Anxiety, Depression and Treatment Gaps in 2026
By 2026, mental health conditions have cemented their status as the defining global public health challenge of our era, with over one billion people living with a diagnosable disorder. Despite unprecedented cultural awareness and demand for psychological support, a severe shortage of mental health professionals and deceptive insurance practices have left nearly half of those affected without treatment. While digital therapeutics and telepsychiatry offer scalable solutions, the fundamental gap between clinical need and accessible care remains dangerously wide.
The Scope of the Global Mental Health Crisis
Mental health is no longer a peripheral medical topic; it is central to global healthcare strategy. Current data reveals that psychological distress is pervasive across all geographic boundaries, age brackets, and socioeconomic strata. The World Health Organization (WHO) estimates that roughly one in eight people worldwide is living with a mental health disorder 123. The onset of the COVID-19 pandemic triggered a massive 25% surge in the global prevalence of anxiety and depression 45. While the acute phase of the pandemic has passed, longitudinal data indicates that this elevated baseline of emotional burnout, chronic anxiety, and social withdrawal has largely become permanent 56.
Anxiety and depressive disorders are the absolute drivers of this global burden. According to the Global Burden of Disease (GBD) 2021 study, which analyzed trends from 1990 to 2021, the global prevalence of anxiety disorders reached 359.2 million cases, accounting for a massive 18.2% increase in its age-standardized disability-adjusted life year (DALY) rate 4. Depressive disorders followed closely, affecting an estimated 332.4 million people worldwide, marking a 13.4% increase in DALY rates over the same period 4. Forecasts using autoregressive integrated moving average models project that by 2040, global cases will surpass 515 million for anxiety and 466 million for depressive disorders 4.
In the United States, the statistics mirror these global surges but reflect an even higher concentration of documented clinical diagnoses. Data from the 2024 National Survey on Drug Use and Health (NSDUH), released by the Substance Abuse and Mental Health Services Administration (SAMHSA) in 2025, revealed that 23.4% of U.S. adults - equivalent to 61.5 million people - experienced a mental health condition in the past year 85. Anxiety disorders are the most common psychiatric hurdle in America, affecting over 42.5 million adults annually, which equates to roughly 19.1% of the adult population 106.
Demographic Disparities: Who is Most Affected?
The burden of mental illness is not distributed equally. Extensive research highlights stark demographic disparities, particularly regarding age and sex. Women are significantly more likely to be diagnosed with both anxiety and depressive disorders than men. Epidemiological studies estimate that women experience depression at roughly twice the rate of men, a disparity attributed to a complex interplay of hormonal factors, higher rates of reported trauma and violence, and socioeconomic pressures 1078. For anxiety, women are approximately 1.6 times more likely to be affected, with 23.4% of women reporting anxiety symptoms in the past year compared to 14.3% of men 6. However, researchers note that cultural stigma often leads to underreporting among men, making advocacy and destigmatization crucial for accurate diagnosis .
The age distribution of mental health conditions also reveals a shifting landscape. Historically, mental health interventions focused heavily on adults, but contemporary data proves that psychological distress takes root early. Half of all mental health conditions begin by age 14, and 75% develop by age 24 410. Young adults aged 18 to 25 currently carry the highest burden of mental health conditions among all adult age groups, with over 36% reporting symptoms 88. Furthermore, younger adults aged 20 to 29 have shown the largest increases in prevalence over the past decade 39.
To understand the specific landscape of these conditions, it is helpful to look at how they distribute across the population.
| Mental Health Condition | Global Prevalence | U.S. Adult Prevalence (Past Year) | Key Characteristics & Trajectories |
|---|---|---|---|
| Anxiety Disorders | ~359 million (4.05%) | 19.1% (42.5 million) | Includes generalized anxiety, social anxiety, and panic disorders. The incidence has surged by 52% among youth since 1990 46. |
| Major Depression | ~332 million (5.0%) | 8.3% (21 million) | The leading contributor to disability worldwide. Strongly correlated with economic instability, trauma, and isolation 78. |
| Post-Traumatic Stress (PTSD) | ~3.9% | 5.0% | Often untreated in marginalized communities. Driven by exposure to violence, severe accidents, and childhood trauma 48. |
| Bipolar Disorder | ~40 million | 2.8% | Characterized by severe mood swings. Affects 1 in 150 adults globally and is associated with reduced life expectancy 348. |
| Schizophrenia | ~24 million | 1.2% | Affects roughly 1 in 300 adults. Requires the most intensive, lifelong psychiatric management and community support 348. |
The Economic and Societal Toll
Mental illness is not solely a healthcare challenge; it is a macroeconomic crisis. The economic impact of untreated mental health disorders is staggering. The World Health Organization estimates that depression and anxiety alone cost the global economy approximately $1 trillion each year 45. Other estimates from corporate health analyses suggest the total global economic cost could reach up to $3 trillion annually by 2025, driven primarily by lost productivity, absenteeism, and an estimated 14 billion lost workdays 2.
Beyond the financial metrics, the societal cost is measured in life expectancy and mortality. People living with severe mental illnesses, such as schizophrenia or bipolar disorder, experience mortality rates over twice as high as the general population, largely due to untreated co-occurring physical health conditions and reduced social support 10. Tragically, suicide remains a devastating outcome of untreated psychiatric distress. In 2021, suicide claimed an estimated 727,000 lives globally, standing as a leading cause of death among young people across all socioeconomic contexts 1. In the United States, over 49,000 people died by suicide in 2023, and roughly 14.3 million adults reported having serious thoughts of suicide in 2024 810. Despite these grim statistics, global progress in reducing suicide mortality remains far too slow to meet the United Nations Sustainable Development Goal of a one-third reduction by 2030 1.
Diagnosing the Global Treatment Gap
Raising public awareness about the prevalence of mental health conditions has been a vital achievement of the past decade. However, awareness alone does not heal; clinical intervention does. Global health organizations track the "treatment gap," which measures the vast chasm between the number of people who experience a psychological disorder and the number who actually receive adequate, evidence-based care.
The reality of this gap is bleak. A landmark study published by researchers from the University of British Columbia and Harvard Medical School analyzed survey data from nearly 57,000 participants across 21 countries to map the exact points where patients fall out of the healthcare pipeline. The findings were stark: globally, only about 6.9% of people who meet the criteria for a mental health or substance-use disorder receive minimally effective treatment 11.
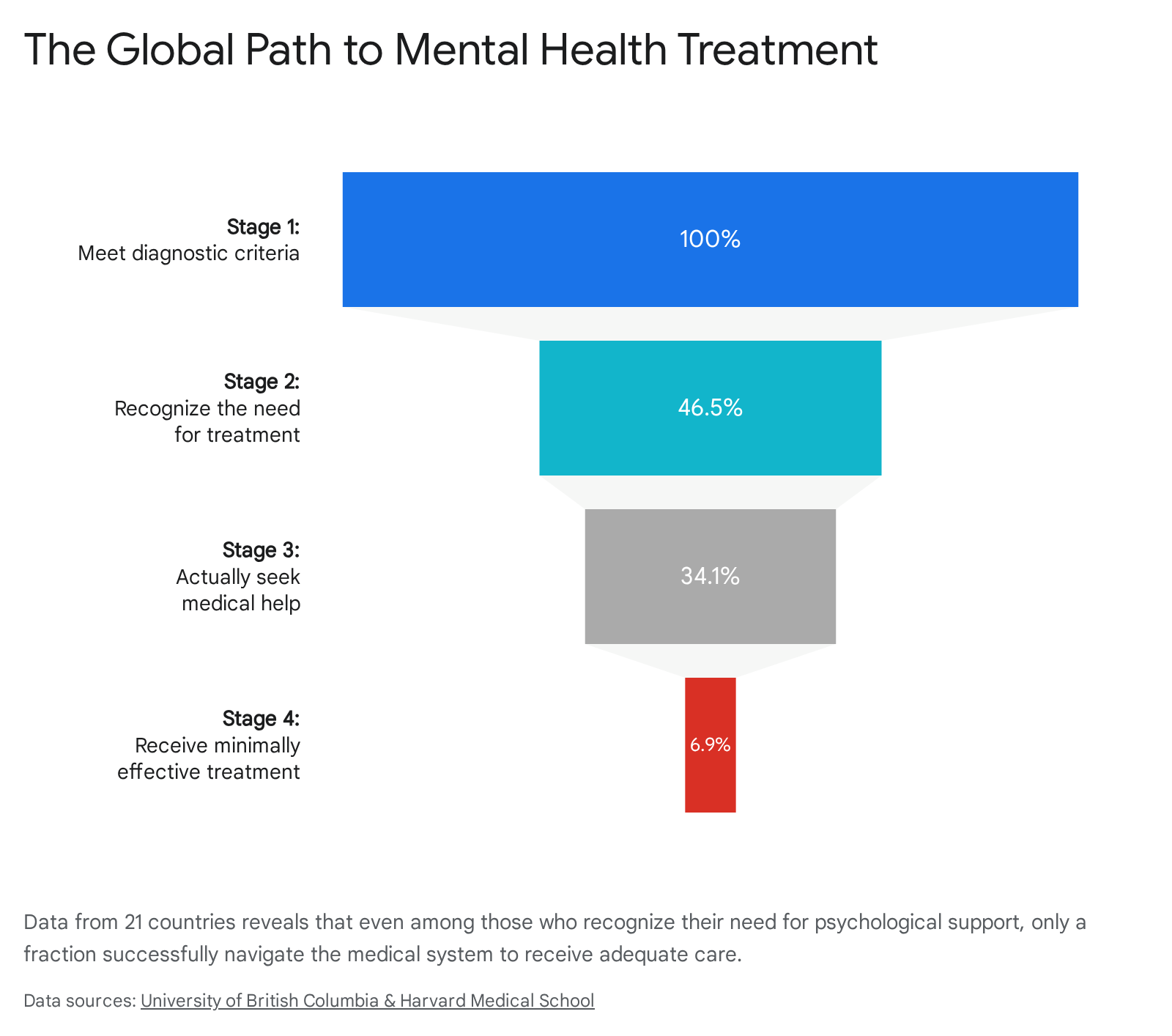
The barriers to care are multilayered. The study noted that the single largest hurdle is a lack of recognition; only 46.5% of individuals with a disorder recognized their own need for treatment 11. Even among those who did recognize their distress, only 34.1% reached out to the medical system for help, often deterred by social stigma, fear of clinical environments, or a lack of mental health literacy 211. Finally, of those who successfully sought help, less than half received care that met the minimum standards for clinical effectiveness 11.
Geographic Inequities: High-Income vs. Low-Income Nations
The nature of the treatment gap changes drastically depending on a nation's wealth and infrastructure. In low- and middle-income countries (LMICs), the gap is driven by a profound absolute lack of resources. The WHO's 2024 Mental Health Atlas reveals that median global government expenditure on mental health remains frozen at just 2.1% of total health budgets 3. The disparities within this figure are extreme. While high-income countries spend an average of nearly $66 per capita on mental health services, low-income nations spend as little as $0.04 per person 37.
Because of this chronic underfunding, fewer than 10% of affected individuals in low-income countries receive any formal care 1. In these regions, community-based care is virtually nonexistent. Over 60% of psychiatric inpatient beds remain in large, centralized psychiatric hospitals, where admissions are frequently involuntary and lengths of stay can stretch for years 13. Out-of-pocket expenses for vital mental health medications frequently push households into poverty in developing nations, further deterring people from seeking help 4.
In high-income countries like the United States, the infrastructure exists, yet access remains deeply flawed. The 2024 NSDUH data shows that nearly 48% of American adults with a mental illness received no treatment 81812. For those grappling with co-occurring mental health and substance use disorders, the statistics are even more dire: only 14.5% received treatment for both conditions, while over 41% received treatment for neither 8. When surveyed, Americans consistently cite the high cost of care, an inability to find available providers, and restrictive insurance barriers as the primary reasons they abandon treatment 818.
Wait Times Across Universal and Private Systems
When individuals do seek help, they are frequently met with crippling wait times. Mental healthcare is highly time-sensitive; a patient reaching out to a psychologist is often experiencing an acute emotional crisis. Delays in care allow conditions to worsen, compounding psychological distress and increasing the risk of self-medication through substance use.
Wait times are a universal friction point, plaguing both privatized insurance markets and publicly funded single-payer systems.
| Country | Healthcare Model | Average Mental Health Wait Times / Access Metrics |
|---|---|---|
| United States | Privatized / Mixed | National average wait time for behavioral health is 48 days. Median wait for psychiatric evaluation is 67 days in-person (43 days via telehealth) 1213. |
| United Kingdom | Universal (NHS) | Patients are 8 times more likely to wait over 18 months for mental health care than for physical elective care. Over 16,500 people are waiting over 18 months 1314. |
| Australia | Universal (Medicare) | Mean wait times for adolescents reach 100 days for psychologists and 127 days for psychiatrists. 85% of patients deem waits "too long" 15. |
| Canada | Universal (Medicare) | Psychiatric wait times frequently exceed six months in multiple provinces, leading to high utilization of emergency departments 16. |
In the U.S., wait times are heavily influenced by geography and provider type. An analysis of social workers and therapists found that the most common wait time for a new client is two to four weeks, but specialized psychiatric care can take months 17. In rural areas, patients face wait times up to three times longer than their urban counterparts, with many rural counties offering zero local access to psychiatric care within a 100-mile radius 18.
The Workforce Shortage Bottleneck
The primary structural cause of these wait times is a massive deficit in human capital. The global psychiatric and psychological workforce is not large enough to meet the current demand, let alone the projected future needs.
The WHO reports a global median of just 13 mental health workers per 100,000 people. While high-income nations boast an average of 67 workers per 100,000 population, low-income nations frequently have only one or two 13. Two-thirds of WHO Member States report having just a single psychiatrist to serve 200,000 or more people 9.
In the United States, the sheer scale of the shortage is difficult to overstate. As of late 2025, over 137 million Americans - approximately 40% of the entire U.S. population - live in federally designated Mental Health Professional Shortage Areas (HPSAs) 1218. This deficit spans every discipline, from clinical psychologists to licensed clinical social workers, and heavily impacts the availability of prescribers.
Projecting the Clinician Deficit
The workforce crisis is expected to intensify substantially. The U.S. Health Resources and Services Administration (HRSA) projects that demand for behavioral health services will increase by 49% by the early 2030s, fueled by diminishing stigma, the lingering effects of the pandemic, and an aging population with growing psychological needs 1812. Conversely, the supply of mental health professionals is projected to grow by only 11% over the same period 18.
Federal workforce projections indicate that by 2037 and 2038, the U.S. will face critical shortfalls across nearly every sub-specialty. Estimates suggest a coming deficit of roughly 88,000 to 100,000 mental health counselors, over 114,000 addiction counselors, and tens of thousands of adult and child psychiatrists 181927. Because the demand growth is outpacing supply growth by a factor of nearly 4.5 to 1, reversing this trend will require massive systemic interventions in educational funding, clinical training pipelines, and provider reimbursement rates 27.
The Toll on Mental Health Professionals
The lack of available clinicians creates a brutal feedback loop for the professionals currently working in the system. Mental health providers globally are facing unsustainable caseloads, leading to high rates of emotional exhaustion and burnout.
In the United Kingdom, over 70% of mental health professionals report severe emotional exhaustion, driving high turnover rates 16. In Australia, rural mental health practitioners are struggling under the weight of compounding crises, relying heavily on emergency telehealth services to manage their sprawling territories 16. In the U.S., six in ten clinical psychologists report that they are no longer accepting new patients, completely capping their practice capacity to protect their own mental well-being and maintain the quality of care for existing clients 1218. Furthermore, low reimbursement rates from insurance companies actively discourage clinicians from taking insurance, pushing many into cash-only private practices, which further limits access for lower-income populations 19.
Navigating the "Ghost Network" Crisis
Even when a patient has health insurance that theoretically provides mental health benefits, they frequently run into an invisible wall: the "ghost network."
A ghost network occurs when a health insurance company publishes a provider directory detailing the psychologists, psychiatrists, and therapists who are ostensibly "in-network," only for the patient to discover that these lists are full of unreachable or unavailable practitioners. Patients seeking help often spend hours calling numbers only to find disconnected lines, doctors who retired years ago, clinicians who have moved out of state, or providers whose practices are entirely full 192021.
The Anatomy of a Bureaucratic Maze
In October 2025, the U.S. Department of Health and Human Services (HHS) Office of Inspector General released a damning report quantifying the scale of this deception. Investigating a nationally representative sample of 40 private Medicare Advantage plans and 20 Medicaid managed care plans across multiple states, the watchdog found systemic inaccuracies.
The investigation revealed that an astonishing 55% of the mental health professionals listed as in-network by Medicare Advantage plans were not actually providing care to any of those plans' members 222332. For Medicaid plans, 28% of the directories were inaccurate 2232. Federal investigations paint a grim picture of this bureaucratic maze, where over half of the mental health professionals listed in some private directories are entirely unreachable, effectively functioning as empty silhouettes fading from the system. In one particularly glaring instance, a provider was listed at 19 different clinic locations despite having retired several years prior 2223.
Why do ghost networks exist? The U.S. healthcare model heavily incentivizes them. Insurance companies are paid hundreds of billions of dollars annually by the government to manage Medicare and Medicaid populations. They are legally required to maintain "network adequacy" - proving they have enough contracted doctors to serve their patient pool 2223. However, by failing to audit and clean their directories, insurers can maintain the illusion of a massive, robust network on paper while systematically suppressing the utilization of behavioral health benefits in practice. When patients give up trying to find a doctor, the insurer saves money. Enforcement of federal parity laws has simply not kept pace with these compliance gaps 1932.
Practical Strategies for Patients
For a patient already struggling with severe depression or anxiety, the friction of navigating a ghost network is often enough to make them abandon the search entirely. However, advocates recommend several strategies to bypass these dead ends:
- Leverage Third-Party Tools: Rather than relying solely on outdated insurance PDFs, patients are encouraged to use specialized, frequently updated databases like Psychology Today, Zencare, or Mental Health Match, which allow users to filter by specific insurance plans and exact current availability 2133.
- Seek Sliding Scale Clinics: For those who cannot find an in-network provider, many community mental health centers and non-profit collectives (such as the Open Path Psychotherapy Collective) offer income-based sliding scale fees. These models adjust the cost of therapy - often down to $30 or $60 a session - based on a patient's financial need 2435.
- Explore Out-of-Network Benefits: Many insurance plans offer partial reimbursement for out-of-network providers. While this requires the patient to pay upfront and submit a "superbill" for reimbursement, it vastly widens the pool of available therapists 21.
Decoding the Youth Mental Health Emergency
While psychological distress is rising across all age groups, the burden on adolescents and young adults has reached emergency levels. Between 1990 and 2021, the incidence of anxiety among individuals aged 10 to 24 skyrocketed by 52% 6. The U.S. Centers for Disease Control and Prevention (CDC) recently noted that over 40% of high school students report persistent feelings of sadness or hopelessness, with 53% of female high school students experiencing these symptoms in 2023 612.
Children and teenagers today are shouldering an unprecedented psychological load. Clinical experts attribute this to a perfect storm of systemic factors: intense academic pressure, economic anxiety inherited from their parents, the trauma of the pandemic disrupting crucial social developmental milestones, and the omnipresent influence of the digital world 56.
Does Smartphone Use Actually Cause Depression?
The most fiercely debated question in developmental psychology is the exact relationship between the rise of the smartphone and the collapse of adolescent mental health. While many parents and pundits assert a direct cause-and-effect relationship - that screens actively create sadness - the scientific literature suggests a highly complex, bidirectional mechanism.
There is substantial evidence that heavy digital media use corresponds with poorer developmental outcomes. A major global study tracking over 100,000 young adults found that receiving a first smartphone before the age of 13 is strongly associated with poorer "mind health" in adulthood. Early smartphone owners were significantly more likely to report suicidal thoughts, aggression, and low self-worth. The researchers concluded that roughly 40% of this association is mediated by early access to social media, which acts as a gateway to cyberbullying, poor family relationships, and disrupted sleep 36.
Recent longitudinal research strengthens the argument that social media acts as a catalyst for distress. A 2025 study published in JAMA analyzed data from nearly 12,000 children over a three-year period. The researchers found a unidirectional relationship: when an adolescent increased their time spent on social media beyond their usual baseline, it significantly predicted an increase in depressive symptoms a year later 25. Crucially, the researchers found no evidence for the reverse scenario. Preexisting depressive symptoms did not lead to increased social media use, directly challenging the notion that depressed teens simply use phones as a coping mechanism to self-soothe 25.
A massive meta-analysis published in JAMA Pediatrics echoed these concerns, finding that social media engagement is consistently linked with multiple social-emotional difficulties, with the strongest negative associations observed during early adolescence - a critical window of brain development 38.
The Mechanism: Sleep Disruption and "Problematic Use"
How exactly does a screen translate into anxiety? Researchers from Imperial College London conducted the SCAMP study, tracking thousands of adolescents to uncover the mechanism. They found that teenagers who used social media for more than three hours a day were significantly more likely to develop symptoms of depression and anxiety 26. However, they noted that the effect is not inherently tied to the content itself; rather, it is driven heavily by sleep disruption. Heavy social media use, particularly late into the evening, drastically reduces sleep duration and quality, which in turn causes lasting physiological impacts on emotional regulation 26.
However, the scientific community is not entirely unified on unidirectional causation. A 2024 study led by researchers at Johns Hopkins Children's Center provided a nuanced counterpoint. Their data suggested that social media use did not intrinsically predict an increase in depressive symptoms over time. Instead, they found that "if you tended to be a person who was depressed, you were a person also spending more time on social media" 27. They highlighted that high digital consumption rarely happens in a vacuum; it is often part of a broader lifestyle cluster that includes a lack of physical exercise, staying up late ("eveningness"), cannabis use, and a lack of exposure to outdoor green spaces 27.
Ultimately, the consensus among psychiatrists revolves around the concept of "problematic smartphone use" (PSU). Rather than labeling all screen time as toxic, clinicians look for behavioral addiction markers. PSU is defined by a subjective loss of control, where a teenager neglects real-world responsibilities, abandons meaningful hobbies, and experiences intense emotional discontent, anxiety, or distress when disconnected from their devices 2829. When a child's relationship with technology mirrors addiction, the psychological consequences are severe.
Telehealth and the Digital Therapy Revolution
Facing a historic clinician shortage and overwhelming demand, the healthcare industry has increasingly turned to technology to scale mental health interventions. Telepsychiatry and digital therapeutics (mental health apps) underwent a massive expansion during the pandemic and have now solidified as permanent pillars of global psychiatric care.
The Efficacy of Video-Delivered Psychotherapy
When teletherapy first emerged, many traditional clinicians were highly skeptical. The core of effective psychotherapy is the "therapeutic alliance" - the profound trust, empathy, and connection forged between a patient and provider. Many questioned whether this vital human element could translate across a video screen.
Extensive research has now definitively answered that question. A landmark 2024 systematic review and meta-analysis published in the Canadian Medical Association Journal (CMAJ) analyzed decades of randomized controlled trials comparing video-delivered cognitive behavioral therapy (CBT) to traditional in-person CBT. The conclusion was unambiguous: remote, therapist-guided video sessions are statistically equivalent to in-person therapy in effectively reducing the target symptoms of major depressive disorder, PTSD, OCD, and panic disorder 30.
Further studies in Frontiers in Psychology confirmed that patients in teletherapy rapidly build a strong clinical presence and report feeling just as understood and connected to their remote therapists as they do in physical offices 30. Telepsychiatry has also revolutionized psychiatric medication management, allowing patients in rural areas to bypass local shortages and receive vital prescriptions. Today, an estimated 73% of employers offer virtual mental healthcare access as a core employee benefit, and the vast majority of commercial insurance plans have mandated telehealth coverage 30.
Evaluating the $45 Billion Mental Health App Market
While teletherapy connects a patient to a human doctor via a screen, "digital therapeutics" replace the human entirely with software. The global digital mental health market is experiencing explosive growth, projected to exceed $45 billion by 2026, with over 20,000 distinct mental health apps available for download 4445.
These mobile health (mHealth) applications range from simple meditation guides and mood trackers to highly sophisticated AI-driven chatbots that deliver structured CBT exercises. Recent innovations include the integration of wearable technology - smartwatches that monitor physiological indicators of stress, like heart rate variability, and prompt the user to engage in breathing exercises before a panic attack sets in 45.
Do these apps actually work? The clinical evidence is mixed and highly dependent on the severity of the patient's condition.
Systematic reviews indicate that app-based interventions have an established, proven efficacy in the self-management of mild to moderate depression and anxiety 31. Chatbots like Wysa or Woebot are highly effective at teaching users CBT-based coping skills, acting as "guided self-help" to intercept negative thought spirals 44. In clinical trials where apps were used to support mental health nursing care, patients showed significant improvements in medication adherence and symptom reduction 47.
However, the limitations of software are stark. Research shows that apps produce highly mixed or poor results when applied to severe clinical conditions, such as severe mood disorders, schizophrenia, psychosis, eating disorders, and active substance use disorders 31. In some trials involving people with severe mental illness, relying purely on apps without human oversight led to deterioration and adverse events 31.
The consensus among psychiatric experts in 2026 is that technology is best utilized as an augmentation tool, not a total replacement for human care. Apps are excellent for extending a therapist's reach between sessions, providing scalable psychoeducation, or offering a stopgap for patients languishing on 100-day waitlists. But for deep, complex, and transformative psychological healing, the nuanced connection of a human therapeutic alliance remains irreplaceable 44.
Bottom line
The global mental health landscape in 2026 is characterized by a stark paradox: the world possesses an unprecedented understanding of psychological disorders and highly effective clinical tools, yet the fundamental infrastructure required to deliver that care remains broken. Millions of individuals are caught in a massive treatment gap, bottlenecked by a severe global shortage of psychiatric professionals and obstructed by the bureaucratic deception of insurance ghost networks. While innovations in telepsychiatry and digital health applications are providing vital, scalable lifelines - especially for mild to moderate anxiety and depression - they cannot independently resolve the systemic underfunding of public mental health, leaving governments and healthcare systems with an urgent mandate to aggressively expand the human clinical workforce.