What to Know About the 2026 ADHD Medication Shortage
The nationwide shortage of medications used to treat attention-deficit/hyperactivity disorder (ADHD) has persisted deep into 2026, driven by a complex collision of surging adult diagnoses, stringent regulatory production quotas, and fragile global supply chains. While the supply of non-stimulant medications remains stable, adults and parents of children relying on popular stimulants must navigate intermittent availability by working closely with prescribers to utilize flexible dosing strategies, explore emerging treatments, and leverage independent pharmacy networks.
The Origins and Evolution of the Shortage
The current crisis in ADHD medication access did not emerge overnight. Data published by the American Society of Health-System Pharmacists (ASHP) reveals that nearly 75% of all active drug shortages in the United States actually began in 2022 or earlier, with some persisting for more than five years 12. While the total number of active national drug shortages declined slightly from an all-time high of 323 in early 2024 to 223 by early 2026, medications for ADHD remain among the most severely and consistently impacted 12.
For years, the public narrative surrounding the ADHD medication shortage focused heavily on a pandemic-era surge in telehealth diagnoses. The pandemic did indeed disrupt traditional healthcare delivery, prompting regulatory bodies like the Drug Enforcement Administration (DEA) to temporarily lift certain restrictions, thereby allowing controlled substances to be prescribed via telehealth 3. These waivers have been extended through the end of 2026, removing historical barriers to care and allowing millions of Americans easier access to treatment 3. Consequently, adult ADHD diagnoses have increased dramatically, with recent data indicating that up to 6% of adults in the United States qualified for an ADHD diagnosis in the previous year 3.
However, increased demand is only one facet of the crisis. A recent analysis led by researchers at Yale University, published in the JAMA Health Forum, indicates that the shortage is rooted less in domestic prescribing practices or federal production quotas than in profound global supply chain disruptions 45.
The Fragile Global Supply Chain
The modern pharmaceutical supply chain relies heavily on international partners for active pharmaceutical ingredients (APIs) and key starting materials. Currently, more than 80% of APIs utilized in the United States are produced overseas, predominantly in China and India 6. When global labor shortages, unpredictable shipping delays, or geopolitical tensions impact these overseas manufacturing facilities, domestic production lines grind to a halt 168.
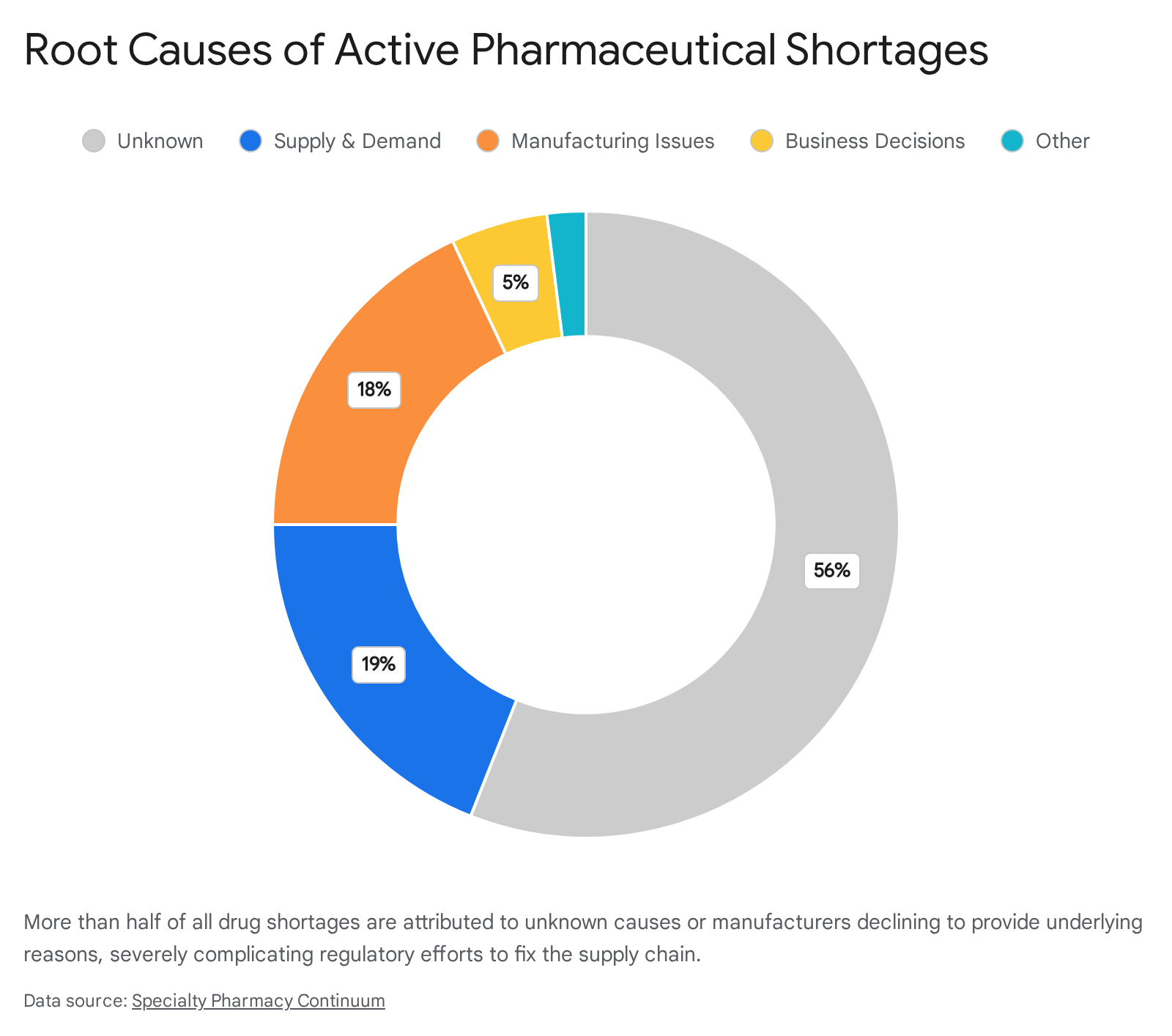
Furthermore, the economic realities of pharmaceutical manufacturing play a significant role. Many of the medications in short supply - particularly generic immediate-release and extended-release stimulants - are off-patent, low-margin products produced by a dwindling number of suppliers 7. Decades of industry consolidation have resulted in a market where a single manufacturing disruption at one facility cannot be easily absorbed by competitors 7. When the University of Utah Drug Information Service tracks the underlying reasons for these shortages, they consistently find that a staggering proportion of the supply chain failures remain completely opaque to both the public and regulatory bodies 10.
DEA Quotas and Regulatory Bottlenecks
Because traditional ADHD stimulants - such as amphetamines and methylphenidate - have a recognized potential for abuse, they are classified as Schedule II controlled substances. As a result, the U.S. Drug Enforcement Administration (DEA) tightly regulates how much of these medications can be produced annually through a system known as Aggregate Production Quotas (APQs) 31112.
For several years, pharmaceutical manufacturers and patient advocacy groups argued that these statutory quotas were set too low to accommodate the rising diagnostic rates, effectively creating an artificial ceiling on supply. In response to mounting pressure and over 5,000 public comments, the DEA implemented significant shifts in January 2026, publishing final APQ orders that raised the production ceilings for several critical stimulant ingredients 11.
The quota for d,l-amphetamine, which serves as the primary component for mixed amphetamine salts (the active ingredient in Adderall and its generic equivalents), was raised by 14.3% to over 24.2 million grams 11. Simultaneously, the quota for lisdexamfetamine, the active prodrug in Vyvanse, was raised by 22% to over 51.2 million grams 11. During this regulatory adjustment, the DEA also explicitly addressed concerns regarding "isomer ratios." Patients had expressed concern that changes in the generic manufacturing process were altering the ratio of dextroamphetamine to levoamphetamine, leading to reports of decreased medication efficacy. The DEA clarified that their quotas do not force a fixed 1:1 isomer ratio, explicitly stating that manufacturers are allocated both racemic mixtures and separate d-amphetamine to achieve the FDA-approved 3:1 ratio 11. This clarification essentially shifted the responsibility for perceived efficacy issues back to FDA quality control and the manufacturing standards of individual pharmaceutical companies 11.
Despite these regulatory victories, raising production quotas does not instantaneously replenish pharmacy shelves. Manufacturers still face internal business constraints, persistent labor shortages in specific production sectors, and rigorous quality control hurdles before the raw APIs can be formulated into finished, distributable capsules 81112.
Tracking and Securing the Pharmaceutical Supply Chain
The structural vulnerabilities exposed by the prolonged ADHD medication shortage have catalyzed massive shifts in how drugs are tracked, traced, and managed throughout the United States and globally. Regulatory bodies and pharmaceutical companies are increasingly relying on advanced technologies to prevent counterfeit medications from entering the market and to gain real-time visibility into supply chain bottlenecks.
Serialization and the DSCSA
At the core of this transformation is the implementation of rigorous "Track and Trace" serialization protocols under regulations like the Drug Supply Chain Security Act (DSCSA) 138. Serialization involves assigning a unique, verifiable digital identity to every single saleable unit of medication 91017. Rather than merely tracking massive pallets of drugs, manufacturers now print unique 2D DataMatrix barcodes on individual cartons 13. These barcodes encapsulate critical information, including the Global Trade Item Number (GTIN), batch or lot number, origin, and expiration date 1011.
As the medication moves from the manufacturing plant, through wholesale distributors, and finally to the local pharmacy, it is continuously scanned 11. This creates an auditable, transparent digital record of the drug's entire journey 13. In pharmacies, this internal safety check ensures that the received medicine is genuine - a critical defense mechanism given the World Health Organization's estimates that nearly 15% of all drugs sold globally are counterfeit 1711. Furthermore, if a quality control issue arises, the track and trace system allows investigators to trace a specific batch backward to its original ingredients or rapidly execute targeted recalls in a fraction of the time traditionally required 13812.
The Role of Advanced Analytics and Blockchain
While serialization drastically improves security, managing the sheer volume of data generated by billions of scanned barcodes presents a formidable technical challenge. Storing this proprietary transaction data in centralized databases has raised cybersecurity and privacy concerns among supply chain partners 8911. To address this, the industry is increasingly exploring decentralized technologies, such as blockchain.
Blockchain technology stores information across a distributed network of computers, creating an immutable, tamper-proof record of transactions 910. A study by Deloitte demonstrated that utilizing blockchain in the pharmaceutical supply chain can reduce the time required to track a product from manufacture to consumption by up to 50%, while a complementary study by Accenture found it could reduce associated logistical costs by up to 30% 9.
Simultaneously, the integration of Artificial Intelligence (AI) and the Internet of Things (IoT) is moving supply chain management from a reactive posture to a predictive one 1321. Advanced AI models can analyze historical supply data, raw material availability, and even public health trends to predict impending shortages before they manifest at the consumer level 1415. For example, AI-driven digital twins - virtual simulations of the manufacturing and distribution process - allow pharmaceutical companies to model different logistical scenarios and optimize their operations to prevent bottlenecks 2116.
Government Initiatives for Supply Chain Resilience
Recognizing that technology alone cannot solve physical shortages of raw materials, the federal government is actively intervening to bolster domestic infrastructure. In April 2026, the Administration for Strategic Preparedness and Response (ASPR), operating under the Department of Health and Human Services (HHS), convened a major Industry Summit focused on the U.S. Medical Manufacturing Industrial Development Strategy 1718.
A primary objective of this summit was to outline strategies for "onshoring" critical manufacturing capabilities 18. By incentivizing the domestic production of APIs and key starting materials, the government aims to reduce reliance on foreign entities. The strategic plan emphasizes the creation of "warm-base" sustainment models - manufacturing facilities that remain operational and can rapidly scale up production capacity during public health emergencies or acute supply chain failures .
Demographic Shifts: The Impact on Pediatric and Adult Care
The medication shortage has highlighted distinct differences in how ADHD is diagnosed and managed across different age demographics, particularly in the wake of the COVID-19 pandemic.
Pediatric Dispensing Trends
Prior to the pandemic, pediatric stimulant use followed predictable seasonal patterns. However, a comprehensive study leveraging data from the IQVIA Longitudinal Prescription Database, which captures 92% of all U.S. prescriptions, revealed significant fluctuations in pediatric care 19. From January 2017 to March 2020, the monthly stimulant dispensing rate to children actually saw a reduction of 18% 19. At the immediate onset of the pandemic, dispensing rates dropped precipitously - likely due to disrupted access to in-person clinical evaluations and the transition to remote schooling, where symptoms of inattention may have been less visible to educators 19.
Following the implementation of telehealth waivers, the rate rebounded 19. Interestingly, when the nationwide shortage of immediate-release mixed amphetamine salts (Adderall) began making headlines in October 2022, the study found that it did not result in a significant drop in children starting or stopping stimulant therapy overall 19. Instead, the shortage forced a shift in prescribing behavior. While the dispensing rate for immediate-release mixed amphetamine salts dropped, there was a compensatory increase in the dispensing of alternative stimulants like dexmethylphenidate and non-stimulants like atomoxetine 19.
The Surge in Adult Treatment
Conversely, the adult demographic has experienced a sustained and unprecedented surge in diagnoses. While pediatricians and child psychiatrists have long-established protocols for diagnosing ADHD, the medical system has historically underdiagnosed the condition in adults 320. With an estimated 15.5 million adults in the U.S. currently diagnosed, adult ADHD is now recognized as the second most common adult psychiatric diagnosis in the country 320.
Despite this prevalence, there remains a critical shortage of clinicians specifically trained in adult ADHD assessment 3. To address this gap in care, organizations like the American Professional Society of ADHD and Related Disorders (APSARD), in partnership with advocacy groups like CHADD, have spent recent years developing comprehensive U.S. Guidelines for the Diagnosis and Treatment of ADHD in Adulthood 3. These guidelines aim to standardize screening, medication management, and psychosocial interventions for adults, ensuring that the growing patient population receives evidence-based care even amidst supply chain constraints 3.
The Current Landscape of ADHD Medications in 2026
When discussing the 2026 medication shortage, it is crucial to understand that not all ADHD treatments are experiencing supply chain failures. The shortages are highly localized within specific classes of stimulant medications, while alternative formulations remain largely available 321.
Stimulants: The Frontline Bottleneck
Stimulant medications - which include the amphetamine and methylphenidate families - work by rapidly increasing the availability of dopamine and norepinephrine in the prefrontal cortex, enhancing focus, motivation, and impulse control 2223. They remain the first-line treatment for the disorder, proving highly effective for roughly 70% to 80% of patients who try them 23. However, this high efficacy and subsequent high demand have placed them squarely at the center of the shortage.
The amphetamine family, which includes mixed amphetamine salts (the active ingredient in Adderall), continues to face severe and widespread supply disruptions 321. According to the FDA's drug shortage database, multiple manufacturers report limited availability extending well into 2026 21. Compounding the issue is that generic formulations are frequently facing more severe backorders than their brand-name counterparts 3. Lisdexamfetamine, a prodrug formulation marketed as Vyvanse, is experiencing intermittent availability, with supply varying wildly depending on the specific dosage strength and the geographic location of the pharmacy 21.
The methylphenidate family, which includes medications like Ritalin and Concerta, is experiencing similar, albeit slightly less severe, disruptions. Manufacturers of methylphenidate extended-release formulations report intermittent backorders for common dosages (18 mg, 27 mg, 36 mg, and 54 mg), citing a combination of manufacturing delays and sudden spikes in demand as patients transition away from unavailable amphetamines 21.
Non-Stimulants: A Stable Alternative
In stark contrast, non-stimulant medications have largely bypassed the current crisis. Because these medications are not classified as controlled substances, their production is not bottlenecked by the DEA's Aggregate Production Quotas 321. Selective norepinephrine reuptake inhibitors like atomoxetine (generic Strattera), alpha-2 agonists like guanfacine (Intuniv), and viloxazine (Qelbree) are consistently available 321. While non-stimulants typically require several weeks of consistent use to reach full therapeutic efficacy - unlike the immediate onset of stimulants - they represent a highly viable and stable alternative for patients struggling to source their usual prescriptions 24.
Overview of Medication Availability
The following table summarizes the status of common ADHD medications amidst the 2026 supply chain disruptions 32123:
| Medication Class | Active Ingredient | Examples (Brand Names) | 2026 Shortage Status | Clinical Notes |
|---|---|---|---|---|
| Stimulant (Amphetamine) | Mixed Amphetamine Salts | Adderall, Adderall XR, Mydayis | Severe Shortage | Generic formulations are heavily impacted; brand names are intermittently available depending on region. |
| Stimulant (Amphetamine) | Lisdexamfetamine | Vyvanse | Intermittent Shortage | Supply varies significantly by dosage strength; active pharmaceutical ingredient sourcing issues persist. |
| Stimulant (Methylphenidate) | Methylphenidate ER | Concerta, Ritalin LA | Intermittent Shortage | Several extended-release generic formulations are frequently on backorder due to manufacturing delays. |
| Non-Stimulant | Atomoxetine | Strattera | Stable Supply | Not subject to DEA quotas; requires continuous dosing to achieve therapeutic effect. |
| Non-Stimulant | Viloxazine | Qelbree | Stable Supply | Widely available; offers an alternative for patients unable to tolerate stimulant side effects. |
| Non-Stimulant | Guanfacine | Intuniv | Stable Supply | Often utilized in conjunction with stimulants or as a standalone option for specific symptom profiles. |
How to Navigate the Shortage: Practical Strategies
Discovering that a vital medication is out of stock can induce significant anxiety, but patients and parents have several proactive strategies at their disposal to navigate the pharmacy landscape in 2026.
Strategic Pharmacy Hunting
When a preferred pharmacy is out of stock, patients are legally permitted to call other pharmacies to inquire about inventory. However, calling exclusively within a single corporate chain (such as only checking various CVS or Walgreens locations) is often inefficient, as these stores typically draw from the same regional distribution centers 825.
Clinical insights from 2026 indicate that independent "mom and pop" pharmacies often possess a distinct advantage 8. These smaller, independent operations frequently contract with different secondary and tertiary regional wholesalers than the major chains, granting them access to medication reserves that larger corporate entities cannot tap into 8.
Patients should be aware that some pharmacies hold strict internal policies against disclosing the inventory of Schedule II controlled substances over the phone, a measure intended to deter drug-seeking behavior and potential theft 25. In these instances, patients may need to visit the pharmacy in person with their identification, or request that their prescribing physician call the pharmacist directly to verify stock 25.
The "Chewable Loophole" and Range Prescriptions
Supply chain data from April 2026 highlighted a unique phenomenon often referred to as the "chewable loophole." While standard adult capsules and tablets of popular stimulants were severely backordered, pediatric formulations - specifically chewable tablets and oral suspensions - showed intermittent to stable availability 8. In response to the crisis, many U.S. insurance providers began granting "Emergency Tier Exceptions," allowing adult patients to access these pediatric formulations or covering the significantly higher cost of brand-name medications when the generic equivalents were unavailable 8.
Furthermore, patients can collaborate with their prescribers to write "range" prescriptions. Because shortages often target specific dosage strengths (e.g., a total depletion of 20 mg tablets), a prescription written with explicit instructions allowing for different dosage forms (such as dispensing two 10 mg tablets in place of one 20 mg tablet) provides the pharmacist with the legal flexibility to fulfill the order using available stock 812.
Medical Bridging: What Are Your Clinical Options?
When a preferred medication is entirely unavailable for an extended period, patients must work closely with their healthcare provider to establish a temporary "bridging" strategy. Medical guidelines universally stress that patients should never start, stop, or arbitrarily adjust the dosage of a psychiatric medication without direct medical supervision 122124.
Transitioning Between Formulations and Families
If a patient's usual extended-release (ER) medication is unavailable, clinical bridging guidelines - such as those adapted by the Australian ADHD Professionals Association (AADPA) and recognized internationally - suggest that an immediate-release (IR) formulation can serve as a highly effective short-term bridge 26. Because IR medications have a shorter duration of action (typically 3 to 4 hours), they require multiple doses throughout the day 2326. For example, a patient stabilized on a 45 mg long-acting methylphenidate capsule might be transitioned to taking a 10 mg immediate-release tablet three times a day to approximate the necessary coverage 26.
Alternatively, a prescriber may opt to switch a patient entirely from the amphetamine family to the methylphenidate family, or vice versa. While both drug classes achieve similar clinical outcomes, their exact mechanisms differ. Amphetamines actively push more neurotransmitters out of storage vesicles into the synapse, whereas methylphenidates primarily block the reuptake transporters, keeping existing neurotransmitters in the synapse longer 23. Because individuals metabolize these drugs differently, cross-tolerance is not perfectly symmetrical, and dosages must be carefully titrated and monitored by the prescriber 2426.
The Risks of "Drug Holidays"
In an attempt to stretch a dwindling prescription, some patients resort to self-initiated "drug holidays," skipping doses on weekends or during periods of lower cognitive demand 812. While planned, medically supervised medication breaks are sometimes utilized in pediatric care to mitigate side effects like growth suppression, abruptly stopping and starting stimulant medication in adults can be destabilizing. For many individuals, erratic dosing can trigger severe withdrawal-like fatigue, mood swings, emotional dysregulation, and intense cognitive "brain fog" 826.
New Treatments on the Horizon in 2026
Amidst the frustration of the ongoing shortage, the pharmaceutical pipeline is offering highly anticipated new options. The U.S. Food and Drug Administration (FDA) has accepted and is currently conducting a priority review of a New Drug Application (NDA) for a novel ADHD medication called centanafadine, developed by Otsuka Pharmaceutical 2027282930. The target action date under the Prescription Drug User Fee Act (PDUFA) is set for July 24, 2026 20272829.
The Promise of Centanafadine
If approved, centanafadine would represent a significant paradigm shift in psychiatric pharmacology, becoming the first-in-class norepinephrine, dopamine, and serotonin reuptake inhibitor (NDSRI) 27282930. Unlike traditional stimulants that primarily target dopamine and norepinephrine, centanafadine's tri-monoamine modulation is designed to address a broader spectrum of symptoms, including emotional dysregulation and comorbid anxiety, which frequently accompany adult ADHD 28.
The clinical profile of centanafadine has been rigorously evaluated in multiple Phase 3 trials and subsequent Matching-Adjusted Indirect Comparisons (MAICs) against existing market leaders 2028313233. The data presents a compelling alternative for the future:
- Efficacy: Centanafadine demonstrates statistically significant and clinically meaningful improvements in core ADHD symptoms compared to a placebo 272829. When compared directly to existing non-stimulants like atomoxetine, it shows comparable efficacy 3132. However, MAIC data indicates it provides a slightly smaller overall reduction in symptom severity when compared head-to-head against highly potent stimulants like lisdexamfetamine 313233.
- Safety and Tolerability: Where centanafadine truly excels is its side-effect profile. Long-term safety data reveals that patients taking centanafadine experience significantly lower rates of severe side effects compared to those on traditional stimulants. Specifically, the data shows statistically significant reductions in the risk of severe appetite loss, dry mouth, insomnia, headache, and medication-induced anxiety when compared to both lisdexamfetamine and methylphenidate 313233.
- Abuse Liability and Scheduling: Perhaps most relevant to the current crisis is centanafadine's performance in Human Abuse Liability (HAL) testing. Clinical data suggests that when doses are pushed beyond the therapeutic range, subjects experience an acute onset of aversion and negative effects, indicating a distinctly lower potential for recreational abuse 283234. Experts suggest that if this profile holds, centanafadine could qualify for less restrictive DEA scheduling than the Schedule II classification that currently throttles stimulant production quotas 34.
Bottom line
The 2026 ADHD medication shortage is the culmination of a deeply interconnected crisis, driven by a surge in adult diagnoses, rigid DEA production quotas, and vulnerabilities within the global pharmaceutical supply chain. While legislative efforts to raise quotas and technological advances in supply chain tracking are underway, immediate relief remains elusive for many patients reliant on generic extended-release stimulants. However, by collaborating closely with prescribers to explore flexible dosing, utilizing bridging strategies with immediate-release or non-stimulant medications, and anticipating the approval of novel treatments like centanafadine, individuals can secure continuous care despite the broader systemic disruptions.