What to Expect from GLP-1 Drugs in 2026
In 2026, glucagon-like peptide-1 (GLP-1) medications have officially transcended their origins as simple weight-loss and diabetes treatments to become systemic disease-modifying therapies for conditions ranging from sleep apnea and liver disease to alcohol addiction. While breakthrough clinical trials demonstrate stunning anti-inflammatory benefits across the human body, sobering failures in Alzheimer's and Parkinson's research - along with complex psychological side effects - reveal that we are only just beginning to understand the boundaries of these metabolic tools. The coming years promise even more powerful "triple-agonist" drugs, though their success will hinge on careful, long-term patient monitoring.
From Gila Monster Venom to a Medical Revolution
To grasp the magnitude of where GLP-1 receptor agonists are heading in 2026, it is essential to understand their highly unusual origins. The foundation of this multi-billion-dollar pharmaceutical revolution did not originate in a synthetic chemistry lab, but rather in the venom of the Gila monster, a venomous lizard native to the southwestern United States and northwestern Mexico 1. Decades ago, endocrinologists researching novel treatments for diabetes isolated a peptide in the lizard's venom called exendin-4 1. This compound shared a roughly 53% structural similarity (homology) with human GLP-1, a hormone produced in the human gut that stimulates insulin release after eating 1.
However, the lizard peptide had a crucial advantage: while human GLP-1 degrades in the bloodstream within minutes, exendin-4 possessed a half-life of several hours 1. This lengthened biological durability made pharmaceutical intervention feasible, ultimately leading to the 2005 approval of exenatide, the world's first GLP-1 receptor agonist, requiring twice-daily injections 1.
In the twenty years since that initial breakthrough, the underlying science has evolved at a blistering pace. Pharmaceutical companies developed synthetic versions of human GLP-1, such as liraglutide (which required daily injections) and eventually semaglutide, which achieved an extended half-life allowing for once-weekly dosing 1. As these drugs hit the market to treat type 2 diabetes, clinicians noticed a profound side effect: patients were losing extraordinary amounts of weight. By mimicking the body's natural satiety signals, the medications were addressing the root biological causes of obesity.
Today, the clinical conversation has shifted entirely. With widespread acknowledgment that obesity is not a failure of willpower but a chronic, adiposity-based metabolic disease, researchers have recognized that the pathways modulated by GLP-1 are implicated in a vast array of interconnected systemic illnesses. From the cardiovascular system to the deep structures of the brain, the therapeutic horizon for these incretin therapies has expanded exponentially.
The Gut-Brain Axis: Rewiring the Reward System
The traditional understanding of GLP-1 focused heavily on the gastrointestinal tract and the pancreas. When nutrients enter the small intestine, specialized L-cells release natural GLP-1 23. This hormone travels to the pancreas to stimulate insulin secretion and reduce glucagon production, thereby regulating blood sugar 24. Simultaneously, it delays gastric emptying, meaning food remains in the stomach longer, sending physical fullness signals to the brain via the vagus nerve 356. This process governs homeostatic eating, which is the biological drive to consume calories to meet basic energy demands 7.
However, the pharmaceutical versions of GLP-1 do much more than slow digestion. Because drugs like semaglutide and tirzepatide persist in the bloodstream for days, they are able to cross the blood-brain barrier at specific structural nodes 24. Once inside the central nervous system, they act directly on brain centers that regulate appetite, craving, and reward 23.
Recent neuroimaging and molecular studies have fundamentally altered our understanding of this process. It is now known that GLP-1 receptors are highly concentrated in the hypothalamus (the brain's metabolic control center) and the nucleus tractus solitarius in the brainstem 238. More surprisingly, they are also present in the mesolimbic reward system, specifically within the ventral tegmental area and the central amygdala 279. This specific neural circuit is responsible for evaluating rewarding experiences and assigning "value" to highly palatable, calorie-dense foods 9.
By activating receptors in the central amygdala, oral and injectable GLP-1 drugs dial back the release of dopamine in major parts of the brain's reward system 7.
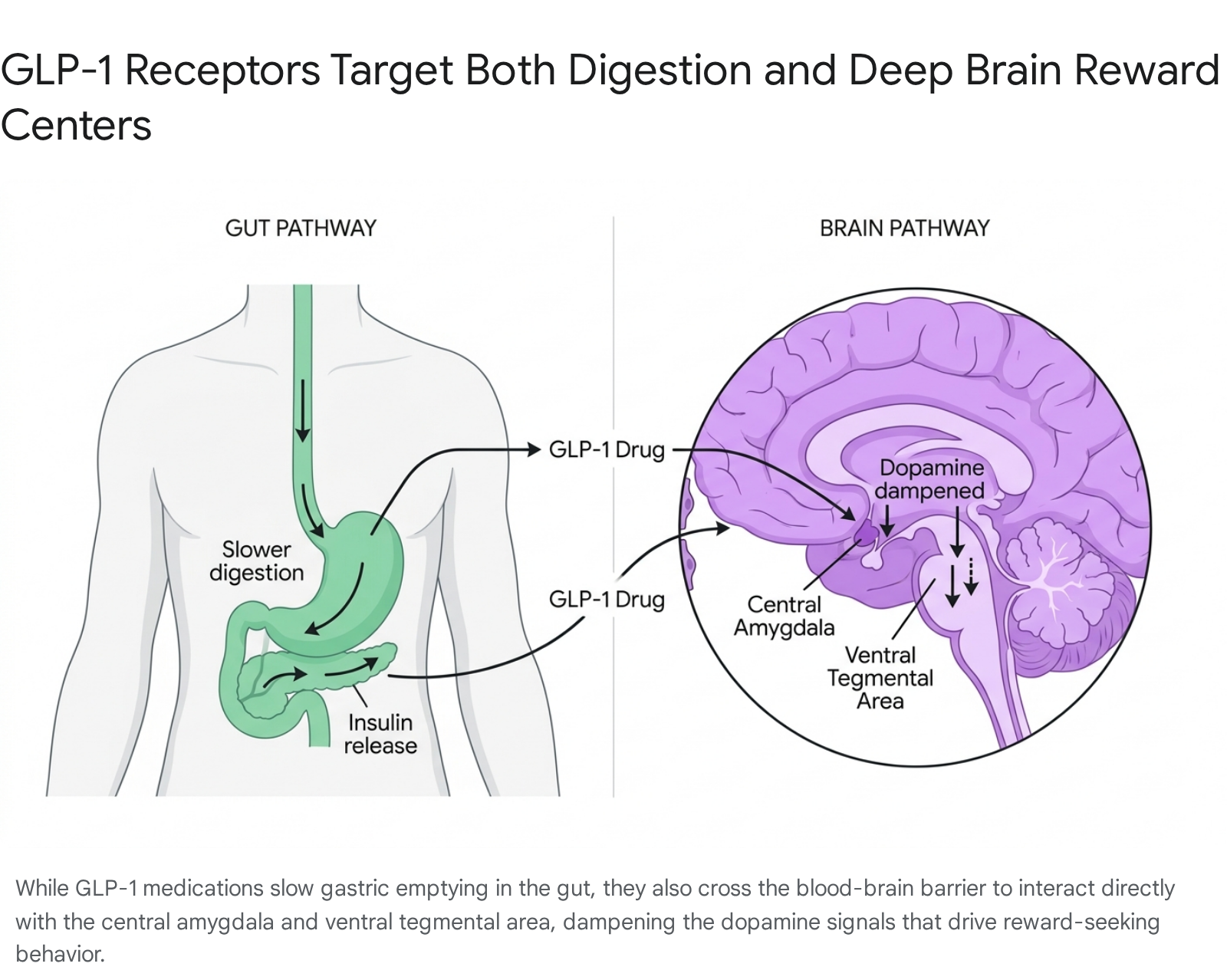
This directly suppresses "hedonic eating" - the compulsion to consume food for pleasure, comfort, or stress relief rather than physical hunger 7. Patients commonly refer to this phenomenon as the silencing of "food noise." This profound neurological mechanism not only explains why patients can easily refuse high-calorie foods while on the medication, but it also provides the biological foundation for why these drugs are now being tested as treatments for substance use disorders and addiction.
Expanding the Pipeline: Recent FDA Approvals
While researchers continue to investigate future applications, regulatory bodies have already recognized the systemic benefits of GLP-1 therapies. Between 2024 and 2025, the U.S. Food and Drug Administration (FDA) approved label expansions for these drugs that fundamentally changed the standard of care in pulmonology, nephrology, and hepatology.
Reversing Obstructive Sleep Apnea
In December 2024, the FDA approved Eli Lilly's tirzepatide (Zepbound) for the treatment of moderate-to-severe obstructive sleep apnea (OSA) in adults with obesity 101112. OSA is a chronic, sleep-related breathing disorder characterized by the complete or partial collapse of the upper airway, leading to repeated pauses in breathing (apnea) and dangerous drops in blood oxygen saturation 101314.
While OSA has traditionally been managed with mechanical interventions like continuous positive airway pressure (CPAP) machines, Zepbound became the first-ever pharmaceutical treatment to address the root physical causes of the disorder 1011. The bidirectionality between obesity and OSA is well-established; excessive adipose tissue around the neck places a heavy mechanical load on the airway, causing it to narrow and close when throat muscles relax during sleep 101214.
The approval was based on the landmark SURMOUNT-OSA Phase 3 clinical trials, which tested tirzepatide against a placebo over 52 weeks in patients who either used CPAP machines or were unwilling/unable to use them 111314. The results demonstrated that tirzepatide dramatically reduced the apnea-hypopnea index (AHI) - the clinical measure of how many breathing pauses a patient experiences per hour 1213. Astonishingly, nearly half of the patients taking the drug saw such significant improvements that their sleep apnea went into clinical remission, effectively resolving the symptoms and eliminating the need for nocturnal respiratory support 1314.
Protecting the Kidneys from Chronic Decline
In January 2025, the FDA granted approval for semaglutide (Ozempic) to reduce the risk of kidney disease worsening, end-stage kidney failure, and cardiovascular-related death in adults with type 2 diabetes and chronic kidney disease (CKD) 15161617. Chronic kidney disease is a progressive, debilitating condition that affects an estimated 37 million adults in the United States, with roughly 40% of patients with type 2 diabetes eventually developing the complication 1618. If left unchecked, CKD necessitates highly invasive dialysis or organ transplantation 1516.
The evidence supporting this approval came from the Phase 3b FLOW trial, a massive international study involving over 3,500 participants 151617. The trial's findings were so definitively positive that an Independent Data Monitoring Committee recommended halting the study early because it had already met its pre-specified efficacy criteria long before the scheduled completion date 151617.
Patients receiving a 1.0 mg weekly dose of semaglutide experienced a statistically significant 24% relative risk reduction for the primary composite outcome, which included a 50% or greater reduction in estimated glomerular filtration rate (eGFR), the onset of kidney failure, or death from cardiovascular or kidney causes 15161718. This established Ozempic as the most broadly indicated GLP-1 receptor agonist in its class, offering vital protection to a highly vulnerable patient population 151618.
Healing Liver Fibrosis and MASH
One of the most eagerly anticipated regulatory milestones was reached in August 2025, when the FDA approved Wegovy (semaglutide 2.4 mg) to treat metabolic dysfunction-associated steatohepatitis (MASH) with moderate-to-advanced liver fibrosis 192021. Previously known as nonalcoholic steatohepatitis (NASH), MASH is a severe, progressive liver disease triggered by metabolic dysfunction 192022. As fat builds up in the liver, it causes toxic inflammation and progressive scarring (fibrosis). If the scarring worsens, it leads to cirrhosis, liver failure, and liver cancer 1920.
Approximately 14.9 million adults in the United States suffer from MASH, yet for decades, the condition went largely unrecognized and untreated due to a lack of pharmaceutical options 192021. The FDA granted accelerated approval based on Part 1 of the pivotal Phase 3 ESSENCE trial 212223. The data revealed that 63% of patients taking Wegovy experienced a total resolution of their steatohepatitis with no worsening of their liver scarring, compared to only 34% of patients on a placebo 212223. Furthermore, 37% of patients on the medication saw an actual reversal and improvement of their liver fibrosis, a deeply significant clinical endpoint 2223.
This approval positioned Wegovy as the first and only GLP-1 therapy cleared for MASH, placing it in direct competition with resmetirom (Rezdiffra), a thyroid hormone receptor beta agonist that was approved for the disease in 2024 20212223.
Summary of Recent Regulatory Breakthroughs
| Medication | Approved Indication | Approval Date | Key Clinical Trial | Primary Clinical Benefit Demonstrated |
|---|---|---|---|---|
| Zepbound (tirzepatide) | Moderate to Severe Obstructive Sleep Apnea (OSA) | December 2024 | SURMOUNT-OSA | Substantial reduction in apnea-hypopnea index (AHI); symptom remission in nearly 50% of patients. 101214 |
| Ozempic (semaglutide) | Chronic Kidney Disease (CKD) in Type 2 Diabetes | January 2025 | FLOW | 24% relative risk reduction in major kidney disease events, dialysis need, and cardiovascular death. 151618 |
| Wegovy (semaglutide) | Metabolic Dysfunction-Associated Steatohepatitis (MASH) | August 2025 | ESSENCE | Resolution of severe liver inflammation in 63% of patients; improvement in fibrosis in 37% of patients. 212223 |
Systemic Inflammation: The Hidden Superpower
As GLP-1 drugs accumulated approvals across vastly different medical specialties, a pressing question emerged in the medical community: how can one class of drugs successfully treat the heart, the kidneys, the liver, and the brain?
Initially, the prevailing assumption was that the cardiovascular and organ-protective benefits were merely secondary downstream effects. The logic suggested that by reducing a patient's total body weight and lowering their blood glucose, the strain on their organs was naturally reduced 2425. While weight loss certainly plays a massive role in improving overall health, recent scientific consensus points to a much more profound mechanism: GLP-1 receptor agonists are highly potent, direct systemic anti-inflammatory agents 2426.
Chronic, low-grade metabolic inflammation is a key driver of atherosclerosis (plaque buildup in the arteries), heart failure, and organ degradation 29. Because GLP-1 receptors are physically present on immune cells, endothelial cells (which line the blood vessels), and cardiovascular tissues, these drugs can directly bind to them and halt the inflammatory cascade at a cellular level 2426.
In early 2026, multiple massive meta-analyses were published analyzing the inflammatory biomarkers of thousands of patients on GLP-1 therapies 252627. The data from over 40 randomized controlled trials showed that patients taking drugs like semaglutide experienced dramatic, statistically significant reductions in high-sensitivity C-reactive protein (hsCRP) and Tumor Necrosis Factor-alpha (TNF-α), which are primary systemic mediators of vascular inflammation and plaque instability 252627. Across trials like SELECT and SUMMIT, incretin therapy reduced hsCRP levels by anywhere from 38% to 50% 29.
Crucially, researchers discovered that this anti-inflammatory effect occurs independently of how much weight a patient loses 2429. In large cardiovascular outcomes trials, patients experienced a drop in major adverse cardiovascular events (like heart attacks and strokes) within the first few months of starting the medication, long before substantial weight loss had actually occurred 29. This realization is prompting a major paradigm shift; medical professionals are increasingly viewing GLP-1 medications not just as anti-obesity drugs, but as systemic vascular-protective and immunomodulatory agents 2429.
A New Frontier: Alcohol Use Disorder and Addiction
Because GLP-1 medications so effectively blunt the dopamine spikes triggered by hyper-palatable foods, researchers naturally hypothesized that the drugs might have a similar effect on the consumption of addictive substances 28293031. Over the past several years, doctors routinely noted anecdotal reports from their obesity patients who spontaneously lost their desire to drink alcohol, smoke cigarettes, or engage in compulsive behaviors after starting medications like Wegovy or Zepbound 3032.
The biological premise was sound. Preclinical animal studies demonstrated that GLP-1 agonists consistently reduced the voluntary self-administration of alcohol, cocaine, fentanyl, heroin, and tobacco by altering the neurobiology of the reward circuits 129. Furthermore, massive population-level analyses of electronic health records in Sweden and Denmark showed that patients prescribed semaglutide or liraglutide for diabetes had up to a 36% lower risk of being hospitalized for alcohol-related issues compared to patients taking other metabolic drugs 12930.
However, observational data and animal models are insufficient for regulatory approval. The medical community required rigorous, randomized, placebo-controlled human trials to prove efficacy.
The 2026 Landmark Trial in Alcohol Use Disorder
In May 2026, a groundbreaking study published in The Lancet provided the most compelling clinical evidence to date that GLP-1s can treat addiction 2832333435. Led by researchers at Copenhagen University Hospital and the U.S. National Institutes of Health (NIH), the trial enrolled 108 treatment-seeking patients diagnosed with both alcohol use disorder (AUD) and comorbid obesity 32333435.
For 26 weeks, all participants received standard cognitive behavioral therapy (CBT). However, they were randomized to receive either a weekly injection of semaglutide or a saline placebo 32333435. The results were staggering. Participants receiving the semaglutide injection experienced a 41.1% reduction in their heavy drinking days, vastly outperforming the 26% reduction seen in the placebo group 3233.
Beyond just the frequency of drinking, the sheer volume of alcohol consumed plummeted. Patients in the semaglutide cohort saw their total monthly alcohol consumption decrease by an average of 1,550 grams, compared to a 1,026-gram decrease in the control group 32. They also reported significantly less intense psychological cravings for alcohol, mirroring the drug's effect on food appetite 29323435.
In the field of addiction medicine, these findings are considered a massive breakthrough. Currently, there are only three FDA-approved medications for alcohol use disorder, such as naltrexone, and they are vastly underutilized due to side effects, patient compliance issues, and modest efficacy 283335. To put the semaglutide trial in clinical perspective, researchers calculated the "number needed to treat" (NNT) - a standard metric of a drug's clinical efficacy. The NNT for semaglutide in this trial was just 4.3, significantly superior to the NNT of 7 or higher associated with currently approved AUD medications 33.
While this Phase 2 data is highly encouraging, researchers caution that larger, longer-duration Phase 3 trials are necessary before securing FDA approval for addiction 1293135. Major trials, such as the STAR trial conducted by the NIH, are actively enrolling Veterans with moderate-to-severe AUD to determine optimal dosing and to ascertain whether the medication is equally effective for individuals suffering from AUD who do not have comorbid obesity 353940.
The Fight Against Neurodegeneration: Alzheimer's and Parkinson's
Given their ability to cross the blood-brain barrier and rapidly decrease neuroinflammation, GLP-1 receptor agonists appeared perfectly suited to tackle the devastating progression of neurodegenerative diseases. Conditions like Alzheimer's and Parkinson's are heavily characterized by toxic protein aggregation (amyloid, tau, and alpha-synuclein), chronic brain inflammation, and a localized loss of insulin sensitivity in brain tissues 3637.
However, the clinical trial readouts across 2025 and 2026 have yielded incredibly complex, mixed results. The outcomes prove that while the GLP-1 biological pathway is relevant to brain aging, delivering the right molecule to the right part of the brain remains a monumental pharmacological challenge.
Mixed Signals in Alzheimer's Disease
In late 2025, the pharmaceutical giant Novo Nordisk reported the top-line results from its highly anticipated EVOKE and EVOKE+ Phase 3 clinical trials 3638. The studies enrolled over 3,800 adults with early-stage symptomatic Alzheimer's disease to test whether an oral formulation of semaglutide could slow cognitive decline 3638. To the deep disappointment of the medical community, the drug completely failed to slow the progression of memory loss or brain degradation over the two-year study period 3638.
Yet, paradoxically, a separate study published shortly thereafter offered immense hope. In December 2025, researchers at Imperial College London released the findings of the ELAD Phase 2b trial, which tested an older, injectable GLP-1 drug called liraglutide on 204 non-diabetic patients with mild to moderate Alzheimer's 36. The results were surprisingly positive: patients treated with liraglutide experienced nearly 50% less brain volume loss (meaning the physical atrophy of the brain was significantly slowed) and demonstrated an 18% slower decline in cognitive function and memory tests compared to the placebo group 36.
Why did one GLP-1 drug fail while another succeeded? Neuroscientists hypothesize that the discrepancy lies in how the drugs are engineered to interact with the blood-brain barrier. Injectable liraglutide is known to successfully penetrate the central nervous system in small but biologically active amounts 36. Conversely, the oral version of semaglutide used in the EVOKE trials was chemically optimized to survive stomach acid and be absorbed in the gastrointestinal tract, which inadvertently severely limited its ability to cross into the brain tissue 36. The contrasting results suggest that the neuroprotective concept of GLP-1 is sound, but future success requires drugs specifically designed for deep central nervous system penetration.
Setbacks and Silver Linings in Parkinson's Disease
An almost identical dichotomy emerged in the pursuit of a disease-modifying treatment for Parkinson's disease. In February 2025, The Lancet published the highly anticipated results of the Exenatide-PD3 trial, a massive Phase 3 study evaluating the GLP-1 drug exenatide 39454640. Following 194 patients over 96 weeks, the trial found absolutely no evidence that the weekly injections slowed disease progression or improved motor symptoms compared to a placebo 454640. Furthermore, specialized DaTscan brain imaging revealed that the drug had no impact on preserving the brain's dopamine-producing neurons 4540. Once again, researchers discovered through spinal fluid analysis that only tiny concentrations of exenatide were actually making it past the blood-brain barrier - roughly 2% of the levels found in the blood serum 4640.
However, just a year prior, a smaller Phase 2 study known as the LixiPark trial evaluating a different GLP-1 drug called lixisenatide offered a much brighter outlook 414243. Published in The New England Journal of Medicine, the study tracked 156 patients with early-stage Parkinson's 4142. Over 12 months, the group receiving daily lixisenatide injections saw virtually zero worsening of their motor symptoms (a negligible reduction of 0.04 points on clinical scales), whereas the placebo group experienced a clear and steady decline 414243.
Ultimately, the neurodegenerative trials of 2025 and 2026 serve as a sobering reminder that GLP-1s are not magic bullets. While the drugs show undisputed potential to shield neurons from inflammatory damage, scientists must fundamentally redesign these molecules to ensure they can flood the brain in high enough concentrations to halt dementia and motor decline.
Summary of Major Neurological Clinical Trials
| Trial Name | Disease Target | GLP-1 Drug Tested | Phase | Primary Outcome / Key Findings |
|---|---|---|---|---|
| EVOKE / EVOKE+ | Alzheimer's Disease | Oral Semaglutide | Phase 3 | Failed. Did not slow disease progression or cognitive decline over 2 years. 3638 |
| ELAD | Alzheimer's Disease | Injectable Liraglutide | Phase 2b | Succeeded. Slowed cognitive decline by 18% and reduced brain volume loss by nearly 50%. 36 |
| Exenatide-PD3 | Parkinson's Disease | Injectable Exenatide | Phase 3 | Failed. Showed no improvement in motor symptoms or dopamine preservation over 96 weeks. 454640 |
| LixiPark | Parkinson's Disease | Injectable Lixisenatide | Phase 2 | Succeeded. Prevented the worsening of motor symptoms over 12 months compared to decline in placebo group. 414243 |
Psychiatric Safety: Suicidal Ideation and Anhedonia
Because modern GLP-1 medications actively alter the neurochemistry of the brain's reward centers, global regulatory agencies have subjected them to intense psychiatric scrutiny. Over the past few years, a complex picture has emerged regarding how these metabolic drugs influence human mood, motivation, and mental health.
Debunking the Link to Suicidal Ideation
In July 2023, the European Medicines Agency (EMA) and the FDA launched massive safety investigations after the Icelandic Medicines Agency reported three isolated cases of suicidal ideation and self-injury in patients taking semaglutide and liraglutide 44454647. Because obesity is already statistically correlated with higher baseline rates of depression, regulators needed to determine if the medication was causing psychiatric deterioration or if the reports were simply a reflection of the underlying patient population 4547.
By early 2024, after reviewing over 150 spontaneous adverse event reports and combing through massive epidemiological databases, both the EMA and the FDA reached a definitive conclusion: there is absolutely no causal link between GLP-1 receptor agonists and suicidal thoughts or self-harm 444648495051.
In fact, the data suggested the opposite. Massive target trial emulation studies utilizing electronic health records revealed that patients prescribed GLP-1s actually exhibited a significantly lower risk of suicidal ideation and new-onset depression compared to matched cohorts taking alternative diabetes medications like SGLT2 inhibitors 505253. The risk reduction was similarly observed in adolescent populations taking the drugs for obesity 50.
Relying on this overwhelming evidence, the FDA took a rare and decisive step in January 2026. The agency explicitly requested that pharmaceutical manufacturers remove the warnings regarding suicidal ideation and behavior from the official prescribing labels of Wegovy, Saxenda, and Zepbound 5253. This sweeping regulatory reversal cemented the class-wide psychiatric safety profile of these medications.
The Reality of Mood Flattening and Anhedonia
While the extreme fears of suicidality have been thoroughly debunked, clinicians in 2026 are highly focused on a more subtle, yet very real, psychiatric side effect: anhedonia.
Because GLP-1 agonists blunt dopamine spikes in the mesolimbic pathway to suppress cravings for food and alcohol, some patients experience an unintended generalized flattening of emotion 5455. In clinical practice, patients occasionally report losing the joy they once found in social engagements, hobbies, or daily life 55. This flattening of hedonic response is a direct reflection of the drug's neurobiological activity 5455.
While the majority of patients actually report significantly improved overall mood - driven by dramatic weight loss, better mobility, and normalized blood sugar - those with a pre-existing history of major depressive disorder require vigilant monitoring 54555664. Medical consensus dictates that prescribers should proactively screen patients for shifts in motivation and joy at every follow-up visit 55. If a patient experiences persistent emotional blunting, physicians are advised to adjust the dosage, modify the dosing schedule, or consider transitioning the patient to an alternative therapy to protect their psychological well-being 5564.
Debunking Pervasive Myths Surrounding GLP-1s
As GLP-1 prescriptions skyrocketed across the globe, they inevitably generated a massive wave of public misunderstanding. In 2026, longitudinal clinical data provides clear answers to the most common myths surrounding these treatments.
- Myth: The drugs permanently shrink your stomach like bariatric surgery. Fact: GLP-1 medications do not physically alter the anatomy or size of the stomach 565. Instead, they chemically slow gastric emptying, meaning food takes longer to process and pass into the small intestine 356566. This prolonged digestion creates a sensation of physical fullness. If the medication is stopped, the speed of gastric emptying returns to its normal, pre-treatment baseline.
- Myth: You don't need to diet or exercise while taking them. Fact: The drugs are highly effective, but they are not magic. Every FDA label explicitly mandates that the drugs be used in combination with a reduced-calorie diet and increased physical activity 666. Furthermore, because the drugs cause rapid weight loss, patients who fail to consume adequate protein and engage in resistance training are at a high risk of losing significant lean muscle mass alongside body fat, which can permanently damage their resting metabolic rate 356.
- Myth: Once you reach your goal weight, you are cured and can stop. Fact: Obesity is recognized by the medical community as a chronic, relapsing biological disease, much like hypertension or high cholesterol 36566. Just as blood pressure spikes if a patient abandons their cardiovascular medication, stopping GLP-1 therapy leads to rapid metabolic rebound. Clinical trial extensions show that patients who discontinue semaglutide or tirzepatide typically experience near-total weight regain within 18 months 656657. These are long-term maintenance medications designed for lifetime management 666.
- Myth: They cause irreversible stomach paralysis and gastrointestinal damage. Fact: While mild-to-moderate gastrointestinal distress (including nausea, diarrhea, and constipation) is the most frequently reported side effect - especially when first initiating treatment or increasing the dose - these symptoms are generally transient 35665. Severe gastrointestinal complications are exceptionally rare. The vast majority of patients develop a tolerance to the medication, and their GI symptoms completely resolve within a few weeks of reaching a stable maintenance dose 5665.
What to Expect Next: Retatrutide and the Triple Agonists
While semaglutide and tirzepatide dominate clinical practice today, the pharmaceutical pipeline is aggressively advancing toward a new generation of even more potent therapies. The most highly anticipated drug development story of 2026 is Eli Lilly's retatrutide, an investigational "triple-G" agonist 576869.
To understand why retatrutide represents such a massive leap forward, one must look at its receptor targets. Semaglutide is a single agonist (targeting only GLP-1). Tirzepatide is a dual agonist (targeting both GLP-1 and GIP) 5769. Retatrutide is the world's first triple-hormone receptor agonist, targeting GLP-1, GIP, and crucially, glucagon 15769.
The Power of the Glucagon Receptor
Historically, the hormone glucagon was viewed simply as the counter-regulatory hormone to insulin - its job was to raise blood sugar when it dipped too low 57. However, researchers have weaponized glucagon's other biological properties to accelerate weight loss. While GLP-1 and GIP work primarily to suppress appetite and increase insulin sensitivity, the activation of the glucagon receptor directly increases a patient's resting energy expenditure and promotes lipolysis, the active breakdown of stored fat 5769.
In highly simplified terms, a patient taking retatrutide eats significantly less food (due to the GLP-1/GIP mechanisms) while simultaneously burning significantly more calories at rest (due to the glucagon mechanism) 5769.
The clinical results of this triple-pathway approach have been truly staggering. In December 2025, Eli Lilly released the highly anticipated top-line results of the TRIUMPH-4 Phase 3 trial, which tested retatrutide in patients suffering from obesity and osteoarthritis 686970. Patients on the highest dose (12 mg, taken once weekly) lost an astonishing mean of 28.7% of their total body weight over 68 weeks - an average absolute weight loss of 71.2 pounds 686970.
This figure represents the highest weight loss efficacy ever recorded in a pharmacologic obesity trial, utterly shattering the roughly 15% seen with Wegovy and the 22% seen with Zepbound 686970. A 28.7% reduction places the efficacy of the injectable medication on par with invasive bariatric surgery 157.
The Approval Timeline
Throughout 2026, the medical and financial sectors are closely monitoring the readouts of the remaining trials in the massive TRIUMPH clinical program 68707172. The pivotal trial required for FDA approval - TRIUMPH-1, which focuses on general obesity - is expected to read out in the middle of 2026 68707172.
If the data from TRIUMPH-1 mirrors the unprecedented weight loss seen in TRIUMPH-4 without any unexpected safety signals, Eli Lilly is on track to submit a New Drug Application (NDA) to the FDA in the fourth quarter of 2026 687071. Assuming a standard 10-to-12-month regulatory review process, retatrutide is projected to receive final FDA approval in late 2027, with a full commercial launch expected in the first half of 2028 68697072.
Bottom line
In 2026, GLP-1 medications have fundamentally reshaped the landscape of chronic disease management. With FDA approvals expanding to cover obstructive sleep apnea, chronic kidney disease, and severe liver fibrosis - alongside highly promising data demonstrating efficacy in treating alcohol use disorder - these therapies are proving to be powerful systemic anti-inflammatory agents. However, highly publicized failures in Alzheimer's and Parkinson's trials demonstrate that successfully delivering these drugs into the brain remains a significant scientific hurdle, and clinicians must remain vigilant in monitoring patients for subtle, drug-induced shifts in mood and emotional reward.