What 2026 Data Shows About Weight-Loss Drug Side Effects
The 2026 clinical data and global pharmacovigilance reports confirm that while next-generation weight-loss medications achieve unprecedented results, gastrointestinal intolerance and novel side effects remain significant hurdles. Regulatory agencies have largely cleared the drugs of causing thyroid cancer and suicidal ideation, but they have issued strengthened warnings for rare complications like severe pancreatitis and illicit compounded formulations.
The New Baseline: From Trials to Global Pharmacovigilance
We are well past the initial honeymoon phase of glucagon-like peptide-1 (GLP-1) receptor agonists. As millions of people worldwide transition from clinical trial participants to long-term, real-world users, the medical community's understanding of obesity medication side effects has matured. In 2026, the conversation has shifted from theoretical risks to highly documented safety profiles, guided by massive global pharmacovigilance databases and the completion of major Phase 3 trials for next-generation drugs.
Today's landscape includes single-receptor agonists like semaglutide, dual-agonists like tirzepatide and the investigational cagrilintide/semaglutide (CagriSema), and upcoming triple-agonists like retatrutide. We also have a new wave of oral non-peptide medications like orforglipron. With this diversity of mechanisms comes a wider, more nuanced spectrum of side effects. Regulators like the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), the UK's Medicines and Healthcare products Regulatory Agency (MHRA), Japan's Pharmaceuticals and Medical Devices Agency (PMDA), and Australia's Therapeutic Goods Administration (TGA) have spent the last two years actively auditing these medications, resulting in several critical label updates.
The Gastrointestinal Ladder: The Most Common Barrier
The most frequent reason people stop taking GLP-1 medications is not a rare, catastrophic event, but persistent, unmanaged gastrointestinal (GI) distress. Because these drugs fundamentally work by slowing gastric emptying and interacting with receptors in the gut and brain to signal fullness, GI side effects are a feature, not just a bug, of the mechanism.
In both clinical trials and real-world surveillance, nausea, vomiting, diarrhea, and constipation dominate the patient experience. Retrospective analyses of the FDA Adverse Event Reporting System (FAERS) database spanning over 18 million reports show that semaglutide is heavily linked to delayed gastric emptying (often colloquially referred to as gastroparesis), severe nausea, and vomiting 1223. The FAERS data indicates that while tirzepatide shares this GI profile, semaglutide demonstrates a slightly broader range of notable GI adverse effects in real-world reporting 23.
Delayed Gastric Emptying and the FAERS Data
Gastroparesis, or delayed gastric emptying, is a relative contraindication that demands careful evaluation. GLP-1 drugs slow gastric motility as part of their core mechanism, which can worsen symptoms in patients with pre-existing gastroparesis 4. The FAERS database highlights that reports of delayed gastric emptying are notably more frequent with semaglutide use compared to other GLP-1s 235.
For patients with a history of significant gastrointestinal issues, clinicians are increasingly approaching GLP-1 therapy with caution. A telehealth provider cannot easily perform a gastric emptying study or assess abdominal distension remotely, making in-person evaluation critical for patients with chronic nausea, early satiety, or postprandial vomiting before initiating therapy 4.
The Microdosing Trend and Telehealth Risks
Clinical trials carefully step up, or "titrate," the medication dosage over several months to allow the body to adapt. In the real world - particularly with the boom of telehealth prescribing - this structured follow-up is sometimes lost 4. When patients are aggressively titrated to higher doses without proper medical guidance, they frequently hit a wall of GI intolerance. Telehealth platforms that skip structured follow-up during this escalation phase risk missing early warning signs, such as persistent vomiting leading to dehydration, electrolyte disturbances, or acute kidney injury 4.
Current expert consensus emphasizes that persistent vomiting is a severe red flag. To combat early GI distress, the off-label practice of "microdosing" - starting at a fraction of the manufacturer's recommended initial dose - has gained traction in 2026 7. While obesity medicine societies have not yet formalized protocols for microdosing, many specialized clinicians use it to build tolerance in highly sensitive patients, slowly increasing the dose over weeks based on real-world response 7.
Does Extreme Weight Loss Mean Extreme Muscle Loss?
One of the most persistent fears surrounding GLP-1 therapy is the claim that it causes disproportionate muscle wasting. Early reports suggested that 25% to 40% of the weight lost on drugs like semaglutide and tirzepatide came from lean mass 8910. However, 2026 data has brought much-needed nuance to this narrative, revealing that the fear of catastrophic muscle loss has been largely overstated due to measurement limitations.
The DXA Scan Illusion and Myosteatosis
Historically, lean mass changes were measured using Dual-energy X-ray Absorptiometry (DXA) scans. DXA measures anything that isn't bone or fat as "lean mass." This means water weight, glycogen stores, organ tissue, and intramuscular fat are all lumped into the lean mass category 9116. When a patient loses weight rapidly, fluid shifts and the loss of intramuscular fat - a highly favorable metabolic adaptation known as reducing myosteatosis - register on a DXA scan as "lean mass loss" 9.
Recent functional studies and advanced MRI data have clarified the picture. The SURPASS-3 MRI sub-study demonstrated that tirzepatide significantly reduces fatty infiltration within the muscle itself, an adaptation DXA would misattribute to muscle loss 9. Furthermore, a 2026 study in Cell Reports Medicine involving both mice and humans provided direct evidence that GLP-1-mediated weight loss targets fat preferentially. In the study, human participants maintained their handgrip and knee extension strength despite a decrease in absolute thigh muscle size, and muscle tissue showed an increase in mitochondrial proteins 6.
Advanced Real-World Body Composition Data
A 2026 real-world Bioelectrical Impedance Analysis (BIA) cohort study presented at the European Congress on Obesity confirmed that following GLP-1 therapy, 80% to 85% of the weight lost is fat mass 7. In this study of 486 adults, fat mass decreased by approximately 18%, while skeletal muscle mass decreased by only 5%. Consequently, relative skeletal muscle mass was preserved or actually increased in over 70% of patients 7.
A 2025 meta-analysis published in Metabolism reached a similar conclusion: while the average GLP-1 user loses some muscle in absolute terms, they end up with the same or a higher proportion of muscle in their body 10. For older adults or those with pre-existing sarcopenia, extra monitoring and a dedicated protocol of 1.2 to 1.6 g/kg/day of protein alongside resistance training are still strongly recommended 106.
The Future: Myostatin Inhibitors
Even though normal GLP-1 weight loss does not cause disproportionate functional muscle wasting, the pharmaceutical industry is racing to optimize body composition further. Enter myostatin inhibitors - drugs that block the body's natural brakes on muscle growth. By targeting activin type II receptors or myostatin directly, these agents reduce the suppression of muscle protein synthesis, allowing lean mass to be maintained or built even during a caloric deficit 1415.
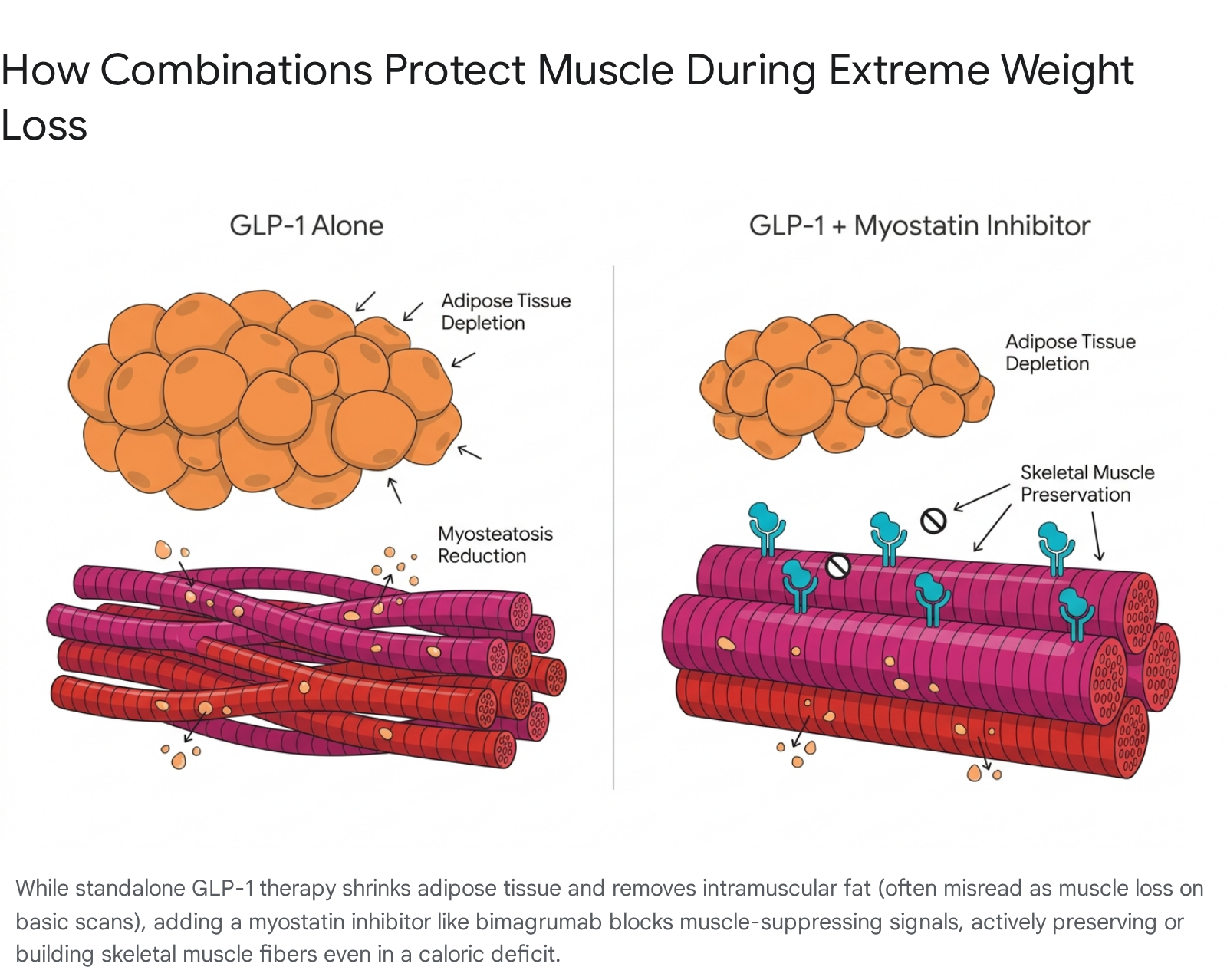
The Phase 2 BELIEVE trial (combining semaglutide with the myostatin inhibitor bimagrumab) and the COURAGE trial (combining semaglutide with trevogrumab) have shown startling results. In the BELIEVE trial, participants lost an average of 17.8 kg at 48 weeks, with approximately 92% of the extra weight lost coming purely from fat mass, leaving muscle almost entirely untouched 914. Similarly, the COURAGE trial demonstrated that combining semaglutide with trevogrumab prevented roughly half of the lean mass loss typically caused by semaglutide alone 14. Side effects for these combinations include new profiles like muscle spasms, acne, and mild diarrhea, but they represent a massive leap forward in preserving metabolic health during radical weight loss 14.
Next-Generation Drugs: New Mechanisms, Novel Side Effects
As the pipeline expands beyond semaglutide and tirzepatide, new mechanisms of action are introducing entirely new safety signals. By looking at 2025 - 2026 trial data for retatrutide, CagriSema, and orforglipron, we can see exactly what the future of obesity medicine side effects looks like.
Retatrutide and the Dysesthesia Signal
Retatrutide is an investigational "triple agonist" targeting GLP-1, GIP, and glucagon receptors. It is currently the most powerful obesity drug in late-stage trials. In the Phase 3 TRIUMPH-4 trial, patients on the maximum 12 mg dose lost an extraordinary 28.7% of their body weight at 68 weeks, with 58.6% of participants losing at least 25% of their body weight - outcomes rivaling bariatric surgery 178.
However, the addition of the glucagon receptor introduces distinct side effects. Because glucagon increases cardiac output and sympathetic drive, retatrutide causes a modest, transient elevation in resting heart rate (+5 to 7 beats per minute) 19. More surprisingly, the Phase 3 trials uncovered a new safety signal: dysesthesia - an abnormal, sometimes painful sense of touch where normal sensations feel prickly, burning, or uncomfortable 8.
In the TRIUMPH-4 trial, dysesthesia occurred in 20.9% of patients on the 12 mg dose, compared to just 0.7% on placebo 8.
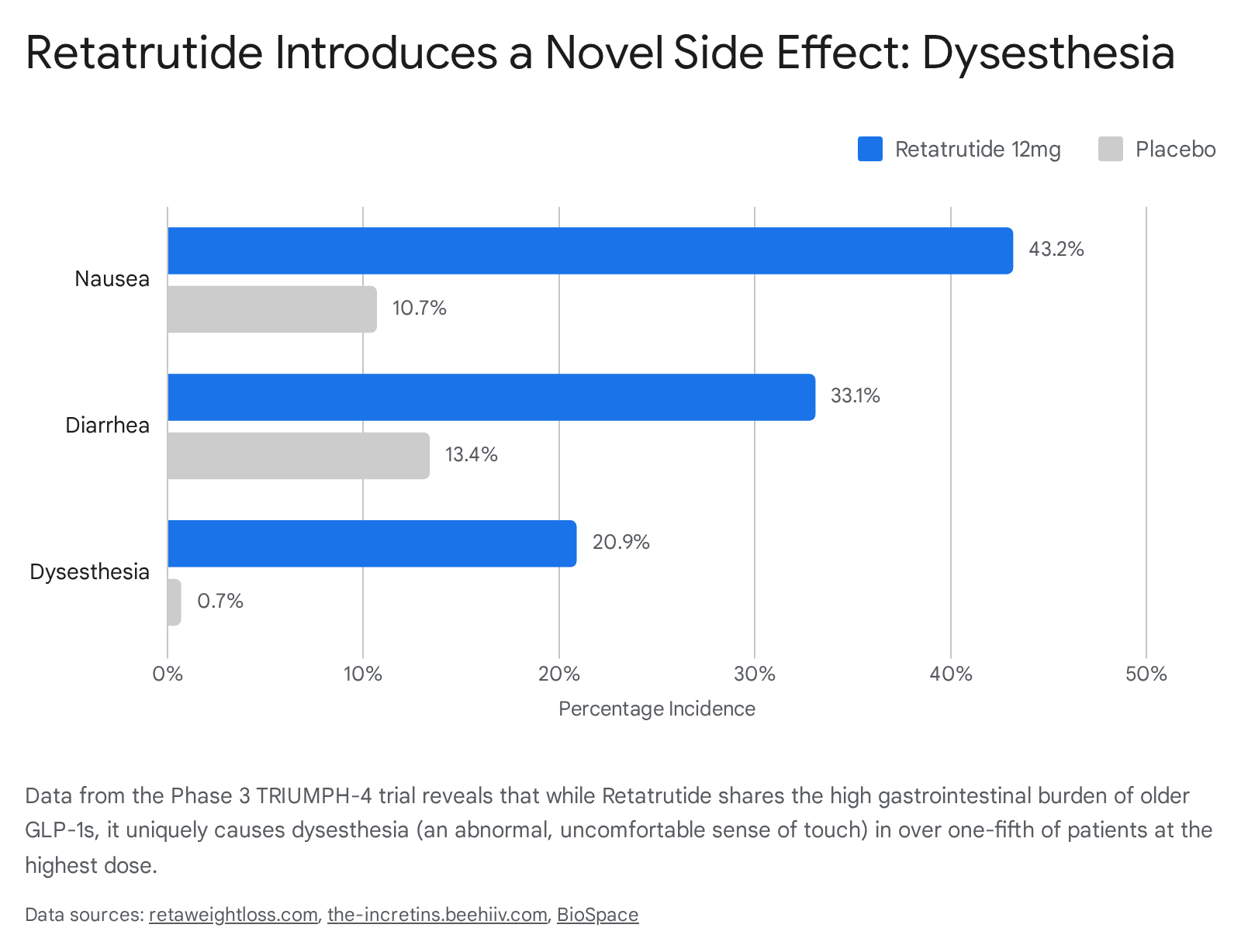
While researchers note it does not frequently lead to discontinuation (affecting about 2% of dropouts), it is a unique tolerability hurdle 178. Overall, retatrutide carries a high discontinuation rate due to adverse events (18.2% at the highest dose). Interestingly, Eli Lilly noted that some of these dropouts were actually due to "perceived excessive weight loss" among patients with lower starting BMIs, highlighting the sheer potency of the drug 820.
CagriSema: High GI Burden for High Efficacy
CagriSema combines semaglutide with cagrilintide, an amylin analogue. By hitting two different appetite-regulating pathways, the Phase 3 REDEFINE 1 trial showed an average weight loss of 22.7% at 68 weeks in adults without diabetes 9. In the REDEFINE 2 trial focusing on patients with Type 2 diabetes, the drug achieved a 15.7% weight reduction 922. The drug also demonstrated remarkable cardiovascular benefits, reducing systolic blood pressure by 10.9 mm Hg 10.
The trade-off for this dual-action is intense gastrointestinal friction. In REDEFINE 1, almost 80% of CagriSema patients experienced a GI adverse event, compared to roughly 40% on placebo 911. Nausea affected 55% of users, while vomiting impacted 26.1% 9. Despite this massive side effect burden, discontinuation rates remained surprisingly low (6% in REDEFINE 1 and 8.4% in REDEFINE 2), suggesting the GI effects were mostly transient and manageable for motivated patients 9.
Orforglipron: The Oral Alternative
While an oral formulation of semaglutide exists, it requires strict fasting protocols and specific water intake. Orforglipron is an investigational, once-daily, non-peptide oral GLP-1 pill that carries no food or water restrictions. In the Phase 3 ATTAIN-1 and ATTAIN-2 trials, it generated between 10.5% and 12.4% weight loss over 72 weeks 121327.
Its safety profile mirrors the injectable GLP-1 class: diarrhea (26-27%), nausea (36%), and vomiting (14-23%) are common at the highest doses, predominantly occurring during the dose escalation phase 1314. In the ACHIEVE-4 cardiovascular outcomes trial, orforglipron demonstrated a stunning 57% reduction in all-cause mortality compared to insulin glargine 29. Discontinuation rates due to adverse events hover around 5% to 10% 1415. For many patients, the sheer convenience of a daily pill will easily justify the transient GI upset.
2026 Drug Profile Comparison
| Medication | Mechanism | Phase 3 Average Weight Loss | Dominant Side Effect Profile | Discontinuation Rate (Adverse Events) |
|---|---|---|---|---|
| Semaglutide (Wegovy) | GLP-1 Agonist | ~15% | High GI (Nausea, Vomiting), Delayed gastric emptying | ~7% |
| Tirzepatide (Zepbound) | GLP-1 + GIP | ~21% | High GI, reduced myosteatosis, mild heart rate increase | ~6 - 15% |
| CagriSema | GLP-1 + Amylin | ~22.7% | Very High GI (Nausea 55%), mostly mild-to-moderate | ~6 - 8.4% |
| Retatrutide | GLP-1 + GIP + Glucagon | ~28.7% | High GI, Dysesthesia (20.9%), increased heart rate | ~18.2% |
| Orforglipron | Oral GLP-1 | ~11 - 12.4% | Moderate GI (Diarrhea 27%, Nausea 36%), no fasting rules | ~5 - 10% |
(Note: Data derived from 2025 - 2026 Phase 3 trials: REDEFINE, TRIUMPH, and ATTAIN. Direct head-to-head trial data is still pending for some comparisons). 179111215
Rare but Severe Complications: Pancreatitis and Ileus
While everyday nausea is expected, regulators remain highly vigilant regarding severe gastrointestinal events that can require hospitalization.
MHRA Warnings on Necrotising Pancreatitis
Acute pancreatitis - inflammation of the pancreas - has long been a known, uncommon risk associated with GLP-1 therapies. However, in January 2026, the UK's MHRA issued a Drug Safety Alert mandating strengthened warnings across all GLP-1 and dual GIP/GLP-1 product labels (including semaglutide and tirzepatide) 1632.
This update was triggered by post-marketing experience revealing rare reports of particularly severe complications, specifically necrotising and fatal pancreatitis 1617. Between 2007 and late 2025, the MHRA received 1,296 Yellow Card reports of pancreatitis linked to these drugs 17. The guidance for 2026 is uncompromising: if a patient develops severe, persistent abdominal pain radiating to the back, often accompanied by nausea and vomiting, the medication must be stopped immediately and never restarted if pancreatitis is confirmed 16.
The Ileus Risk and Japan's PMDA Revisions
Gastric slowing can occasionally progress to a full intestinal blockage, known as ileus. In mid-2025, Japan's Pharmaceuticals and Medical Devices Agency (PMDA) and the Ministry of Health, Labour and Welfare (MHLW) ordered label revisions for both semaglutide and tirzepatide to explicitly include the risk of ileus 18. This aligns with growing international consensus that patients with a history of severe gastrointestinal disease should approach these medications with extreme caution. Japan has also experienced a massive surge in off-label use of GLP-1s for cosmetic weight loss, prompting the Japan Medical Association to actively combat inappropriate prescribing that leads to drug shortages and unmonitored adverse events 1835.
Debunking Cancer and Re-evaluating Mental Health Risks
Perhaps the most reassuring safety developments of the 2025 - 2026 period involve the dismissal of two severe safety signals that previously clouded the GLP-1 class: thyroid cancer and suicidal ideation.
EMA and FDA Clear the Thyroid Cancer Fears
Because GLP-1 drugs caused medullary thyroid carcinoma (MTC) in rodents during early testing, the FDA historically placed a "black box" warning on the drugs, contraindicating them for patients with a personal or family history of MTC 36. In late 2023, the EMA's Pharmacovigilance Risk Assessment Committee (PRAC) completed an exhaustive review of massive observational datasets, non-clinical data, and post-marketing surveillance 19.
The PRAC formally concluded that the available evidence "does not support a causal association" between GLP-1 receptor agonists and thyroid cancer in humans, and opted not to update the product information 19. While caution is still advised for high-risk genetic profiles like Multiple Endocrine Neoplasia syndrome type 2 (MEN2), the broader fear of drug-induced thyroid cancer has been largely laid to rest.
Suicidal Ideation: A Nuanced Global Perspective
In mid-2023, European regulators launched an investigation triggered by the Icelandic medicines agency into reports of suicidal thoughts and self-injury among patients using semaglutide and liraglutide 2021. By April 2024, the EMA announced that clinical trials and post-marketing surveillance showed absolutely no link between the drugs and suicidal behavior 21. In March 2026, the FDA took this a step further, formally requesting that manufacturers remove suicidal ideation and behavior warnings from the labels of Saxenda, Wegovy, and Zepbound, following an all-inclusive meta-analysis of over 99,000 patients proving no elevated risk 41.
However, regulators acknowledge that profound weight loss and shifting metabolic states can impact mental health indirectly. The Australian TGA took a more cautious route, updating its warnings to ensure physicians monitor patients for unusual mood changes, noting the "complex interplay between mental illness and chronic endocrine disorders" 22. The TGA's database recorded 85 mental health-related adverse events linked to GLP-1s by late 2025 22. Similarly, Singapore's Health Sciences Authority (HSA) continues to monitor the situation closely, though they report zero local adverse events regarding self-harm associated with the medications 2324.
The Hidden Danger: Counterfeits and the Compounding Grey Market
Perhaps the most acute risk surrounding weight-loss drugs in 2026 has nothing to do with the pharmaceutical molecules themselves, but rather how patients are sourcing them. Global shortages in 2024 and 2025 gave rise to a massive compounding and counterfeit market. Even as the FDA declared the semaglutide and tirzepatide shortages largely resolved in early 2026, the grey market persists 41.
Salt Forms and Dosing Errors
The FDA and EMA have issued severe warnings regarding unapproved GLP-1 drugs. The FDA has received multiple reports of hospitalizations directly linked to dosing errors with compounded injectable products 25. Because patients or telehealth providers must manually draw doses from vials, miscalculations are rampant. Furthermore, the FDA has warned that many compounders are selling "salt forms" of the drug (semaglutide sodium or semaglutide acetate), which are structurally different from the approved active ingredients and have never been proven safe 25.
Global Crackdowns on Illicit E-Commerce
Regulators are actively cracking down on the illegal distribution of experimental drugs. The FDA recently issued warning letters to companies distributing active pharmaceutical ingredients for retatrutide and cagrilintide, neither of which are legally available or approved for compounding 25.
Globally, the scale of the counterfeit market is staggering. In Europe, the EMA is actively pulling down thousands of fake social media profiles and websites selling fraudulent weight loss pens that often contain harmful substances instead of GLP-1 agonists, resulting in life-threatening interactions 26. In Asia, Singapore's HSA seized over $750,000 worth of illegal health products and removed more than 2,300 online listings in 2025 alone, combating products spiked with potent steroids and banned ingredients that have caused acute kidney injuries and Cushing's syndrome 27.
Bottom line
In 2026, the safety profile of weight-loss medications is clearer than ever: they are highly effective but practically guaranteed to cause gastrointestinal friction during the dose escalation phase. Major fears regarding muscle wasting, thyroid cancer, and suicidal ideation have been largely debunked or contextualized by global regulators, though patients must remain vigilant for rare complications like severe pancreatitis and ileus. As next-generation drugs like retatrutide and CagriSema enter the market, patients and providers will have to weigh unprecedented, bariatric-level weight loss against novel side effects like skin dysesthesia and elevated heart rates.