How Do Ozempic and Wegovy Work for Weight Loss
Ozempic and Wegovy are brand names for semaglutide, a medication that mimics a natural digestive hormone to regulate blood sugar and drastically reduce appetite. While both contain the exact same active ingredient, Ozempic is approved at lower doses to manage type 2 diabetes, whereas Wegovy is prescribed at higher doses specifically for chronic weight management. Clinical evidence demonstrates that semaglutide helps patients lose 15% or more of their body weight and significantly lowers the risk of major cardiovascular and kidney events, though stopping the medication usually results in substantial weight regain.
Ozempic vs. Wegovy: What is the Difference?
The unprecedented surge in public awareness surrounding glucagon-like peptide-1 (GLP-1) receptor agonists has led to widespread confusion regarding the difference between Ozempic and Wegovy. Fundamentally, they are the exact same drug - semaglutide - manufactured by the same pharmaceutical company, Novo Nordisk 12. The distinction lies entirely in how the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) have approved them to be used, the dosages at which they are prescribed, and the devices used to deliver them.
Semaglutide was first introduced under the brand name Ozempic in 2017 as a once-weekly injectable treatment to help adults with type 2 diabetes control their blood sugar 12. Over time, endocrinologists and primary care physicians noted a profound secondary effect: patients taking Ozempic were losing a significant amount of weight. Recognizing this powerful side effect, Novo Nordisk initiated dedicated clinical trials to study semaglutide solely for obesity, independent of diabetes. In 2021, the FDA approved a higher-dose formulation of semaglutide under the brand name Wegovy specifically for chronic weight management 131.
To further expand access and provide options for patients who struggle with needles, the FDA approved a daily oral pill version of Wegovy (25 mg) in December 2025 126. A lower-dose oral version of semaglutide, branded as Rybelsus, has already been available for type 2 diabetes since 2019 13.
While health care providers sometimes prescribe Ozempic "off-label" for weight loss when dealing with insurance barriers or shortages, only Wegovy is formally approved to treat obesity 14.
| Feature | Ozempic | Wegovy (Injection) | Wegovy (Pill) | Rybelsus |
|---|---|---|---|---|
| Active Ingredient | Semaglutide | Semaglutide | Semaglutide | Semaglutide |
| Primary Indication | Type 2 Diabetes | Weight Management | Weight Management | Type 2 Diabetes |
| Maximum Target Dose | 2.0 mg (Weekly) | 2.4 mg (Weekly) | 25 mg (Daily) | 14 mg (Daily) |
| Delivery Method | Multi-use injection pen | Single-use injection pen | Oral tablet | Oral tablet |
| Initial FDA Approval | 2017 | 2021 | 2025 | 2019 |
The Science of Satiety: How Semaglutide Re-wires Appetite
To understand why semaglutide is so uniquely effective, one must look at the body's natural incretin system. When a person eats a meal, specialized enteroendocrine L-cells located in the intestines (particularly the ileum and colon) detect the presence of carbohydrates, fats, and proteins 5611. In response, these cells release a hormone called endogenous glucagon-like peptide-1 (GLP-1) 512. This hormone travels through the bloodstream, signaling the pancreas to release insulin in a glucose-dependent manner, while simultaneously suppressing glucagon, a hormone that raises blood sugar 78.
However, natural GLP-1 is incredibly fragile. Within one to two minutes of being released, it is destroyed by an enzyme called dipeptidyl peptidase-4 (DPP-4) 512. Because its lifespan is so brief, endogenous GLP-1 only acts locally and suppresses appetite for a very short window during and immediately after a meal 5.
Semaglutide is a synthetic, long-acting analog of this hormone. Scientists modified the GLP-1 molecule with structural changes - specifically a substitution that resists breakdown by the DPP-4 enzyme, and the addition of a fatty acid chain that allows it to bind to albumin in the blood 579. These engineering modifications extend the drug's half-life from two minutes to approximately seven days 15. By circulating continuously, semaglutide exerts a relentless, sustained effect on the body's appetite regulation systems through two primary mechanisms: a central pathway in the brain and a peripheral pathway in the gut.
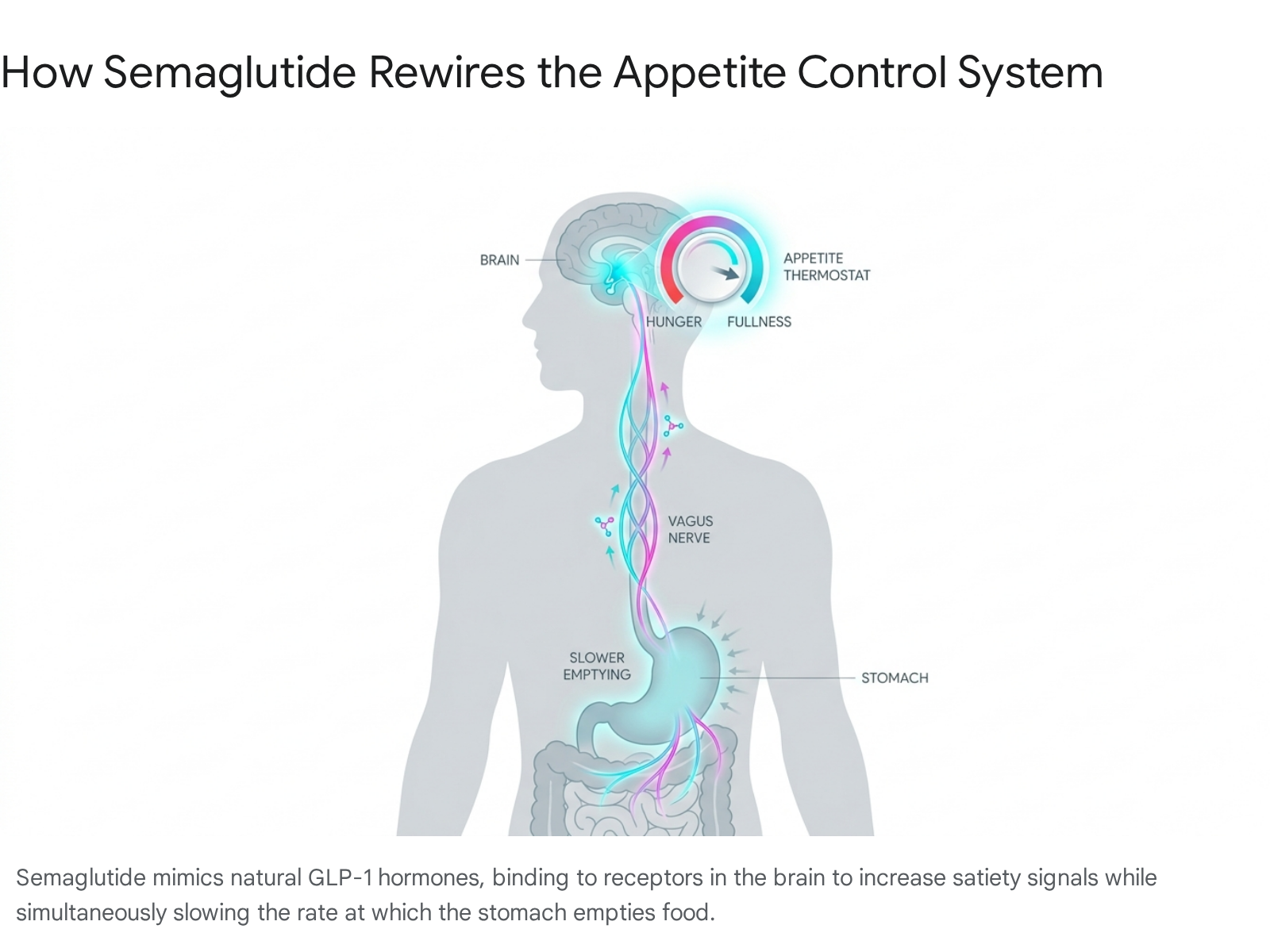
The Gut-Brain Axis and the "Fullness Thermostat"
The brain's hypothalamus acts as the body's metabolic control center, heavily influencing energy balance and the drive to eat 10. The hypothalamus integrates signals from the body to determine a metabolic "set point" for weight. Evolutionarily, the human body is designed to survive famine; when a person attempts to lose weight through traditional dieting, the brain perceives this drop in body mass as a starvation threat. It triggers compensatory mechanisms, slowing the basal metabolic rate and ramping up hunger hormones like ghrelin to force the body back to its heavier set point 121112.
Semaglutide bypasses this evolutionary defense by crossing into the central nervous system. It accesses circumventricular organs, such as the area postrema and the subfornical organ, which lack a restrictive blood-brain barrier 5713. Once there, semaglutide binds to GLP-1 receptors in the arcuate nucleus of the hypothalamus 510. It acts as a master switch, simultaneously activating POMC/CART neurons, which promote feelings of intense satiety, and inhibiting NPY/AgRP neurons, which are responsible for driving hunger 810.
Furthermore, semaglutide acts on the brain's hedonic reward circuitry. By targeting receptors in the ventral tegmental area and the nucleus accumbens, the drug reduces the amount of dopamine released in response to highly palatable food cues 5. Clinically, patients describe this as the elimination of "food noise" - the relentless, intrusive background thoughts about what and when they will eat next. Food simply ceases to be as neurologically rewarding, allowing patients to make dietary choices without fighting intense physiological cravings 512.
Slowing Down the Stomach
Peripherally, semaglutide stimulates the vagus nerve, the primary parasympathetic conduit connecting the gastrointestinal tract to the brainstem 1020. It also physically alters the digestive process by inducing a delay in gastric emptying 78.
Because the stomach retains food for a significantly longer duration, physical stretch receptors in the gastric wall continue sending mechanical fullness signals to the brainstem long after a meal has ended 510. While this delay is highly effective for maintaining satiety and reducing overall caloric intake, it is also the primary biological driver behind the gastrointestinal side effects - such as nausea, bloating, and constipation - that many patients experience when starting the medication 61221.
The Evidence: Do GLP-1 Drugs Actually Work for Weight Loss?
Prior to the introduction of modern GLP-1 therapies, pharmacological weight loss interventions were famously underwhelming. Older anti-obesity medications rarely achieved more than a 5% to 10% reduction in body weight, and their severe side-effect profiles often precluded the long-term therapy required to maintain that loss 622. Semaglutide dramatically altered this landscape, producing results that approach the efficacy of bariatric surgery.
The FDA approval for Wegovy was built upon the landmark Semaglutide Treatment Effect in People with Obesity (STEP) clinical trial program, a massive multi-regional research effort involving thousands of participants globally 1415.
The STEP Clinical Trial Outcomes
In the pivotal STEP 1 trial, 1,961 adults with a body mass index (BMI) of 30 or higher (or 27 or higher with at least one weight-related comorbidity) were randomly assigned to receive either a 2.4 mg weekly injection of semaglutide or a matching placebo 1516. Crucially, the medication was not tested in a vacuum. Both groups were required to adhere to an intensive lifestyle intervention program, which included a 500-calorie daily dietary deficit and a mandate of 150 minutes of physical activity per week 915.
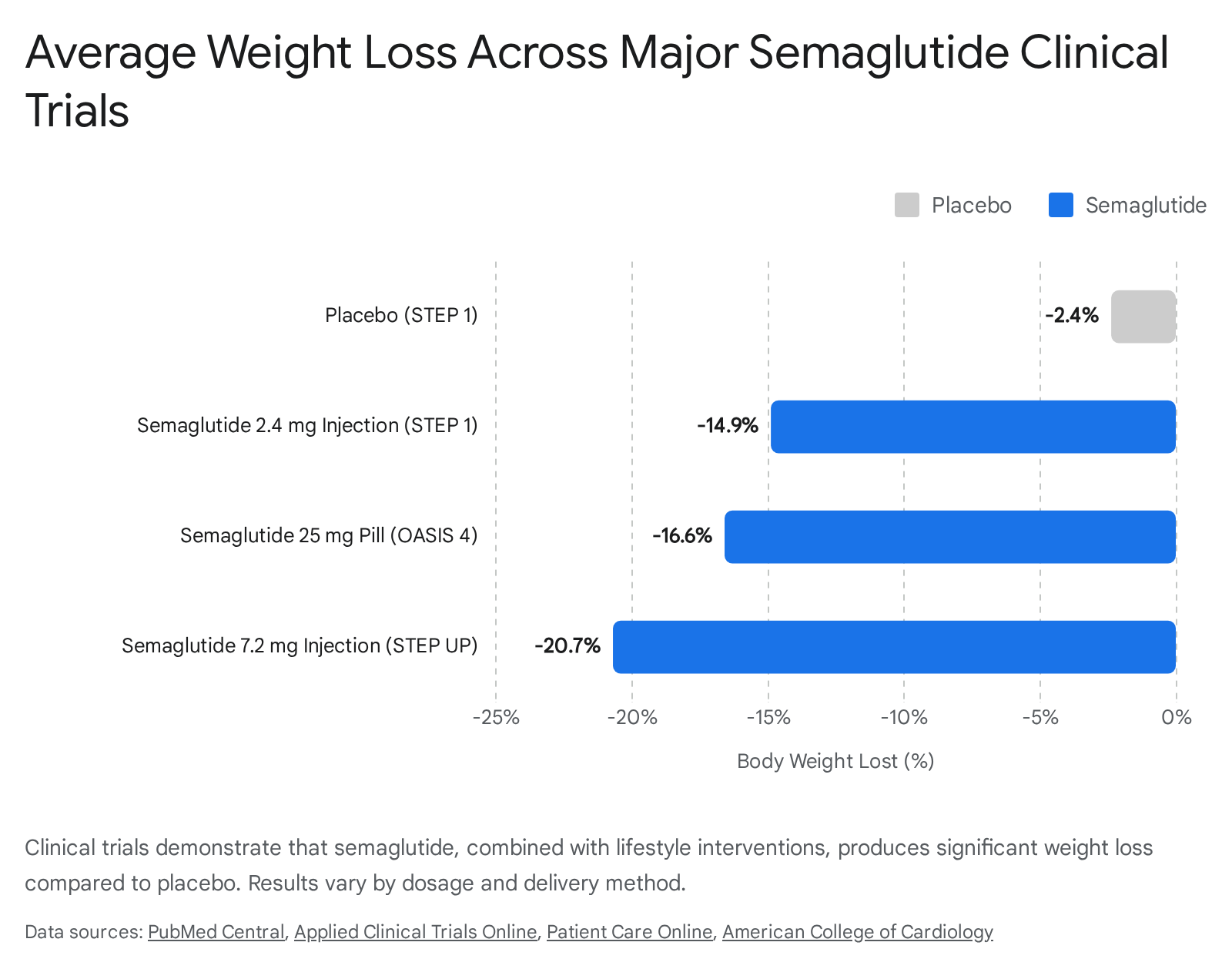
After 68 weeks, participants receiving the semaglutide injection lost an average of 14.9% of their baseline body weight, compared to just 2.4% for those in the placebo group 1416. For a patient starting at 230 pounds, this translates to an average weight loss of roughly 34 pounds. The trial also revealed that 84% of participants on the drug were able to tolerate the full dose at week 68, and more than 50% of the patients on the active drug achieved a weight reduction of at least 15% 141617.
The STEP program included multiple sub-trials to test the drug across different populations. For instance, the STEP 2 trial evaluated patients who had both obesity and type 2 diabetes. Historically, patients with type 2 diabetes have a much harder time losing weight. In this trial, the semaglutide 2.4 mg group lost an average of 9.6% of their body weight over 68 weeks, compared to 3.4% on placebo 914. While lower than the non-diabetic cohort, this still represented a massive clinical improvement in glycemic control and fat reduction 14.
Pushing the Boundaries: Higher Doses and Oral Pills
The ceiling for semaglutide's efficacy is still being actively explored. In early 2025, pharmaceutical data from the STEP UP trial revealed that an experimental, ultra-high 7.2 mg weekly dose of subcutaneous semaglutide yielded a staggering 20.7% average weight loss after 72 weeks 18. Even more notably, a third of the participants in the 7.2 mg cohort lost 25% or more of their total body mass, with an adverse event profile that remained comparable to the standard 2.4 mg dose 18. While this ultra-high dose is not yet commercially available, it signals that higher concentrations can push efficacy into the realm of advanced bariatric procedures.
Simultaneously, researchers solved one of the major barriers to GLP-1 adoption: the injection needle. Because peptides are typically destroyed by stomach acid, creating a viable pill form of semaglutide required complex pharmacological engineering, utilizing specific absorption-enhancing agents like SNAC 7. In the OASIS 4 trial, an oral 25 mg daily dose of semaglutide resulted in a 16.6% weight loss over 64 weeks 2. This compelling data directly supported the FDA's decision to approve the Wegovy pill in late 2025, allowing patients to achieve injection-level weight loss through a simple daily tablet taken on an empty stomach 326.
Do GLP-1 Drugs Cause Muscle Loss?
As semaglutide transformed from a niche diabetes treatment into a global cultural phenomenon, widespread concerns emerged regarding "muscle wasting." Critics pointed out that the rapid, drastic weight loss triggered by the drug was indiscriminately stripping away lean muscle alongside fat, potentially leaving patients frail and damaging their long-term metabolic rate 1128. The medical reality, however, requires more nuance.
In standard human physiology, any form of caloric restriction and rapid weight loss will result in the loss of both adipose tissue (fat) and lean mass (which includes skeletal muscle, bone density, and water). The "Rule of 20-30%" dictates that during typical dietary weight loss, approximately 20% to 30% of the mass lost will naturally be lean tissue, not just fat 11.
To investigate how semaglutide impacts this dynamic, a sub-study embedded within the STEP 1 trial closely monitored 140 participants' body composition using dual-energy X-ray absorptiometry (DEXA) scans. The data confirmed that while patients on semaglutide did lose a quantifiable amount of total lean body mass (about 9.7% from baseline), they lost a vastly disproportionate amount of fat mass (nearly 20% reduction in total fat, and over 27% reduction in visceral fat) 19. As a result, the ratio of lean mass to total body mass actually improved by 3 percentage points 19. In effect, the body composition shifted toward a healthier, leaner overall phenotype 1128.
Therefore, clinical consensus indicates that GLP-1 drugs do not possess a biologically toxic mechanism that directly wastes or attacks muscle fibers 1120. The muscle loss observed is a direct, physiological consequence of severe caloric deficits and a lack of mechanical stimulus 11.
To mitigate this expected lean mass reduction, obesity medicine specialists strongly emphasize a two-pronged strategy: GLP-1 therapy must be paired with elevated dietary protein intake (often above standard daily allowances) and structured resistance training 1120. This combination acts as a metabolic "brake" on muscle reduction. Furthermore, recognizing this challenge, several biotech and pharmaceutical companies are currently running clinical trials combining GLP-1 agonists with muscle-preserving agents, such as myostatin and activin inhibitors, aiming to drive fat loss while actively maintaining lean tissue in frail or older populations 28.
Beyond Weight Loss: Cardiovascular and Kidney Protection
Perhaps the most consequential shift in the medical understanding of semaglutide is the realization that it is not merely a cosmetic weight loss tool, but a potent, systemic cardiometabolic intervention. Obesity acts as an upstream driver of systemic inflammation, cardiovascular disease, and metabolic dysfunction 21. By aggressively treating the root adiposity, semaglutide yields profound secondary health benefits that extend far beyond the scale.
The SELECT Trial and Heart Health
In 2023 and 2024, the medical community's view of Wegovy was permanently altered by the publication of the SELECT trial results. The massive study enrolled 17,604 overweight or obese patients who had a history of cardiovascular disease (such as a prior heart attack or stroke) but did not have a history of diabetes 222324.
Over a median follow-up period of 40 months, patients taking the 2.4 mg semaglutide injection experienced a 20% relative reduction in major adverse cardiac events (MACE), which includes nonfatal heart attacks, nonfatal strokes, and cardiovascular deaths 222425. This represented an absolute risk reduction of 1.5%, dropping the event rate from 8.0% in the placebo group to 6.5% in the semaglutide group, despite 90% of the participants already taking statins and other standard cardiac medications 2225.
Notably, a subsequent analysis of the SELECT data revealed that the cardiovascular protection kicked in rapidly - often within the first three to six weeks, with statistically significant divergence between the drug and placebo groups visible by three months 23. This early benefit occurred well before patients had lost a clinically meaningful amount of weight (less than 5% body weight reduction by month three) 23. This strongly suggests that semaglutide's cardiovascular benefits do not stem solely from fat reduction, but also from improved vascular inflammation, reduction in C-reactive protein (hs-CRP), and direct protective effects on the heart tissue itself 723. This landmark trial led the FDA and the EMA to officially expand Wegovy's label to include cardiovascular risk reduction in 2024 1126.
The FLOW Trial and Chronic Kidney Disease
Similarly, the FLOW trial investigated semaglutide's impact on 3,533 patients suffering from both type 2 diabetes and chronic kidney disease (CKD) 2738. This population is at an exceptionally high risk for kidney failure, cardiovascular events, and premature death 39.
The trial was halted early by an independent data monitoring committee because the benefits were so overwhelmingly clear 38. Semaglutide reduced the risk of major kidney disease events - a composite metric including the onset of kidney failure, the need for dialysis or transplantation, or a 50% drop in kidney function - by 24% compared to a placebo 2739. Additionally, the drug significantly slowed the annual decline of estimated glomerular filtration rates (eGFR), while simultaneously lowering the risk of death from any cause by 20% 2739. These results established semaglutide as a foundational therapy for renal protection in diabetic populations.
Emerging Frontiers: Liver Disease and Sleep Apnea
The systemic benefits of GLP-1 receptor agonists continue to unfold in ongoing research. Cardiometabolic diseases frequently overlap, and researchers are actively exploring semaglutide's efficacy in treating metabolic dysfunction-associated steatotic liver disease (MASLD) and its more severe inflammatory form, MASH 3740. The drug's ability to reduce insulin resistance and lower pro-inflammatory cytokines makes it a promising candidate for improving liver histology and reducing hepatic fat 7. Additionally, trials are underway evaluating the drug class for improvements in obstructive sleep apnea, knee osteoarthritis, and even neurodegenerative conditions, pointing toward a future where a single GLP-1 prescription addresses a cascade of interconnected ailments 37.
What Happens When You Stop Taking Semaglutide?
A common question among prospective patients is whether they can take semaglutide for a year, reach their goal weight, and then simply stop the medication while maintaining their new physique. The clinical data strongly indicates that this is an ineffective strategy. Obesity is now universally recognized by the medical community as a chronic, relapsing disease, much like hypertension or asthma; if you remove the pharmacological intervention controlling the disease, the symptoms invariably return 2829.
When semaglutide is discontinued, the artificial extension of the gut-brain signaling halts. Without the drug binding to the GLP-1 receptors, gastric emptying speeds back up to normal rates, the suppression of the hypothalamic hunger centers lifts, and the intense food cravings and "food noise" return 4330.
The STEP 1 trial extension study provided a stark, quantified look at this reality. Researchers tracked a subset of 327 trial participants for an entire year after they stopped taking semaglutide and ceased their intensive lifestyle counseling 28. By week 120 (one year off the drug), the participants had regained an average of 11.6 percentage points of the 17.3% body weight they had lost 28. In short, they regained roughly two-thirds of the lost weight within 12 months. Furthermore, the cardiometabolic improvements they had achieved - such as lowered blood pressure and improved lipid profiles - largely reverted toward their baseline levels 2829.
Real-world observational data from large health systems reflects a slightly more nuanced outcome, but confirms the general trend. A review of over 20,000 patient records by Epic Research found that one year after stopping semaglutide, 17.7% of patients had regained all the weight they lost or even exceeded their initial baseline weight 45. However, a majority (56.2%) managed to remain around the same weight they were when they stopped, or continued to lose slightly 45. This variability largely depends on how deeply a patient integrated structural behavioral, dietary, and exercise changes during their treatment phase 4345.
Because abrupt discontinuation leads to such rapid rebound weight gain, some obesity medicine specialists advocate for structured tapering - gradually reducing the dose over several weeks or months to ease the body's transition - though the evidence base for specific tapering schedules remains limited 4330. Ultimately, for the vast majority of individuals, maintaining the initial dramatic results requires staying on a long-term maintenance dose of the medication 2843.
Understanding the Side Effects and Long-Term Safety
While semaglutide is generally considered safe and well-tolerated for its approved indications, its safety profile is not without friction. Because the drug fundamentally alters the speed and function of human digestion, gastrointestinal side effects are remarkably common and expected.
Common Gastrointestinal Issues
In clinical trials, up to 74% of participants reported some form of gastrointestinal distress, most notably nausea, vomiting, diarrhea, or constipation 946. These symptoms are typically mild to moderate and are most severe during the "dose escalation" phase - the first 16 to 20 weeks when a patient's dosage is incrementally raised every four weeks to allow the body to acclimate 94347.
For most users, these side effects wane over time as steady-state pharmacology is achieved, though severe GI intolerance causes roughly 4.5% to 7% of users to permanently abandon the drug 915. Clinicians frequently advise patients to avoid rich, fatty, or highly processed foods that are difficult to digest while on the medication to minimize nausea 12.
Rare But Serious Risks
Beyond transient nausea, there are rarer but medically significant adverse events that warrant strict monitoring. The FDA and global health authorities monitor signals for several serious conditions associated with the GLP-1 class:
- Pancreatitis and Gallbladder Disease: The drug can increase the risk of acute pancreatitis (inflammation of the pancreas) and cholelithiasis (gallstones). While the gallbladder issues are largely consistent with the physiology of rapid weight loss rather than a direct toxic drug effect, patients presenting with severe, radiating abdominal pain must seek immediate medical evaluation. Patients with a prior history of pancreatitis are generally advised against using semaglutide 21464748.
- Gastroparesis (Stomach Paralysis): In rare instances, the medically induced slowing of the stomach can become pathological, leading to severe bowel obstructions (ileus) or intractable vomiting. The FDA has added safety warnings to Ozempic's official label regarding intestinal obstruction 4950.
- Vision Issues: In 2025, observational data highlighted a potential link between semaglutide and non-arteritic anterior ischemic optic neuropathy (NAION), a rare condition that can cause sudden, irreversible vision loss. While major international studies suggest a small but measurable increase in risk, the data is observational, causality is not proven, and research is actively ongoing 49.
- Thyroid Tumors: Semaglutide carries a strict "black box" warning regarding thyroid C-cell tumors. This warning is based entirely on studies in rodents; it is currently unknown if semaglutide causes medullary thyroid carcinoma (MTC) in humans. Nevertheless, the drug is strictly contraindicated for anyone with a personal or family history of MTC or Multiple Endocrine Neoplasia syndrome type 2 (MEN2) 214748.
The Long-Term Safety Data Gap
As GLP-1 prescriptions skyrocket globally, medical experts repeatedly emphasize a significant "data gap." While short-term and medium-term safety (up to four years) is well established through trials like SELECT and STEP, decades-long safety data for non-diabetic patients maintaining high-dose GLP-1 therapy simply does not exist yet 464849.
The World Health Organization (WHO) and independent reviews have noted that while the weight loss efficacy is undeniable, evidence on the multi-decade consequences of continuous receptor activation remains uncertain 4931. This underscores the medical consensus that semaglutide is a serious pharmaceutical intervention intended for patients facing legitimate metabolic risks, not a casual cosmetic tool.
The Global Shortage and the Compounding Controversy
The viral popularity of Wegovy and Ozempic, fueled by intense media coverage and social media exposure, led to a severe, multi-year global supply shortage 2632. The overwhelming demand vastly outpaced Novo Nordisk's manufacturing capacity, particularly for the complex auto-injector pen devices used to deliver the drug 3233. Consequently, both drugs were placed on the FDA and EMA national drug shortage lists starting in 2022 3234.
This shortage triggered a massive regulatory loophole in the United States. Under sections 503A and 503B of the Federal Food, Drug, and Cosmetic Act, when an FDA-approved drug is officially listed as "in shortage," licensed compounding pharmacies and outsourcing facilities are legally permitted to produce and sell "essentially a copy" of the drug to fill the public health supply gap 333435.
Overnight, thousands of telehealth clinics and medical spas began offering cheaper, unbranded "compounded semaglutide." Between 2021 and 2023, semaglutide prescription fills increased by an astonishing 442%, largely driven by this compounded market 34. However, compounded drugs are not vetted by the FDA for safety, efficacy, or purity. Health officials and Novo Nordisk raised severe alarms, noting that some compounders were using untested salt forms of semaglutide (like semaglutide sodium) rather than the approved base molecule, leading to reports of inconsistent dosing, variable purity, and increased adverse events 46493435.
In response to the crisis, Novo Nordisk executed an $11 billion acquisition of three Catalent contract-manufacturing facilities in 2024, massively expanding their peptide-injection production capacity 33. By early 2025, the supply chain stabilized. On February 21, 2025, the FDA officially declared the semaglutide shortage resolved, immediately terminating the enforcement discretion that allowed pharmacies to compound the drug 3334. This resolution cleared the way for Novo Nordisk to launch hundreds of trademark infringement and false advertising lawsuits against clinics and pharmacies continuing to sell unauthorized versions, forcing the grey market to rapidly contract 4934.
Bottom line
Semaglutide, sold as Ozempic for diabetes and Wegovy for obesity, represents a historical paradigm shift in metabolic medicine. By mimicking natural hormones to rewire the brain's appetite centers and slow digestion, clinical evidence overwhelmingly proves it induces significant, sustained weight loss while offering profound protection against cardiovascular and kidney disease. However, it is a chronic treatment, not a temporary cure; discontinuing the medication usually results in rapid weight regain, and the medical community continues to closely monitor the drug to bridge the gap in decades-long safety data.