Foundayo (Orforglipron) Cost, Coverage, and Access in 2026
Patients prescribed Foundayo (orforglipron) in 2026 can anticipate out-of-pocket costs ranging from $25 per month with commercial insurance copay cards to $149 - $349 per month for uninsured individuals utilizing manufacturer direct-to-consumer platforms. While the medication has been rapidly integrated into major pharmacy benefit manager (PBM) formularies following its accelerated April 2026 FDA approval, actual patient access remains heavily restricted by employer-mandated prior authorizations and step-therapy requirements. The international market rollout remains pending, with European and UK patients unlikely to see widespread availability through national health systems before late 2026 or 2027. It is essential to acknowledge that as the global cardiometabolic landscape evolves, specific coverage details, formulary statuses, and out-of-pocket costs throughout 2026 and 2027 are subject to real-time adjustments and represent forward-looking projections based on early launch data.
For millions of patients, the biological miracles of modern metabolic medicine have been inextricably linked to the physical and logistical friction of weekly injections. From navigating persistent needle phobias to managing complex cold-chain storage during air travel, the physical delivery mechanism has stood as the primary barrier to long-term patient adherence 1. The arrival of a daily, non-peptide oral GLP-1 receptor agonist fundamentally dismantles these barriers, offering a highly effective obesity treatment model designed for seamless integration into real-world routines. However, a widespread misconception persists in the public and corporate consciousness: the assumption that transitioning from a complex biologic injection to a daily pill inherently translates to cheap, generic-level pricing. Orforglipron is a highly advanced, patented small molecule 1. While its manufacturing bypasses the expensive, supply-constrained bio-fermentation processes required for peptide injectables, its pricing strategy is deliberately calibrated to protect the revenue margins of its injectable sibling, Zepbound (tirzepatide), while simultaneously undercutting competitors in the cash-pay market 142.
This comprehensive report analyzes the clinical mechanisms, efficacy data, out-of-pocket economics, PBM formulary dynamics, and global rollout trajectory of Foundayo in the 2026 healthcare ecosystem.
What Exactly Is Foundayo and How Does It Work?
To understand why Foundayo represents a monumental scientific milestone, it is necessary to examine the biological hostility of the human digestive tract. Traditional GLP-1 medications, such as semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound), are peptides 378. Peptides are essentially short chains of amino acids - fragile protein structures that mimic naturally occurring incretin hormones responsible for regulating appetite, slowing gastric emptying, and stimulating insulin release 379.
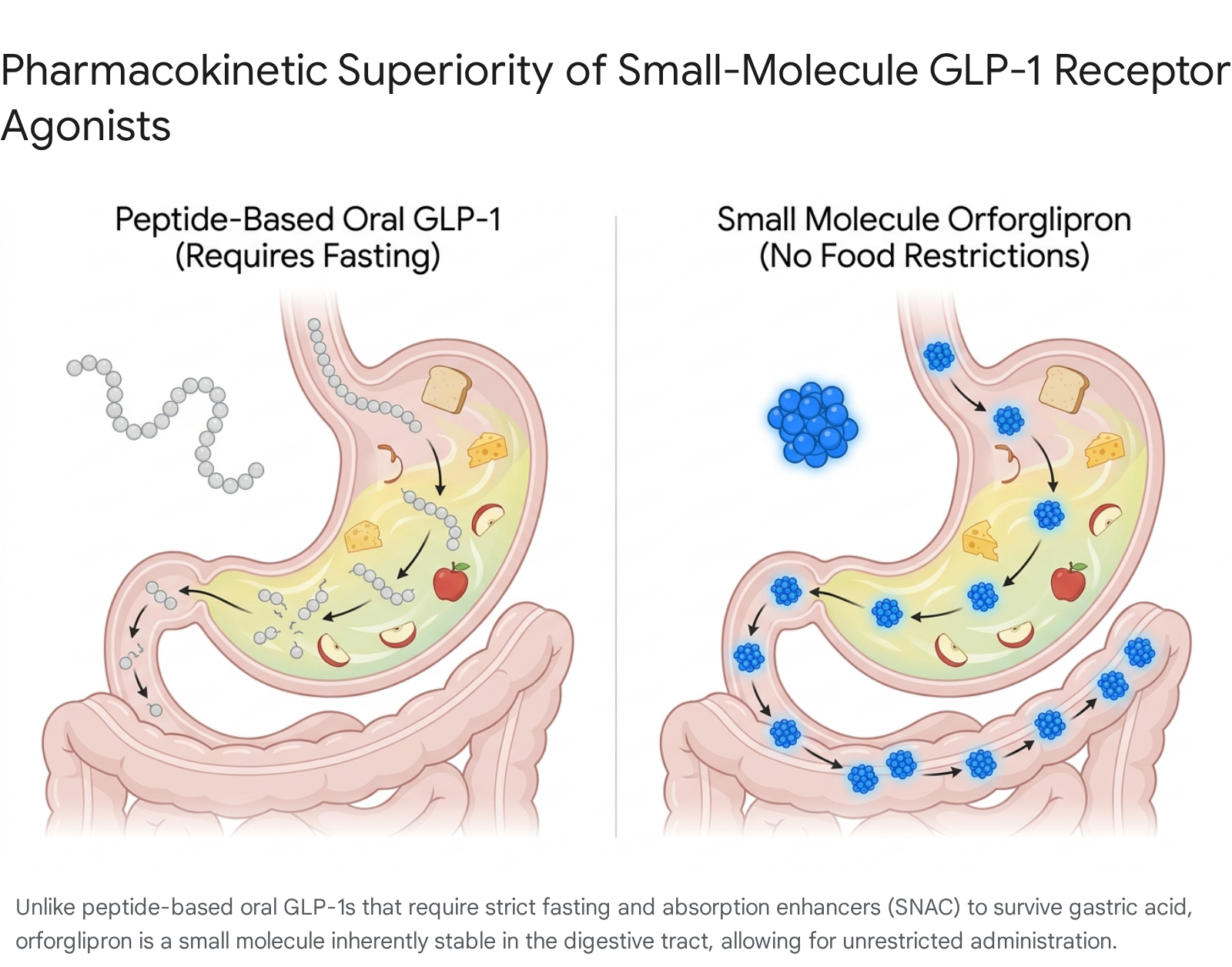
An effective, accurate analogy is to view peptide drugs as delicate origami sculptures. Dropping these delicate structures into the highly acidic, enzyme-rich environment of the human stomach is equivalent to dropping a paper origami crane into an industrial shredder 37. The digestive system is designed to dismantle proteins, rendering the medication useless before it can be absorbed into the bloodstream 3. To bypass this destructive environment, pharmaceutical companies historically relied exclusively on subcutaneous injections. Novo Nordisk eventually achieved the first oral peptide breakthrough with Rybelsus and the Wegovy pill by combining the semaglutide peptide with a specialized absorption enhancer called SNAC (sodium N-[8-(2-hydroxybenzoyl)amino]caprylate) 10412. Returning to the analogy, SNAC acts as a temporary, imperfect protective bubble around the origami crane. However, this chemical bubble is highly sensitive and requires a perfectly empty "shredder" to function properly. Consequently, oral semaglutide requires stringent administrative rules: it must be taken immediately upon waking, on a completely empty stomach, with no more than four ounces of water, followed by a mandatory 30-minute fasting period where no other food, drink, or medication can be consumed 105146.
Foundayo (orforglipron), originally discovered by Chugai Pharmaceutical and exclusively licensed by Eli Lilly in 2018, is fundamentally different; it is not a peptide 137. Extending the previous analogy, if a peptide is a delicate origami sculpture, a small molecule is a solid titanium cube. Orforglipron is a synthetic, non-peptide small molecule chemically engineered to effortlessly withstand the highly acidic environment of the stomach and the enzymatic gauntlet of the intestines without relying on permeation enhancers 7812.
At the molecular level, sophisticated cryogenic electron microscopy (Cryo-EM) demonstrates that orforglipron binds uniquely within the upper helical bundle of the GLP-1 receptor 4. It acts as a highly potent partial agonist that heavily favors cyclic adenosine monophosphate (cAMP) signaling pathways over beta-arrestin recruitment, facilitating sustained receptor activation 4. Because its absorption does not rely on transient changes in gastric pH or specialized chemical enhancers, Foundayo achieves high oral bioavailability without any dietary restrictions 417. Patients can take the pill at any time of day, alongside a heavy meal, a cup of coffee, or concurrently with other daily medications, drastically reducing the friction of daily adherence that historically plagued early oral GLP-1 therapies 7178.
How Does Foundayo Compare to Injectables and Other GLP-1 Pills?
While Foundayo offers unprecedented administrative convenience, its clinical efficacy profile places it in a distinct therapeutic tier below the most powerful dual-agonist injectables. This dynamic presents patients and clinicians with a calculated choice between achieving maximum absolute weight loss and maintaining the ease of daily administration.
The FDA's expedited 50-day approval of Foundayo in April 2026 was heavily supported by the rigorous Phase 3 ATTAIN clinical trial program, which enrolled over 4,500 participants globally across various registration trials 17. In the pivotal ATTAIN-1 trial, which specifically evaluated adults with obesity (or overweight individuals presenting with at least one weight-related comorbidity) without diabetes, orforglipron demonstrated significant, dose-dependent weight reduction over a 72-week period 7910.
Participants randomized to receive the highest maintenance dose (36 mg in the clinical trial framework, marketed contextually as 17.2 mg for clinical prescription) lost an average of 12.4% of their baseline body weight, equating to an absolute reduction of 27.3 pounds 911. This performance starkly contrasted with the placebo cohort, which achieved a mere 0.9% (2.2 pounds) weight reduction over the same 72-week duration 112. The depth of response was equally notable; nearly 60% of participants on the highest dose achieved at least a 10% reduction in overall body weight, and approximately 40% achieved a 15% reduction 9.
Beyond raw weight reduction, the cardiovascular and metabolic secondary endpoints were clinically profound. At the highest dose, patients experienced an average 9-centimeter reduction in waist circumference, a 21.6% reduction in circulating triglycerides, an 8.5% drop in non-HDL cholesterol, and a systolic blood pressure reduction of nearly 7 mmHg 10. In exploratory analyses, the inflammatory marker high-sensitivity C-reactive protein (hsCRP) dropped by nearly 48%, highlighting the systemic anti-inflammatory benefits of the small molecule 10. Furthermore, in the ATTAIN-2 trial - which focused exclusively on patients suffering from obesity alongside concurrent Type 2 diabetes - a once-daily dose of orforglipron reduced average body weight by 10.5% (22.9 pounds) while simultaneously driving significant reductions in HbA1c levels 12.
Additional data stems from the ACHIEVE clinical program, which directly pitted orforglipron against competitors in diabetic populations. In these head-to-head trials, orforglipron demonstrated marked superiority over oral semaglutide (Rybelsus). Patients taking the highest orforglipron dose saw their HbA1c levels drop by an average of 1.9%, compared to a 1.5% drop for those on Rybelsus 613. Correspondingly, weight loss in this diabetic cohort reached approximately 18 pounds (8% of starting weight) for orforglipron versus 11.5 pounds (5%) for Rybelsus 6.
However, when indirectly compared to the broader obesity market, orforglipron's 12.4% weight loss ceiling falls short of the 15% to 16.6% average weight loss observed with Novo Nordisk's oral and injectable Wegovy (semaglutide) 9111426. Furthermore, it noticeably trails the 21% to 22.5% reductions routinely achieved by Eli Lilly's own injectable dual-agonist, Zepbound (tirzepatide) 926. A specialized population-adjusted indirect treatment comparison indicated that oral semaglutide resulted in approximately 3 percentage points greater weight loss than orforglipron across similar timelines, though this must be weighed against the strict fasting protocols required by semaglutide 15.
The safety profile of Foundayo closely aligns with the broader GLP-1 receptor agonist class, heavily dominated by gastrointestinal adverse events. The most common side effects reported in clinical trials include nausea, constipation, diarrhea, vomiting, indigestion, and abdominal pain 58. Because Foundayo acts as a highly potent partial agonist, the gastrointestinal impact during the initial dose-titration phase can be severe if not properly managed. Notably, the discontinuation rate due to adverse events in the ATTAIN-1 trial reached 10.3% for patients on the highest dose, compared to just 2.7% for the placebo group 11. Comparative indirect studies noted that patients receiving orforglipron had nearly four times higher odds of discontinuing treatment due to adverse events, and fourteen times higher odds of discontinuation specifically due to gastrointestinal events, than those taking oral semaglutide 1315.
To mitigate these tolerability challenges, Foundayo employs a highly graduated titration schedule. Patients initiate therapy at a baseline 0.8 mg dose, maintaining this for a minimum of 30 days before escalating to 2.5 mg. Subsequent step-ups to 5.5 mg, 9 mg, 14.5 mg, and finally the maximum 17.2 mg dose are executed at 30-day intervals, allowing the patient's gastrointestinal tract to acclimate to the drug's mechanisms and minimizing abrupt adverse reactions 52829.
Comparison of Leading GLP-1 Therapies in 2026
To fully grasp Foundayo's strategic positioning, it is vital to contrast its pricing, efficacy, and administrative format against its primary pharmaceutical rivals.
| Medication | Manufacturer | Active Ingredient | Dosing Format | Peak Avg. Weight Loss | Notable Restrictions | Expected 2026 Monthly List/Cash Price | Typical Commercial Copay Card Terms |
|---|---|---|---|---|---|---|---|
| Foundayo | Eli Lilly | Orforglipron | Daily Pill (Small Molecule) | 11.2% - 12.4% | None (Any time, with/without food) | $149 (Starter) to $349 (Max Dose) | $25/month; Max savings $100/mo, $1,000/yr. Limit 10 fills/yr. |
| Wegovy Pill | Novo Nordisk | Oral Semaglutide | Daily Pill (Peptide + SNAC) | 14.0% - 16.6% | Strict morning fasting; wait 30 mins | $149 (Starter) to $299 (Max Dose) | $25/month; Max savings $100/mo. Limited to eligible plans. |
| Zepbound | Eli Lilly | Tirzepatide | Weekly Sub-Q Injection | 21.0% - 22.5% | Requires refrigeration, needle injection | $299 (Vial Starter) to ~$1,086 (Pen List) | $25/month; Max savings up to $150/mo. Vials excluded from card. |
| Rybelsus | Novo Nordisk | Oral Semaglutide | Daily Pill (Peptide + SNAC) | 5.0% - 8.0% (T2D focus) | Strict morning fasting; wait 30 mins | Varies widely (Off-label for obesity) | Generally restricted strictly to Type 2 Diabetes diagnoses. |
What Will Foundayo Cost Me Out of Pocket in 2026?
The pricing strategy for Foundayo in 2026 reflects a sophisticated economic balancing act by Eli Lilly. The manufacturer must rapidly expand the total addressable market by lowering financial barriers to entry, while simultaneously preventing mass cannibalization of its highly profitable Zepbound injectable franchise. To achieve this, Lilly utilizes a tiered, channel-specific pricing model designed to capture both the insured and self-pay demographics 4.
For patients whose employer-sponsored or commercial health insurance plans affirmatively include Foundayo on their formulary, out-of-pocket costs are highly subsidized. Eli Lilly's official commercial savings card allows eligible, commercially insured patients to pay as little as $25 for a one-month prescription 14730. However, these manufacturer copay cards contain strict limitations that patients frequently overlook until they reach the pharmacy counter. The Foundayo savings card is subject to maximum monthly savings caps - typically subsidizing up to $100 per 1-month fill, with a separate maximum annual savings limit of $1,000 per calendar year 16. Furthermore, the card may only be used for a maximum of 10 prescription fills per calendar year, requiring patients to carefully manage their refills or face full out-of-pocket costs for the remaining two months of the calendar year 216.
A defining feature of the 2026 obesity market is the massive, systemic expansion of direct-to-consumer (DTC) pharmaceutical distribution. Acknowledging that over 16 million Americans with private insurance face absolute formulary exclusions for weight-loss medications, Eli Lilly aggressively expanded its LillyDirect online pharmacy platform 832. Through LillyDirect, uninsured patients - or those with commercial insurance that explicitly denies coverage for obesity medications - can bypass traditional retail pharmacy markups and purchase Foundayo at a reduced, tiered cash price.
The cash pricing is heavily dose-dependent, a strategic maneuver designed to lure patients in with a low starter cost before stepping up the financial commitment as the clinical dose increases. The 0.8 mg starting dose commands a cash price of $149 per month 72916. Upon titration, the 2.5 mg dose costs $199 per month, while the 5.5 mg and 9 mg maintenance doses cost $299 per month 2916. The highest 14.5 mg and 17.2 mg doses carry a standard list price of $349 per month, though Lilly frequently applies automated purchase offers that discount these maximum doses back to $299, provided the patient completes their refill within a strict 45-day window 52916.
This pricing structure directly mirrors Novo Nordisk's strategy for the Wegovy pill, which also launches at an identical $149 for the starting dose but caps permanently at $299 for its maximum therapeutic doses 1734. Industry analysts note that Lilly purposefully priced the highest doses of Foundayo slightly higher than oral Wegovy to avoid triggering a destructive "price war" in the US cash-pay market, relying instead on Foundayo's superior convenience and lack of fasting restrictions to justify the modest premium 2. In contrast, the direct-to-consumer cost for Zepbound single-dose vials remains steeper, starting at $299 for the lowest 2.5 mg dose and quickly escalating to $449 per month for the higher 7.5 mg through 15 mg maintenance doses 1837.
Historically, Medicare Part D has been statutorily prohibited from covering any medications prescribed exclusively for weight loss. However, intense political pressure and a landmark macroeconomic agreement between the White House, Eli Lilly, and Novo Nordisk drastically altered the regulatory landscape in late 2025. Under the "Most-Favored-Nation" pricing framework negotiated by the Trump Administration, Medicare beneficiaries secured unprecedented access to GLP-1 therapies 3219.
Beginning July 1, 2026, through the newly established Medicare GLP-1 Bridge program, eligible Medicare Part D individuals will pay a capped maximum of $50 per month for both Foundayo and Zepbound, pending final regulatory implementations 1472021. In exchange for these drastic price concessions in the government channel, pharmaceutical manufacturers received three years of tariff relief on pharmaceutical imports and were granted sweeping immunity from future legislative pricing mandates 1922. This geopolitical maneuvering ensures that over 40 million Americans reliant on government insurance programs finally possess a financially viable pathway to obesity care 22.
Will My Insurance Cover Foundayo?
For commercially insured Americans, access to Foundayo is dictated almost entirely by Pharmacy Benefit Managers (PBMs) - the powerful, consolidated intermediaries who design prescription formularies, dictate step-therapy protocols, and negotiate backend rebates with drug manufacturers 23.
By mid-2026, Eli Lilly secured a major access milestone: all three of the nation's largest PBMs - CVS Caremark, Express Scripts, and OptumRx, which collectively manage nearly 80% of prescription drug claims in the United States, covering 270 million people - agreed to cover Lilly's full obesity medicine portfolio, including Foundayo 202123.
The inclusion of Foundayo on CVS Caremark's standard commercial template, effective June 1, 2026, represents a massive strategic and public relations victory for Lilly 2021. In mid-2025, CVS Caremark had controversially dropped Zepbound from its preferred formulary entirely in favor of a highly lucrative rebate deal with Novo Nordisk that established Wegovy as the exclusive preferred treatment 2124. This exclusive arrangement triggered widespread patient backlash and prompted a class-action lawsuit alleging that CVS Caremark violated the Employee Retirement Income Security Act (ERISA) by arbitrarily restricting care and breaching fiduciary duties to plan members 2124. Facing intense legal pressure and threats of employer attrition, CVS Caremark abruptly reversed course in May 2026, adding the newly approved Foundayo to formularies immediately and formally restoring Zepbound coverage by October 1, 2026 2125.
This high-profile PBM reversal highlights a broader industry trend: the sheer patient demand for varied GLP-1 formulations - ranging from injectable peptides to small-molecule pills - is forcing PBMs to abandon single-manufacturer exclusivity deals in favor of broader, multi-drug formularies that prioritize patient choice and physician discretion 21.
How Can I Navigate Employer Formulary Exclusions and Step-Therapy?
While PBMs may place Foundayo on their standard commercial formularies, the ultimate decision to fund the medication rests with the self-insured employer. In 2026, GLP-1 drugs account for an estimated 14% of all prescription drug spending nationally, creating an unsustainable fiscal burden for many corporations 45. Faced with annual costs exceeding $10,000 per user on branded injectables, employers are implementing aggressive utilization management strategies 46.
Only about 37% of self-funded employers currently offer broad GLP-1 coverage for weight loss without severe restrictions 47. The remainder utilize tactics ranging from outright exclusions to complex, multi-tiered step-therapy pathways 47. Navigating this restrictive environment in 2026 requires meticulous clinical documentation and strategic maneuvering by patients and their healthcare providers.
1. Documenting Baseline Metrics for Prior Authorizations
If an employer plan opts to cover weight-management drugs, the patient must inevitably overcome a strict Prior Authorization (PA) hurdle 48. Insurers rarely approve GLP-1s based on a simple prescription. Patients must ensure their provider meticulously documents baseline metrics before the very first dose is taken. Criteria typically mandate a documented Body Mass Index (BMI) of $\ge 30 \text{ kg/m}^2$, or a BMI of $\ge 27 \text{ kg/m}^2$ paired with at least one documented weight-related comorbidity, such as hypertension, dyslipidemia, prediabetes, or obstructive sleep apnea 1748. Crucially, failure to record the exact baseline weight prior to treatment initiation will almost certainly result in an administrative denial when the patient applies for a renewal PA six months later, as insurers require definitive proof of at least 5% weight loss from baseline to continue funding the medication 48.
2. Identifying the "Diabetes Loophole"
Many employer health plans that explicitly exclude weight-loss medications will still fully cover GLP-1s for the treatment of Type 2 Diabetes to comply with standard chronic care mandates 4749. The critical factor for PA approval in these instances is whether the patient has ever met the diagnostic criteria for diabetes, universally defined as a historical Hemoglobin A1c $\ge 6.5\%$ 48. If a patient previously recorded an A1c of 6.6% but has since lowered it to 6.0% through lifestyle interventions, they still legally qualify for the diabetes indication under most plan rules. Submitting the PA under an obesity diagnostic code rather than leveraging a historical diabetes code is the leading cause of administrative denial for otherwise eligible patients 48. While Foundayo is primarily approved for weight management as of early 2026, Lilly's ongoing ACHIEVE clinical trials aim to secure a formal Type 2 Diabetes indication later in the year, which will immediately open this coverage pathway for orforglipron 28.
3. Surviving Step Therapy and Lifestyle Mandates
Step therapy requires a patient to actively try and clinically "fail" on a cheaper, preferred medication before the insurer will approve the newer, more expensive drug 45. Some PBMs may mandate that patients try Novo Nordisk's Wegovy, or even older generics like naltrexone-bupropion, before they will authorize Foundayo 4850. Additionally, according to industry surveys from Mercer, approximately 38% of employers with GLP-1 coverage now mandate active participation in a structured lifestyle or weight management coaching program as a rigid condition of continued medication access 45. If a patient was already paying out-of-pocket for Foundayo, or changes jobs to a new employer plan with strict step-therapy rules, providers can frequently bypass these delays by submitting a "Continuation of Therapy" PA. This requires thoroughly documenting the current medication dose, the duration of ongoing therapy, and the successful clinical weight response achieved thus far, establishing a medical necessity to remain on the current drug 48.
4. Bypassing the Plan Entirely via Tax-Advantaged Accounts
If an employer institutes a hard carve-out completely excluding all anti-obesity medications regardless of PA status, internal appeals are largely futile 48. In these scenarios, employees should look toward employer-funded Health Reimbursement Arrangements (HRAs) or employee-funded Flexible Spending Accounts (FSAs) and Health Savings Accounts (HSAs). IRS regulations explicitly permit the use of pre-tax funds for weight-loss medications if the treatment is formally prescribed by a physician for a specific diagnosed disease, such as obesity, hypertension, or heart disease (but not for general cosmetic improvement) 4651. Patients can legally leverage these tax-free funds in conjunction with the LillyDirect $149 - $349 cash-pay pricing to create a sustainable, discounted financial bridge entirely outside the employer's restrictive health plan 46.
When Will Foundayo Be Available Outside the US?
The rapid, aggressive rollout of Foundayo in the United States highlights a stark contrast in global regulatory, manufacturing, and pricing frameworks. In the US, Eli Lilly strategically utilized an FDA Commissioner's National Priority Voucher (CNPV) to exponentially accelerate the review process. This controversial pathway, intended for products aligned with urgent national health priorities, allowed Lilly to secure FDA approval in a record-breaking 50 days - the fastest approval timeline observed since 2002 145226. Despite congressional pushback regarding the CNPV program's potential to erode public confidence in FDA review standards, the maneuver was highly successful 26. Anticipating this rapid clearance, Lilly deliberately stockpiled $1.5 billion worth of pre-launch inventory - predominantly orforglipron - to flood the US market and decisively prevent the catastrophic supply shortages that plagued the early commercial rollouts of Mounjaro and Wegovy 2654.
Conversely, international markets operate on markedly slower, value-based appraisal timelines that prioritize long-term health economics over rapid market access.
In the United Kingdom, for example, Foundayo remains an unlicensed, investigational medication as of mid-2026 5556. While Eli Lilly submitted its comprehensive clinical data package to the Medicines and Healthcare products Regulatory Agency (MHRA) concurrently with its global submissions in 2025, the UK regulatory process dictates a distinct, two-phased rollout that tests the patience of consumers 2854.
First, industry forecasts anticipate MHRA marketing authorization for orforglipron to land in the latter half of 2026 5456. Once approved, the drug will become legally available for prescribing through private medical networks and online pharmacies 2857. Because the UK pharmaceutical market does not utilize the opaque, rebate-driven US PBM structure, private out-of-pocket pricing is expected to be significantly more transparent. Early estimates project UK private prescription costs to land between £100 and £300 per month, largely mirroring the tiered US cash-pay equivalents established through LillyDirect 305458.
However, MHRA approval does not equate to access for the general public. The National Institute for Health and Care Excellence (NICE) must independently appraise the clinical and cost-effectiveness of orforglipron before it can be prescribed and subsidized on the National Health Service (NHS) 5758. The NICE review process is notoriously rigorous, evaluating long-term health economics, quality-adjusted life years, and the absolute cost of the drug against existing standard-of-care treatments. Consequently, NHS integration and widespread public access to Foundayo is highly unlikely before 2027 at the earliest 5759.
Until official MHRA approval is secured, UK patients cannot legally import Foundayo from the United States, forcing continued reliance on currently licensed peptide alternatives such as Wegovy and Mounjaro 5960. The small-molecule nature of orforglipron, however, promises a highly resilient global supply chain once these regulatory hurdles are cleared. Unlike biologic peptides that require complex, time-consuming fermentation processes and strict cold-chain logistics, small-molecule pills can be rapidly synthesized at immense scale in traditional pharmaceutical manufacturing facilities, suggesting that once international approvals are granted, global supply will comfortably meet the soaring demand 130.
Bottom line
The 2026 launch of Foundayo (orforglipron) represents a critical inflection point in the treatment of obesity, transitioning the clinical standard from complex peptide injectables to a resilient, small-molecule daily pill. By entirely eliminating fasting restrictions, strict timing protocols, and cold-chain logistics, Foundayo substantially lowers the behavioral friction of long-term adherence.
While the medication does not achieve the peak 20%+ weight loss routinely seen with injectable dual-agonists like Zepbound, its 12.4% efficacy profile provides a highly compelling alternative for needle-averse populations and those seeking sustainable long-term maintenance therapy. Economically, Eli Lilly has aggressively structured direct-to-consumer pricing ($149 - $349) and negotiated landmark Medicare coverage ($50/month) to force broad market access against entrenched PBM resistance. However, patients must proactively and strategically manage the restrictive prior authorization and step-therapy protocols erected by cost-conscious self-insured employers. As global production scales unhindered by biologic manufacturing bottlenecks, Foundayo is uniquely positioned to democratize access to GLP-1 therapy worldwide, pending the imminent but slower regulatory approvals of international bodies like the UK's MHRA.