How GLP-1s Change Your Gut Microbiome Week by Week
When you start a glucagon-like peptide-1 (GLP-1) medication, your gut microbiome undergoes a profound, gradual transformation driven by slower digestion, reduced food intake, and shifts in gut chemistry. Within the first few weeks, the altered intestinal environment reshapes your microbial populations, often increasing beneficial, metabolism-regulating bacteria while reducing inflammation-associated strains. These microbial shifts not only help explain the gastrointestinal side effects many users experience but may also play a crucial role in determining how much weight you ultimately lose.
The Invisible Engine of Weight Loss
Glucagon-like peptide-1 receptor agonists - such as semaglutide, liraglutide, and tirzepatide - have fundamentally altered the modern management of obesity and type 2 diabetes. By mimicking a naturally occurring incretin hormone, these medications stimulate glucose-dependent insulin release, suppress the hormone glucagon, and signal profound satiety to the brain 12. However, the global conversation around these medications frequently overlooks the bustling, microscopic ecosystem residing exactly where the natural hormone is produced: the gastrointestinal tract.
Your gut microbiome consists of trillions of bacteria, viruses, and fungi that break down food, regulate immune responses, and produce metabolic signaling molecules. For years, scientists have understood that obesity and metabolic dysfunction are heavily linked to gut dysbiosis, which is an imbalance where inflammatory microbes outnumber beneficial, diverse ones 33. When individuals possess a healthy, highly diverse microbiome, they generally exhibit better glucose tolerance, lower systemic inflammation, and a more robust intestinal barrier. Conversely, individuals living with obesity or type 2 diabetes often present with a less diverse microbial profile that is highly efficient at extracting excess calories from the diet and promoting fat storage.
Recent clinical and preclinical data reveal that GLP-1 medications and the gut microbiome operate on a highly dynamic, bidirectional street.
The drugs fundamentally alter the physical and chemical environment in which your gut bacteria live, essentially forcing the microbiome to adapt and reshape itself to survive. Concurrently, the specific strains of bacteria you harbor before you even take your first injection may dictate how well you tolerate the medication, the severity of your gastrointestinal side effects, and how effectively the drug lowers your blood sugar and body weight over the long term 45.
The Biological Baseline: How Your Gut Makes Its Own GLP-1
To fully understand what happens when you introduce a synthetic GLP-1 receptor agonist into your body, it is essential to first understand how your body produces this exact same hormone naturally.
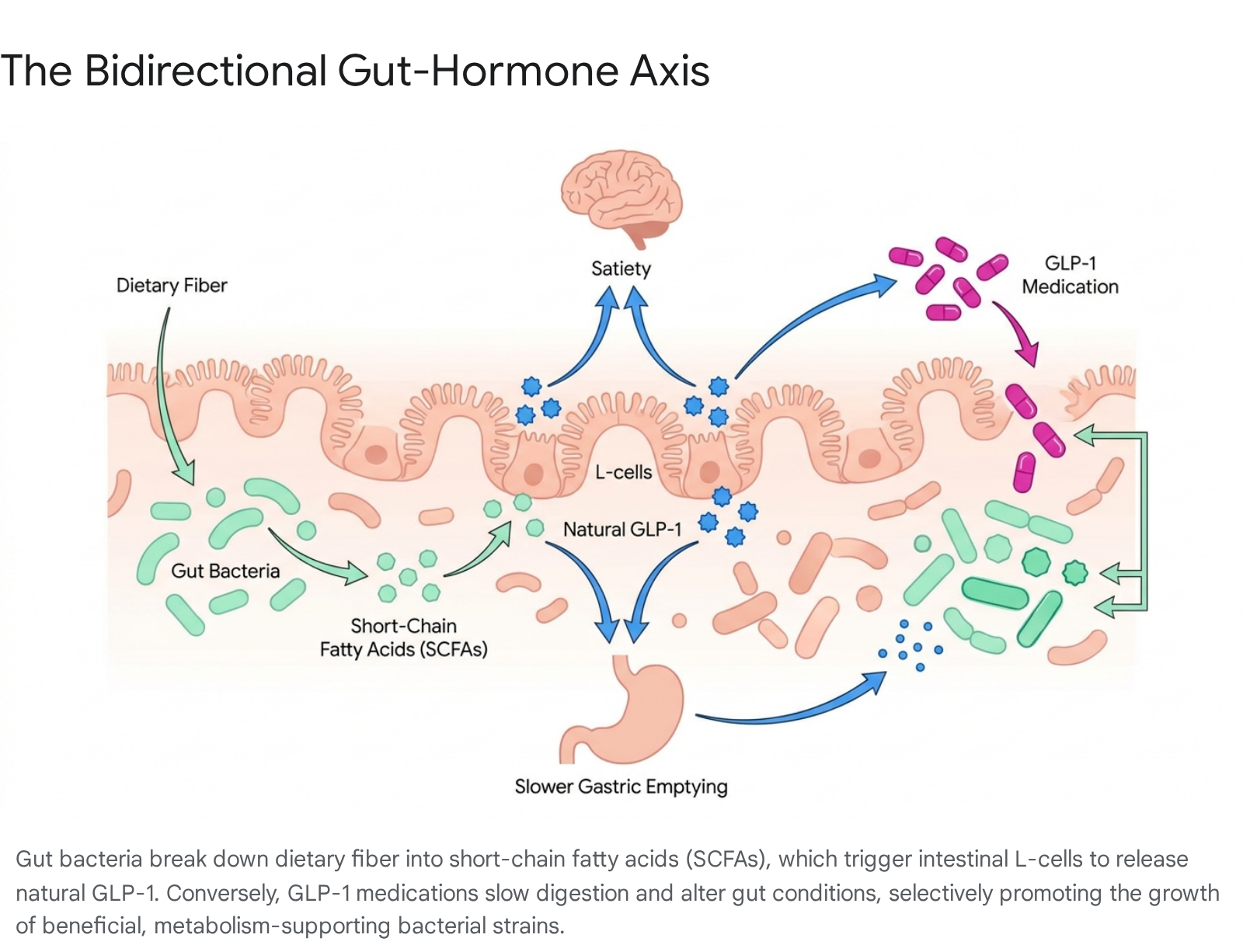
Endogenous, or natural, GLP-1 is secreted primarily by specialized cells in the lining of the distal small intestine and the colon, known as enteroendocrine L-cells 46. These L-cells act as sophisticated biological and chemical sensors that monitor the environment of the gut lumen. When you consume dietary fiber - specifically complex carbohydrates that human digestive enzymes cannot break down - it travels relatively intact to the lower intestine. There, your resident gut microbes ferment this fiber. This bacterial fermentation process produces highly beneficial metabolic byproducts called short-chain fatty acids, primarily butyrate, propionate, and acetate 47.
These short-chain fatty acids bind directly to specific G-protein-coupled receptors, particularly GPR41 and GPR43, which are located on the surface of the intestinal L-cells. This binding acts as a chemical signal, effectively instructing the L-cells to release natural GLP-1 into the bloodstream 469. Once released, the hormone travels to the pancreas to boost insulin production in response to glucose, and simultaneously travels to the brain to signal that you have eaten enough. In individuals with healthy, diverse microbiomes, this signaling loop is robust, efficient, and finely tuned to prevent overeating and maintain blood sugar stability.
However, in individuals living with metabolic dysfunction or obesity, this elegant system is frequently broken. Dysbiosis, characterized by a lack of microbial diversity and an overgrowth of inflammatory bacterial species, impairs this natural signaling. Harmful bacteria produce increased levels of inflammatory molecules, such as lipopolysaccharides, which can activate immune receptors like Toll-like receptor 4. This triggers an inflammatory cascade that blocks the GLP-1 signaling pathways, reduces the sensitivity of insulin receptors, and worsens systemic insulin resistance 410. Furthermore, when the gut lacks the specific bacterial strains responsible for fermenting fiber into short-chain fatty acids, the L-cells do not receive the necessary chemical prompts to release natural GLP-1, leaving the individual feeling constantly hungry and struggling with erratic blood sugar levels.
When you take a prescription GLP-1 medication, you are introducing a long-acting, synthetic version of this hormone that has been pharmacologically engineered to resist immediate breakdown by the body's natural enzymes, specifically the dipeptidyl peptidase-4 enzyme 8. The medication forcefully activates the satiety and insulin-regulating pathways that dysbiosis and metabolic disease may have blunted. But the drug's effects do not simply stop at the receptors in the brain and pancreas. It initiates a massive domino effect of physical changes in the digestive tract that inevitably forces the microbiome to evolve and adapt.
Week One and Two: Gastric Emptying and The Initial Shock
The transformation of the gut microbiome on a GLP-1 medication is a gradual process of ecological succession, much like a forest adapting to a sudden change in climate. It requires time to adjust to radical changes in food supply, transit speed, and the chemical environment of the intestines.
When you take your first dose of a GLP-1 medication, the most immediate physiological change in the gastrointestinal tract is a pharmacological delay in gastric emptying. The stomach retains food much longer than usual, releasing it into the small intestine at a slow, controlled trickle rather than a rapid rush 112. For the microbiome, which relies entirely on the host's eating and digestive patterns for its survival, this represents a seismic environmental event.
Food staying in the stomach and small intestine longer gives bacteria significantly more time to interact with nutrients 13. However, it also fundamentally changes the pH balance and the predictable timing of nutrient availability in the lower gut. Fast-fermenting bacteria that have evolved to thrive on rapid, frequent influxes of simple sugars suddenly find their food supply heavily rationed and delayed 813.
During these first seven to fourteen days, the overall structural diversity of the microbiome may not look vastly different on a macro scale, but the local environment is in turmoil 910. This period of ecological disruption correlates perfectly with the peak of gastrointestinal side effects reported by patients. As bacterial populations begin to scramble for resources in a slower-moving digestive tract, the normal processes of digestion become highly unpredictable.
As gastric emptying slows down, food ferments longer in the upper portions of the gastrointestinal tract. This prolonged fermentation often produces excess gas, leading to the severe bloating, belching, and nausea that are the hallmark side effects of early dose titration 16. At the same time, the altered transit speed wreaks havoc on bowel habits. Many patients experience severe constipation because the slower transit time allows the colon to absorb much more water from waste than usual, creating hard, difficult-to-pass stools. The beneficial bacteria that normally produce metabolites to stimulate healthy intestinal motility are temporarily disrupted by the new environment 813. Conversely, some patients experience sudden bouts of diarrhea as the gut attempts to flush out the rapidly shifting bacterial byproducts and unabsorbed bile acids.
For most patients and their prescribing clinicians, distinguishing between normal microbial adjustment and severe drug intolerance is a critical task during this phase. Mild to moderate bloating or a shift in bowel frequency is to be expected as the ecosystem adjusts; however, severe, persistent vomiting or signs of bowel obstruction require immediate medical intervention and potential discontinuation of the drug 1611.
Week Three and Four: Dietary Shifts and Microbial Adaptation
By the third and fourth weeks of treatment, as the patient continues through the dose escalation protocol, the medication's central appetite-suppressing effects typically become robust. At this stage, a secondary, yet equally powerful, driver of microbiome change kicks in: a radical, sustained shift in the host's diet.
Appetite suppression on these medications frequently leads to a massive reduction in total daily caloric intake, often declining by 16% to 39% 12. Furthermore, the specific types of food consumed usually change drastically. Patients who previously consumed Western-style diets characterized by high saturated fats, highly processed foods, and simple sugars frequently find that these foods suddenly trigger intense nausea and food aversion 13. Consequently, they naturally pivot toward eating much smaller, simpler meals that are easier to digest.
This sustained dietary shift literally starves specific bacterial populations out of existence. Bacteria belonging to the Firmicutes phylum are often associated with obesity and are highly efficient at extracting maximum calories from high-fat, high-sugar diets. Because the host is no longer supplying the refined carbohydrates and heavy fats these bacteria require to thrive, their populations begin to steadily decline 3414.
Simultaneously, if the patient follows clinical advice to consume high-quality lean proteins and adequate soluble fibers, the populations of short-chain fatty acid-producing bacteria begin to stabilize and gain a competitive advantage in the gut. The temporary bloating and erratic bowel habits from the first two weeks often begin to subside as the surviving microbial community successfully adapts to the slower, steadier flow of nutrients and the new chemical reality of the gastrointestinal tract 1316.
Month Three and Beyond: Establishing a New Microbial Ecosystem
Around the three-month mark, most patients reach a steady-state maintenance dose of their GLP-1 medication, and their weight loss trajectory is well established. It is at this stage that deep genomic sequencing of human stool samples reveals distinct, measurable, and highly consistent structural shifts in the gut microbiome.
A pivotal 2025 clinical trial conducted by Chen and colleagues, which followed a cohort of patients with type 2 diabetes on semaglutide for 12 weeks, provided a clear, longitudinal window into these long-term microbial changes. The researchers discovered that while the overall microbial alpha diversity - meaning the total number of different bacterial species present - did not change drastically, the relative composition of those bacteria shifted significantly toward a much healthier metabolic profile 1415.
The data revealed a striking decrease in the abundance of the Firmicutes phylum, dropping from roughly 73% at baseline to 56% after twelve weeks of therapy 14. Concurrently, there were significant increases in the Bacteroidota and Actinobacteriota phyla, which are generally associated with leaner human phenotypes and superior metabolic health 14.
The study also highlighted a crucial reduction in opportunistic pathogens. The abundance of Klebsiella, a genus of bacteria notorious for driving systemic inflammation, producing excess ethanol in the gut, and contributing to abnormal blood lipid profiles, decreased significantly 14. By reducing these harmful intestinal bacteria, the medication effectively lowers the systemic inflammatory burden on the body.
In parallel with these bacterial shifts, the researchers observed a rise in the Bifidobacterium genus. This beneficial group of bacteria is well known for supporting the integrity of the gut barrier, reducing local tissue inflammation, and producing essential short-chain fatty acids 1416. Crucially, these 12-week taxonomic changes were accompanied by shifts in over 300 different bacterial metabolites in the patients' bloodstreams, proving that the new microbiome was actively changing how the host processed fats, regulated immune responses, and maintained vascular health 14.
Long-term GLP-1 use, extending from one to two years, appears to support sustained improvements in gut bacteria composition, provided the medication is continued and a health-promoting diet is maintained 313. The medication essentially acts as a permanent chemical scaffold, creating a slower, highly regulated intestinal environment where beneficial bacteria can continually outcompete inflammatory strains 13.
However, clinical evidence strongly indicates that this microbial scaffold is entirely dependent on the continued presence of the drug. When patients stop taking GLP-1 therapies, gastric emptying rapidly speeds back up to baseline levels, the intense satiety signaling ceases, and old dietary habits frequently revert 13. As the environmental pressures are removed, the microbiome changes often reverse just as quickly. The sudden loss of this metabolically favorable, inflammation-lowering bacterial profile is highly likely to be one of the major contributing biological factors to the rapid weight regain experienced by a vast majority of patients who discontinue therapy 13.
The Microbial Winners and Losers: A Taxonomic Breakdown
While the human gut microbiome contains thousands of distinct species, rigorous research into GLP-1 medications repeatedly highlights a few key microbial players whose populations shift dramatically during active treatment. Understanding these specific bacteria helps demystify exactly how these drugs improve metabolic health beyond simple calorie restriction.
If there is a consensus "star" microbe in the era of GLP-1 weight loss medications, it is Akkermansia muciniphila. This unique bacterium lives exclusively in the protective mucus layer lining the intestines and plays a critical, irreplaceable role in maintaining the structural integrity of the gut barrier 139. Higher relative levels of Akkermansia are consistently found in individuals with healthy, flexible metabolisms and lean body mass. Preclinical animal studies and human clinical trials consistently demonstrate that treatment with GLP-1 receptor agonists - particularly liraglutide and tirzepatide - strongly promotes the enrichment and proliferation of Akkermansia 4912.
This enrichment provides massive metabolic dividends. Akkermansia actively strengthens the tight junctions of the intestinal walls, preventing harmful bacterial toxins from leaking out of the gut and into the systemic bloodstream. This reduction in intestinal permeability, commonly referred to as healing a "leaky gut," drastically lowers systemic inflammation, which in turn significantly improves how the body's cells respond to circulating insulin 13. Furthermore, some researchers theorize that the steady proliferation of Akkermansia and the subsequent reduction in neuro-inflammation may be responsible for the mood-stabilizing and cognitive benefits that some patients report long after their initial, rapid weight loss has stabilized 13.
For decades, microbiome researchers have utilized the Firmicutes-to-Bacteroidetes ratio as a rough, high-level biomarker for obesity and metabolic health. Generally, a higher ratio - meaning a gut dominated by Firmicutes with fewer Bacteroidetes - is strongly associated with severe obesity and metabolic syndrome. Firmicutes are highly efficient at extracting excess energy from indigestible dietary components and triggering biological pathways that favor fat storage 412. GLP-1 medications consistently drive this ratio downward. By starving the Firmicutes through reduced caloric intake and fundamentally altering the transit time of the gut, drugs like semaglutide and tirzepatide help push the overarching structure of the microbiome back toward a ratio that closely resembles a naturally lean phenotype 3414.
Equally important to the rise of beneficial microbes is the steep decline of inflammatory, pathogenic microbes. Medications like tirzepatide have been shown in robust animal models to significantly reduce potentially pathogenic bacterial genera such as Erysipelatoclostridium and Helicobacter 1725. In human clinical trials of semaglutide, sharp reductions in Klebsiella have been meticulously documented 14. These specific bacteria are notorious for generating low-grade, chronic inflammation, which is a foundational hallmark of insulin resistance and type 2 diabetes. By aggressively reducing their numbers, GLP-1 drugs help clear the metabolic "static" that prevents the body from burning stored fat efficiently and regulating blood sugar normally.
Comparing the Drugs: Do All GLP-1s Affect the Gut the Same Way?
While they belong to the same overarching pharmaceutical class and share similar mechanisms of action, not all weight-management medications interact with the gut microbiome in the exact same manner. Subtle differences in molecular structure, receptor targets, half-lives, and delivery mechanisms dictate how deeply they reshape the microbial ecosystem.
A summary of how the major medications in this class impact the gut microbiota is detailed below.
Microbiome Impact Across Major Incretin Therapies
| Medication | Mechanism of Action | Observed Microbiome Impact | Clinical Significance |
|---|---|---|---|
| Liraglutide (Saxenda, Victoza) | GLP-1 Receptor Agonist (Daily subcutaneous injection) | Increases Akkermansia muciniphila and Lactobacillus. Induces modest overall structural changes in microbial diversity 49. | Associated with notable renal and hepatic benefits; effectively manages blood glucose and reduces systemic inflammation 25. |
| Semaglutide (Wegovy, Ozempic) | GLP-1 Receptor Agonist (Weekly subcutaneous injection) | Decreases the Firmicutes phylum and Klebsiella. Increases Bacteroidota and Bifidobacterium over a 12-week period 1415. | Strong association with robust long-term weight reduction. Indirectly reshapes the gut through massive, sustained caloric deficits 1025. |
| Tirzepatide (Zepbound, Mounjaro) | Dual GIP & GLP-1 Receptor Agonist (Weekly subcutaneous injection) | Induces broader taxonomic shifts. Reverses dysbiosis, significantly raises Romboutsia and Clostridium, and aggressively reduces Bacteroides and Erysipelatoclostridium 172518. | The dual-action mechanism exerts a more profound influence on microbial ecology, correlating strongly with powerful renoprotective effects and superior overall weight loss 2527. |
| Orforglipron (Investigational) | Oral Non-Peptide GLP-1 Receptor Agonist (Daily pill) | Specific human microbiome sequencing data is currently pending. Exhibits a gastrointestinal side-effect profile (nausea, diarrhea) highly similar to injectable GLP-1s 19. | Does not require fasting or water restrictions like older oral peptides. Aims to deliver efficacy comparable to injectables directly via the digestive tract 30. |
| Oral Semaglutide (Rybelsus) | Oral GLP-1 Receptor Agonist (Daily pill) | Uses the absorption enhancer SNAC to survive harsh stomach acid. Preclinical models suggest SNAC may independently alter gut bacteria and raise inflammatory markers 20. | While highly effective for glycemic control, the long-term daily exposure of the gastrointestinal tract to chemical absorption enhancers is under active scientific investigation for microbiome impacts 20. |
The inclusion of tirzepatide in the therapeutic landscape represents a massive leap forward. Tirzepatide is unique because it targets both the GLP-1 receptor and the glucose-dependent insulinotropic polypeptide (GIP) receptor simultaneously. This dual agonism not only drives statistically superior weight loss in human trials but also seems to exert a much more aggressive, restorative effect on the gut microbiome 2532.
Preclinical studies utilizing diabetic kidney disease models show that tirzepatide effectively and rapidly reverses high-fat diet-induced dysbiosis. Notably, to prove how vital the microbiome is to the drug's success, researchers depleted the gut microbiota of mice using broad-spectrum antibiotics before administering tirzepatide. Without the microbiome present, the metabolic and kidney-protecting benefits of the drug were significantly weakened 171821. This strongly suggests that tirzepatide relies directly on the gut microbiome as an active partner to execute some of its most critical metabolic healing.
The Oral Medication Dilemma: SNAC and Gut Inflammation
As pharmaceutical companies race to develop highly convenient pill versions of these blockbuster drugs, totally new questions about the gut environment arise. Injecting a drug bypasses the immediate physical lumen of the gut, delivering the active compound directly into the systemic circulation. Swallowing a daily pill, however, exposes the delicate lining of the digestive tract to both the active drug and its chemical transport vehicles.
Currently, the only approved oral GLP-1 is oral semaglutide, marketed as Rybelsus. Because peptides like semaglutide are normally destroyed instantly by stomach acid, this pill requires a specialized absorption enhancer called SNAC to survive the harsh environment of the stomach and cross safely into the bloodstream. A 2026 animal study raised significant questions when it suggested that daily, long-term exposure to this SNAC compound was associated with distinct shifts in potentially harmful gut bacteria and elevated inflammatory markers in the intestines 20. While these preclinical findings have not demonstrated any acute harm in human populations, they highlight a critical physiological difference that warrants intense, long-term monitoring.
To circumvent the need for chemical absorption enhancers like SNAC, newer investigational oral molecules like Eli Lilly's orforglipron have been developed. Orforglipron is a small molecule, non-peptide GLP-1 agonist that does not require fasting or water restrictions to be absorbed 1930. In massive Phase 3 clinical trials like ACHIEVE-1 and ATTAIN-1, it has shown remarkable weight loss efficacy, with gastrointestinal side effects closely mirroring those of standard injections 302223. How these pure oral molecules specifically alter the microbial landscape over years of daily use remains one of the most important frontiers for future gastroenterological research.
Predicting Success: Does Your Baseline Microbiome Determine Weight Loss?
One of the most confounding aspects of GLP-1 therapy for endocrinologists and obesity medicine specialists is the sheer variability in patient response. While the average weight loss figures dominate the headlines, a notable minority of patients are considered "non-responders." In large-scale clinical trials, up to 23% of participants occasionally show no clinically significant weight reduction despite strictly adhering to the medication protocol 24. Why do these drugs work brilliantly for some individuals, but completely fail to move the needle for others?
The answer may lie entirely in the specific ecosystem of gut bacteria the patient possessed before they ever took their first dose.
Increasingly, the rapidly expanding field of pharmacomicrobiomics - the rigorous study of how the microbiome affects individual drug response - suggests that baseline microbial signatures can accurately predict a patient's likelihood of success. In a highly scrutinized pilot study of individuals with type 2 diabetes, the patients who responded best to GLP-1 therapies had distinctly different baseline microbial profiles compared to non-responders 4.
Patients who harbored higher initial levels of specific species, such as Bacteroides dorei and Roseburia inulinivorans, experienced significantly greater, more rapid reductions in their long-term blood sugar levels 4. Another longitudinal human study tracking semaglutide and empagliflozin users confirmed that baseline gut microbiome profiles successfully and consistently predicted the degree of glycemic improvement patients achieved at the three-month mark 25.
The biological reasoning behind this baseline predictive power is deeply logical. If a patient's gut is severely dysbiotic - meaning it is overrun with highly inflammatory bacteria that constantly produce toxins that block GLP-1 signaling pathways - the synthetic GLP-1 drug may face massive biological resistance upon entry 49. The systemic inflammation caused by toxic bacterial byproducts can impair insulin receptors throughout the body, blunting the drug's effectiveness at the cellular level. Conversely, a patient who already possesses a solid foundation of short-chain fatty acid-producing bacteria has a gut environment primed and ready to amplify the medication's satiety and metabolic signals 9.
This predictive potential is driving massive commercial and clinical interest in personalized metabolic medicine. In the near future, clinicians might routinely utilize advanced stool sequencing alongside standard blood tests to determine exactly which obesity medication a patient is most likely to respond to, or whether they require a targeted, intensive prebiotic intervention to "fertilize" the gut before starting a GLP-1 agonist 412.
Fueling the Transformation: Fiber, Diet, and Hydration
Because the vast majority of the microbiome changes triggered by GLP-1 medications are driven by the absence of old foods and the markedly slower speed of digestion, what a patient proactively chooses to eat during therapy dictates both the severity of their side effects and the ultimate quality of their new microbial ecosystem.
Clinicians and major nutritional guidelines stress that patients cannot simply eat smaller portions of a standard Western diet and expect optimal, side-effect-free results 12. The typical Western diet - characterized by a severe lack of dietary fiber, high levels of saturated fats, and copious amounts of simple sugars - promotes the exact inflammatory microbial profile that the drug is actively trying to combat 2627. When this diet is combined with the delayed gastric emptying caused by the medication, high-fat meals sit idle in the stomach for hours, inevitably triggering intense nausea, severe vomiting, and acid reflux 18.
To successfully support the gut during this pharmacological transition and minimize adverse events, patients must adopt a strategic, highly microbiome-friendly approach to daily fueling.
Fiber is the undisputed, essential fuel of a healthy microbiome. However, when taking a GLP-1 medication, all fibers are not created equal, and they must be managed with clinical precision to avoid compounding the drug's gastrointestinal side effects.
Soluble fiber, found abundantly in oats, chia seeds, beans, lentils, and apples, attracts water and turns into a soothing, viscous gel during the digestive process 1132. This gel serves two vital physiological purposes. First, it physically stabilizes the delayed gastric emptying caused by the drug, smoothing out the digestive process and drastically reducing the sensation of nausea 32. Second, it is the primary food source for the crucial short-chain fatty acid-producing bacteria in the lower gut 28. By consuming adequate soluble fiber, patients naturally boost their endogenous GLP-1 production, effectively layering their body's natural hormone production directly on top of the pharmaceutical intervention for maximum effect 2829.
Insoluble fiber, found heavily in wheat bran, leafy greens, and whole grains, does not dissolve in water. Instead, it adds physical bulk to the stool and accelerates transit time through the intestines 11. Because severe constipation is one of the most common and medically dangerous side effects of GLP-1 therapy, integrating insoluble fiber is absolutely essential 1113.
However, there is a major, non-negotiable clinical caveat: increasing fiber without simultaneously increasing water intake is a gastrointestinal hazard. Clinical dietitians emphasize that while men should target roughly 35 grams and women 25 grams of daily fiber, if this roughage is consumed without massive increases in hydration, the fiber acts exactly like a dry sponge in a slow-moving gut, making constipation significantly worse and potentially leading to bowel impaction 1113.
Patients transitioning to GLP-1 therapies are broadly and consistently advised to adopt a Mediterranean-style eating pattern to maximize their microbial health 13. This specific dietary framework emphasizes monounsaturated fats, omega-3 fatty acids, complex carbohydrates, and high-quality lean proteins 1213. Research conclusively indicates that diets rich in plant-based diversity foster incredibly robust microbial diversity, far superior to the outcomes seen on Western diets 2627. By seamlessly combining the pharmacological weight-loss power of a GLP-1 agonist with the microbiome-feeding power of a Mediterranean diet, patients actively create an intestinal environment where beneficial bacteria like Akkermansia and Bifidobacterium can thrive permanently, ensuring the metabolic benefits of the drug are fully realized and sustained 1330.
Bottom line
GLP-1 medications do much more than interact with chemical receptors in your brain and pancreas; they fundamentally reshape the microscopic ecosystem of your gut. By slowing digestion and prompting massive dietary changes, these drugs starve out obesity-linked, inflammatory bacteria and create a supportive environment where metabolism-regulating microbes can flourish. However, because these beneficial microbial changes are heavily dependent on diet, maintaining adequate hydration alongside high soluble and insoluble fiber intake is essential to manage side effects and sustain long-term success. While early evidence suggests your baseline microbiome might one day predict exactly how much weight you will lose, larger human trials are still needed to fully untangle the exact causal relationships between the drugs, the gut bacteria, and the scale.