semaglutide cohort 13.
Efficacy aside, tirzepatide also benefits from a highly favorable tolerability profile. While all incretin medications cause gastrointestinal distress (nausea, vomiting, diarrhea) during dose escalation, network meta-analyses show tirzepatide consistently reports lower rates of severe nausea and lower overall discontinuation rates compared to older single-agonists 519. For instance, discontinuation due to adverse effects sits at roughly 6.1% to 14.9% for tirzepatide, making it highly tolerable for long-term adherence 512.
Like semaglutide, tirzepatide is rapidly expanding its label indications. In 2025, it gained FDA approval for the treatment of obstructive sleep apnea, reflecting the profound mechanical and metabolic benefits of reducing airway adiposity 1. For patients accessing care in 2026, clinical consensus generally points to tirzepatide as the superior available option for comprehensive weight loss and general tolerability, assuming insurance coverage allows for equal access 512.
Retatrutide: The Bariatric-Level Future
While tirzepatide rules the present, retatrutide represents the future of obesity medicine. Eli Lilly's investigational triple agonist has generated shockwaves through the medical community following the publication of its Phase 3 TRIUMPH trial program results.
In December 2025, Eli Lilly released the first Phase 3 readout for retatrutide from the TRIUMPH-4 trial. Evaluating adults with obesity and knee osteoarthritis, the trial reported a staggering 28.7% mean body-weight reduction at 68 weeks on the 12 mg weekly dose - the highest weight-loss signal ever recorded in a randomized Phase 3 trial for a GLP-1 class compound 510. This equated to an average loss of 71.2 pounds per patient, accompanied by a massive 75.8% reduction in osteoarthritis pain scores 510.
These figures were corroborated in May 2026 when Eli Lilly announced topline results from the TRIUMPH-1 trial. At the 80-week mark, participants taking the 12 mg dose averaged a 28.3% reduction. More impressively, when the extension data pushed out to 104 weeks for participants with severe obesity (BMI ≥35), average weight loss reached 30.3%, or an average of 85 pounds 911. Nearly half (45.3%) of the participants achieved at least 30% weight loss, a transformative threshold previously thought to be exclusively the domain of invasive gastric bypass or sleeve gastrectomy surgeries 920.
The addition of the glucagon receptor does more than melt peripheral fat; it actively clears ectopic fat from vital organs. In earlier Phase 2 sub-studies published in Nature Medicine, the 12 mg dose of retatrutide reduced liver fat by an astonishing 86% at 48 weeks, with 93% of participants achieving entirely normal liver fat levels 8. For patients battling Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD), this deep clearance of hepatic fat is revolutionary. The drug also produced a 72% reversal rate from prediabetes to normoglycemia and significantly lowered LDL cholesterol 5.
Approval Timelines for Retatrutide
Despite the overwhelming data, retatrutide is not yet available to the public. As of mid-2026, Eli Lilly is still concluding the remaining arms of the massive seven-part TRIUMPH program, which includes trials for patients with cardiovascular disease (TRIUMPH-3) and sleep apnea (TRIUMPH-6) 530. The company is expected to submit its New Drug Application (NDA) to the FDA in Q4 2026 or early Q1 2027 830. Factoring in standard FDA review timelines, the earliest realistic market launch for retatrutide is late 2027 or early 2028 30.
The Dysesthesia Curveball: Retatrutide's Unique Side Effect
The unprecedented power of triple agonism does not come without biological trade-offs. While retatrutide shares the standard gastrointestinal side effects common to all incretin drugs, it has introduced a novel and somewhat concerning safety signal to the clinical lexicon: dysesthesia 1312.
Dysesthesia is a type of neuropathic sensory distortion where normal touch becomes uncomfortable, painful, or altered. Patients report it as a burning sensation on the skin (akin to a severe sunburn without a heat source), prickling, "pins and needles," or extreme skin sensitivity 3121. It differs distinctly from standard paresthesia (the temporary feeling of a limb "falling asleep") because the sensations are often chronic, uncomfortable, and occur without an appropriate external physical stimulus 21.
In the Phase 3 TRIUMPH trials, dysesthesia emerged as a prominent side effect, affecting between 12.5% and 20.9% of patients taking the highest 12 mg dose of retatrutide 1221. This side effect appears to be strictly dose-dependent and highly specific to retatrutide; it does not occur with any meaningful frequency in patients taking the dual-agonist tirzepatide or lower doses of semaglutide 21.
The exact biological mechanism driving this neurological quirk remains unconfirmed. Pharmacovigilance researchers hypothesize that it is directly linked to the activation of the glucagon receptor, which is heavily expressed on both central and peripheral nerves 12. Other prevailing clinical theories suggest it could be tied to transient shifts in electrolytes and B vitamins resulting from rapid weight loss, an effect on small blood vessels, or sudden changes in the subcutaneous fat tissue that normally insulates peripheral nerve endings 123122.
While Eli Lilly's clinical data indicates that the dysesthesia is "generally mild to moderate" and rarely leads to absolute treatment discontinuation, an incidence rate approaching 20% means that hundreds of thousands of patients could experience highly uncomfortable nerve sensations if the drug reaches mass market adoption 122122. Fortunately, current follow-up data does not suggest that retatrutide causes permanent, irreversible peripheral neuropathy 34.
The Muscle Mass Debate: Separating Fact from Fear
As trial participants drop 20% to 30% of their body weight, a significant scientific debate has dominated obesity medicine: how much of that weight is healthy fat, and how much is critical lean muscle mass?
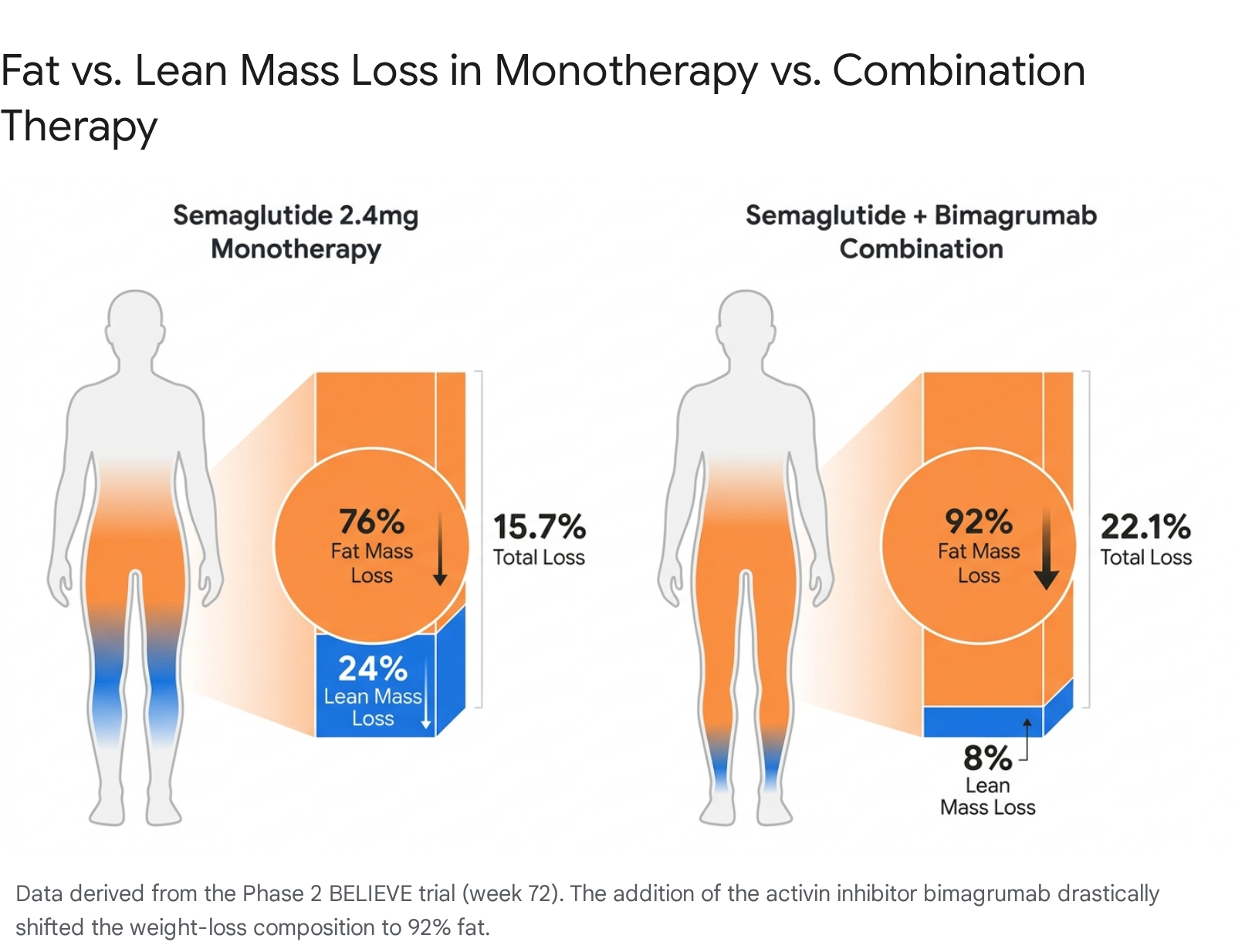
Early Dual-Energy X-ray Absorptiometry (DXA) scan data from the foundational STEP-1 and SURMOUNT-1 trials sparked alarming headlines. Trials showed that up to 40% of the weight lost on semaglutide, and around 25% on tirzepatide, was composed of "lean body mass" 623. Because skeletal muscle naturally declines with age (sarcopenia), geriatricians and metabolic experts feared these highly potent drugs could inadvertently accelerate physical frailty, particularly in elderly populations 624.
However, updated 2026 clinical research has provided a much more nuanced, and highly reassuring, picture. The panic largely stemmed from a misunderstanding of what DXA scans actually measure. "Lean body mass" is a broad umbrella category that includes water weight, bone mineral density, and internal organ weight - not just skeletal muscle 24.
Relative vs. Absolute Muscle Mass
A landmark 2026 pre-clinical and human proof-of-concept study published in Cell Reports Medicine systematically challenged the muscle-wasting narrative. Researchers found that while absolute muscle mass does decrease slightly during GLP-1 therapy (because a lighter body simply requires less muscular infrastructure to carry it around), the relative muscle-to-body-weight ratio actually improves 2425.
Detailed biopsies revealed that the body sheds fat and liver mass at a profoundly faster rate than skeletal muscle 2438. Furthermore, functional tests showed that human patients preserved their handgrip and knee extension strength despite the weight loss, and in animal models, physical running performance and endurance actually improved 2425.
These findings were thoroughly supported by real-world cohort data presented at the 2026 European Congress on Obesity (ECO). Utilizing advanced bioelectrical impedance analysis (BIA) in a study of 486 patients, researchers found that after 14 months of GLP-1 treatment, an overwhelming 80 - 85% of the total weight lost was strictly fat mass 26. Skeletal muscle mass decreased by only 5%, and when statistical modeling accounted for the total drop in fat, relative skeletal muscle mass was completely preserved or increased in more than 70% of the patients 26. The consensus in 2026 is that incretin drugs drive highly favorable body composition changes rather than dangerous, clinically relevant muscle wasting 26.
The Adjuvant Frontier: Muscle-Sparing Combinations
Despite the reassuring functional data, the pharmaceutical industry recognizes that preserving every ounce of muscle is vital, particularly for older adults or those at risk of osteopenia. This has sparked a sub-race to develop "muscle-sparing" adjuvant therapies designed to be paired with GLP-1 drugs 27.
The most prominent of these candidates is bimagrumab, a monoclonal antibody that targets and blocks the activin type II receptor. By inhibiting the myostatin and activin signaling pathways - which normally act as a biological "brake" to limit muscle growth - bimagrumab theoretically allows the body to build or retain muscle even in a steep caloric deficit 2728.
In the Phase 2 BELIEVE trial, published in Nature Medicine in early 2026, researchers tested this theory by combining intravenous bimagrumab (30 mg/kg) with semaglutide (2.4 mg) in 507 adults with obesity 28. The results were spectacular. At 72 weeks, patients on the combination therapy lost 22.1% of their body weight. Crucially, a staggering 92% to 92.8% of that weight loss came exclusively from fat mass, and absolute lean mass actually increased by 2.5% 282930.
The combination therapy also drove a massive 58.2% reduction in visceral adipose tissue 28.
Despite these phenomenal proof-of-concept outcomes, the path forward for combination therapies is highly complex. In late 2025, Eli Lilly unexpectedly terminated a parallel Phase 2 trial of bimagrumab in diabetic patients due to "strategic business reasons," although trials in non-diabetic obese patients remain active with readouts expected later in 2026 3031. The overarching challenge is pharmacoeconomic: adding a second, highly complex biologic infusion to an already expensive injectable GLP-1 regimen creates a massive access hurdle.
For the vast majority of patients in 2026, the most effective, proven strategy to prevent muscle loss while on semaglutide, tirzepatide, or retatrutide remains strictly non-pharmacological. Clinical consensus mandates aggressive dietary protein supplementation (aiming for 1.2 - 1.6g per kg of ideal body weight daily) paired with structured resistance training 2 to 3 times per week to preserve muscle strength and bone density 62332.
The Rebound Reality: What Happens When Treatment Stops?
One of the harshest realities to emerge from the longitudinal data in 2026 is the severe consequence of stopping treatment. Obesity is now widely recognized by endocrinologists as a chronic, relapsing metabolic disease, physiologically akin to hypertension or asthma. If a patient stops taking blood pressure medication, their blood pressure inevitably rises. If a patient stops taking an incretin mimetic, the weight returns.
A definitive 2026 systematic review and meta-analysis published in The BMJ quantified this rebound with sobering clarity. Researchers from the University of Oxford, analyzing 37 studies encompassing over 9,300 adults, found that upon cessation of newer drugs like semaglutide and tirzepatide, weight regains at an aggressive average rate of 0.8 kg (~1.8 pounds) per month 3334. Nonlinear regression modeling from the University of Cambridge estimates that patients regain approximately 60% of their total lost weight within just the first 52 weeks off the drug 35.
At this trajectory, patients are projected to completely return to their baseline pre-treatment weight within 1.5 to 1.7 years of stopping the medication 173334. Alarmingly, the metabolic regain is actually faster than the regain observed when individuals end behavioral diet and exercise programs (rebounding roughly 0.3 kg per month faster) 3334.
This accelerated rebound occurs because the drugs artificially override the body's deeply ingrained homeostatic appetite signals. Once the GLP-1 and GIP receptor agonists are removed from the system, the body's metabolic "set-point" violently reasserts itself. Hunger returns with vengeance, metabolic adaptation slows calorie burn, and patients have not necessarily built the intense behavioral coping strategies required to fight these biological drives naturally 3349.
Furthermore, the hard-won cardiometabolic benefits disappear just as quickly. Trial data shows that improvements in HbA1c, fasting plasma glucose, systolic blood pressure (which drops by an average of 5.8 mm Hg on active treatment), and cholesterol all begin to steadily climb back to dangerous baseline levels in parallel with the weight regain 3334.
The clinical consensus is unequivocal: these medications are not short-term cosmetic "fixes." For sustained cardiometabolic health, patients and healthcare systems must view semaglutide, tirzepatide, and eventually retatrutide as lifelong maintenance therapies 63449.
The End of the Injection Era? The Arrival of Oral GLP-1s
For the millions of patients averse to weekly subcutaneous injections, 2026 brought a long-awaited paradigm shift with the mainstream commercial launch of highly effective oral GLP-1 therapies.
Historically, formulating these drugs as pills has been a biochemical nightmare. Large peptide-based drugs like semaglutide are rapidly destroyed by harsh stomach acids and digestive enzymes, meaning very little survives to be absorbed into the bloodstream. Novo Nordisk partially solved this by combining semaglutide with a chemical absorption enhancer called SNAC, launching the original low-dose Rybelsus. Pushing this further, they developed a high-dose (25 mg and 50 mg) daily Oral Wegovy pill, which received FDA approval in late 2025 and a positive recommendation from the European Medicines Agency (EMA) in May 2026 1136. The 25 mg daily pill produces weight loss comparable to the standard 2.4 mg weekly injection (roughly 15-16%) 11.
However, Oral Wegovy still requires patients to adhere to incredibly strict fasting rules - taking the pill on an empty stomach with a tiny sip of water and waiting a full 30 minutes before consuming any food, beverages, or other medications.
The true pharmaceutical breakthrough in this space is Eli Lilly's orforglipron (marketed under the brand name Foundayo). Approved by the FDA on April 1, 2026, Foundayo is a "small-molecule" non-peptide GLP-1 receptor agonist 43738. Because it is a highly stable small molecule rather than a fragile peptide, it easily survives the digestive tract and absorbs efficiently through the gastric mucosa into the bloodstream 4.
Crucially, this structural difference means Foundayo can be taken at any time of day, with or without food, and with no restrictions on water intake, entirely removing the onerous fasting rules that plague older oral peptides 453.
While it does not match the 20%+ weight loss of injectable dual-agonists like tirzepatide, Phase 3 trials demonstrated that Foundayo is highly effective within the oral class. In the ACHIEVE-3 head-to-head trial published in early 2026, orforglipron 36 mg demonstrated statistically superior weight reduction compared directly to oral semaglutide 14 mg (achieving 8% versus 5% weight loss over 52 weeks in a diabetic cohort) 4.
Foundayo is positioned as an ideal entry-level therapy for needle-phobic patients, or as a convenient, affordable long-term maintenance drug after patients hit their goal weight with heavy-hitting injectables 124. Disrupting the market further, Eli Lilly launched Foundayo at a highly aggressive cash price of $149 per month via their direct-to-consumer platform LillyDirect, significantly undercutting the $1,000+ list prices of traditional injectables and forcing competitors to rethink their pricing models 53.
Market Access, Global Policy, and Medicare in 2026
The scientific brilliance of multi-receptor agonism means nothing if patients cannot physically access or afford the medications. Throughout 2024 and 2025, the industry was plagued by severe global supply chain shortages, leading to a massive, loosely regulated gray market of compounded variants. By mid-2026, Novo Nordisk and Eli Lilly successfully scaled their manufacturing infrastructure; the FDA officially removed semaglutide and tirzepatide from the drug shortage list, paving the way for regulatory agencies to crack down on unauthorized compounding pharmacies 1239.
Simultaneously, insurance coverage underwent a seismic shift in the United States. Following over two decades of statutory bans (stemming from the 2003 Medicare Modernization Act) that prohibited Medicare from covering any drugs explicitly for weight loss, heavy governmental negotiations resulted in a landmark policy change 4041.
Starting July 1, 2026, the Centers for Medicare & Medicaid Services (CMS) launched the "Medicare GLP-1 Bridge" program 4243. Utilizing "most-favored-nation" pricing agreements negotiated with the manufacturers, Medicare secured an astonishing net price of $245 per month for leading medications like Wegovy and Zepbound 3943. Eligible seniors - specifically those with a BMI over 35, or those with a BMI over 30 accompanied by a comorbidity like heart failure, chronic kidney disease, or uncontrolled hypertension - can now access these life-changing therapies for a capped out-of-pocket copay of just $50 a month 4243.
This coverage expansion is projected to radically alter the cardiovascular health trajectory of older Americans. However, the Congressional Budget Office (CBO) estimates that covering GLP-1 drugs for obesity will cost the Medicare program roughly $35 billion between 2026 and 2034, raising ongoing debates about the long-term sustainability of the federal budget 4041. Furthermore, major pharmacy benefit managers (PBMs) like CVS Caremark have updated their commercial formularies to restore broad coverage for both tirzepatide (Zepbound) and the new oral Foundayo, ensuring parity in the commercial insurance market 4445.
Globally, state-run healthcare systems are finally capitulating to the clinical evidence. In mid-2026, France became the first European Union nation to fully reimburse both Wegovy and Mounjaro for severely obese patients (BMI ≥35 with comorbidities) through its public social security system, estimating a state cost of €100 million at full rollout 4647. The UK's National Health Service (NHS) and Japan's public health system have also formally integrated the drugs into their public healthcare frameworks with similar BMI restrictions, officially cementing the global paradigm shift of obesity from a "lifestyle choice" to a fiercely managed chronic disease 2047.
Looking ahead, the market is bracing for a massive disruption as original patents for semaglutide begin expiring in major global markets like China, India, Brazil, and Canada in 2026 248. This loss of exclusivity is paving the way for generic manufacturers to flood the international market, driving down prices globally and ensuring that the pharmacological management of obesity becomes accessible to billions 2.
Bottom line
In 2026, tirzepatide (Zepbound/Mounjaro) stands as the most practical, highly effective choice for obesity management, balancing ~21% weight loss with an excellent tolerability profile and wide commercial availability. Retatrutide is the undisputed future heavyweight, boasting an incredible 30% weight reduction and deep liver fat clearance, though patients must wait until at least late 2027 for FDA approval and weigh the risks of its unique dysesthesia (nerve tingling) side effect. Regardless of the chosen medication, current data strongly emphasizes that these are lifelong treatments; ceasing therapy results in rapid, profound weight regain, necessitating ongoing adherence or transitioning to new oral daily pills like orforglipron for affordable, long-term maintenance.