How Much Weight Loss Do GLP-1s Actually Deliver
Current FDA-approved GLP-1 medications typically help patients lose between 15% and 22.5% of their total body weight over a year to 18 months, while next-generation drugs currently in late-stage trials are pushing these boundaries near 30%. However, clinical data shows that up to 40% of the weight lost can be lean muscle mass, and patients typically regain roughly two-thirds of their lost weight within a year of stopping the medication.
The Weight Loss Pharmacotherapy Boom
The landscape of obesity treatment has fundamentally shifted. For decades, the medical community relied primarily on behavioral interventions - diet and exercise - with mixed long-term success. Bariatric surgery offered substantial weight reduction but carried surgical risks and accessibility barriers. Today, a new class of medications known as incretin mimetics, primarily glucagon-like peptide-1 (GLP-1) receptor agonists, has bridged the gap between lifestyle interventions and surgery.
The demand for these drugs has been unprecedented. Real-world data analyzing over 40 million United States patient records shows that prescriptions for GLP-1 drugs to treat overweight or obesity surged by 587% between 2019 and 2024 1. In 2019, semaglutide accounted for roughly 31% of new GLP-1 prescriptions; by 2023, it accounted for over 88% 21. Interestingly, the demographic profile of users is also shifting. First-time prescribing rates for young adults aged 18 to 39 increased by 588% from 2019 to 2024, a period during which the rate of bariatric surgeries fell by nearly 42% 1.
Despite this explosive growth, a massive unmet clinical need remains. In 2024, only 11.2% of patients officially diagnosed with overweight or obesity were prescribed a GLP-1 drug, while just 0.28% underwent bariatric surgery 1. As clinical trials continue to yield data, healthcare providers and patients face a complex matrix of choices regarding efficacy, dosing, side effects, and long-term biological impacts.
The Biology of Satiety: How These Medications Work
To understand the varied results of these medications, it is necessary to examine how they interact with the body's natural endocrine system. GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide) are incretin hormones secreted by the intestines immediately following the ingestion of nutrients 23.
Naturally released GLP-1 and GIP are rapidly broken down by an enzyme called dipeptidyl peptidase-4 (DPP-4), meaning their effects are short-lived in the body 3. Modern weight-loss injectables and pills are receptor agonists - synthetic molecules engineered to mimic these natural hormones while resisting rapid degradation, allowing them to remain active for days or weeks 23.
Mechanisms of Action
These drugs facilitate weight loss through a multi-system approach that spans the brain, the gut, and the metabolic organs:
- Neurological Appetite Suppression: GLP-1 and GIP cross the blood-brain barrier and target appetite control centers, particularly the hypothalamus 26. They stimulate neurons that promote satiety (fullness) and inhibit neurons that drive hunger. Clinically, this is often described by patients as quieting "food noise" - the constant, intrusive thoughts about eating 4. GIP specifically enhances GLP-1's effects by improving the brain's response to fullness 2.
- Delayed Gastric Emptying: GLP-1 slows the rate at which the stomach empties food into the small intestine 265. This physical mechanism prolongs the sensation of a full stomach after a meal, reducing the desire to snack between meals 56. Interestingly, while GLP-1 strongly inhibits gastric emptying, isolated GIP has been shown to have little effect on this specific gastrointestinal mechanism 3.
- Metabolic Regulation: Both hormones act on the pancreas to stimulate insulin release when blood sugar is high and suppress glucagon, a hormone that raises blood sugar 265. GIP uniquely modulates fat metabolism, promoting both lipogenesis (fat storage) and lipolysis (fat breakdown) depending on the body's immediate energy needs 6.
While early drugs targeted only GLP-1, the pharmaceutical industry has rapidly evolved toward dual and triple agonists, combining multiple hormonal mimics into single molecules to create synergistic effects on weight and metabolism 610.
Efficacy by the Numbers: Drug Comparisons
The landscape of obesity pharmacotherapy is currently dominated by a few key molecules, each with its own clinical profile, dosing structure, and maximum observed weight loss.
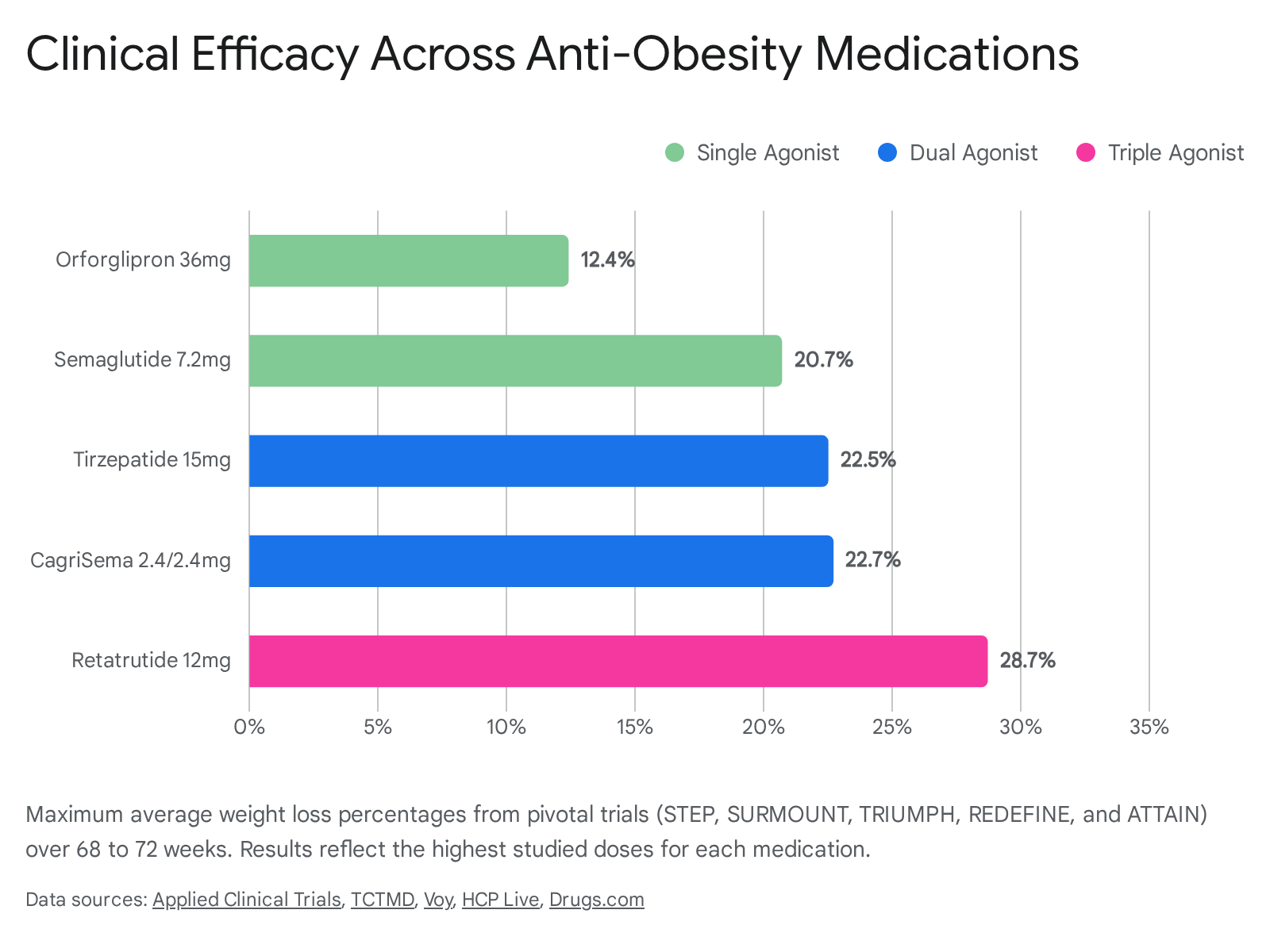
| Active Ingredient | Brand Name(s) | Mechanism of Action | Max Average Weight Loss | Primary FDA Indications |
|---|---|---|---|---|
| Semaglutide | Wegovy, Ozempic | GLP-1 Agonist | ~15% (at 2.4 mg) to 20.7% (at 7.2 mg) | Obesity, Type 2 Diabetes, Cardiovascular Risk, MASH |
| Tirzepatide | Zepbound, Mounjaro | GLP-1 + GIP Dual Agonist | ~20.9% to 22.5% | Obesity, Type 2 Diabetes, Obstructive Sleep Apnea |
| Retatrutide | (Investigational) | GLP-1 + GIP + Glucagon Triple Agonist | ~28.7% | Currently in Phase 3 trials |
| Semaglutide + Cagrilintide | CagriSema (Investigational) | GLP-1 + Amylin Dual Agonist | ~22.7% | Currently in Phase 3 trials |
| Orforglipron | Foundayo | Oral GLP-1 Agonist (Non-peptide) | ~11.1% to 12.4% | Obesity, Overweight |
Semaglutide: The Foundation of Modern Obesity Care
Semaglutide - marketed as Ozempic for Type 2 diabetes and Wegovy for chronic weight management - was the first drug to prove that highly effective, non-surgical weight loss was possible at a population level 1112.
The clinical evidence for semaglutide is anchored by the STEP (Semaglutide Treatment Effect in People with obesity) trial program. In the foundational STEP 1 trial, 1,961 adults without diabetes were given a once-weekly 2.4 mg subcutaneous injection alongside a lifestyle intervention 137. Over 68 weeks, participants receiving semaglutide lost an average of 14.9% of their baseline body weight, compared to just 2.4% in the placebo group 1378.
The trial revealed that 86% of patients on the medication achieved at least a 5% reduction in total body weight, and nearly one-third (32%) lost 20% or more of their body weight 137. Across the STEP 1, 3, 4, and 8 trials, the 2.4 mg dose consistently delivered mean weight losses ranging from 14.9% to 17.4% 9. In patients with Type 2 diabetes (STEP 2), weight loss was more modest, averaging 9.6% compared to 3.4% for placebo, a phenomenon common across metabolic medications 9.
Seeking to push the boundaries of single-agonist therapy, Novo Nordisk recently concluded the STEP UP trial, which tested a massive 7.2 mg dose of semaglutide. Topline data showed that patients on the 7.2 mg dose experienced an average weight loss of 20.7% after 72 weeks, with 33.2% of patients losing 25% or more of their body weight 17. The safety profile remained consistent with the 2.4 mg dose, primarily involving mild to moderate gastrointestinal adverse events 17.
Tirzepatide: The Dual-Agonist Breakthrough
While semaglutide revolutionized the space, tirzepatide (marketed as Zepbound for obesity and Mounjaro for diabetes) introduced the concept of dual-receptor agonism. By mimicking both GLP-1 and GIP, tirzepatide amplifies insulin secretion and further reduces appetite beyond what a GLP-1 can do alone 12.
The SURMOUNT clinical trial program demonstrated unprecedented efficacy. In SURMOUNT-1, which enrolled 2,539 adults with overweight or obesity, participants receiving the maximum 15 mg weekly dose achieved a mean body weight reduction of 20.9% to 22.5% over 72 weeks 101112. Over 60% of patients receiving the 15 mg dose lost more than 20% of their baseline weight, and over 90% achieved at least a 5% reduction 1011.
For years, clinicians debated whether the dual-agonist tirzepatide was truly superior to the single-agonist semaglutide. The SURMOUNT-5 trial, a phase 3b open-label study, settled the question directly. Enrolling 751 adults with obesity or overweight and comorbidities, the trial pitted the maximum tolerated dose of tirzepatide (10 or 15 mg) against the maximum dose of semaglutide (1.7 or 2.4 mg) over 72 weeks 212213. Tirzepatide achieved a 20.2% mean body weight reduction compared to 13.7% for semaglutide, representing a 47% greater relative weight loss 2114. Furthermore, 31.6% of patients taking tirzepatide achieved a massive 25% reduction in body weight, compared to just 16.1% of those taking semaglutide 2114.
Retatrutide: The Triple Agonist
The pharmaceutical industry is not stopping at dual agonists. Retatrutide is an investigational triple agonist that targets three receptors: GLP-1, GIP, and Glucagon 1015. The addition of glucagon receptor activation is a novel mechanism believed to increase energy expenditure and further enhance weight loss efficacy 15.
Results from the phase 3 TRIUMPH-4 trial, released in late 2025, showed that participants with obesity and knee osteoarthritis taking a 12 mg dose of retatrutide lost an average of 28.7% of their body weight over 68 weeks 262716. This represents a loss of roughly 71 pounds for the average participant, the highest mean percentage seen in any obesity treatment trial to date, nearing the results traditionally achieved only through bariatric surgery 27. Seven additional TRIUMPH phase 3 trials are scheduled to conclude throughout 2026, with an eye toward FDA submission 2627.
CagriSema: The Amylin Combination
Novo Nordisk's CagriSema takes a different combination approach. It is a fixed-dose injection containing semaglutide and cagrilintide, a long-acting amylin receptor agonist 2917. Amylin is a hormone co-secreted with insulin that also regulates satiety 17.
In the REDEFINE 1 trial, coadministration of cagrilintide 2.4 mg and semaglutide 2.4 mg resulted in a 20.4% to 22.7% mean body weight reduction at week 68, significantly outperforming both semaglutide alone (16.1%) and placebo 3132. The drug was submitted for FDA approval for weight management in December 2025 2932. In patients with Type 2 diabetes (REIMAGINE 2 trial), CagriSema led to a superior weight loss of 14.2% compared to 10.2% with semaglutide alone, demonstrating dual benefits across metabolic disease states 3132.
Foundayo (Orforglipron): The Oral Alternative
While injectable medications have dominated the market, adherence to weekly injections remains a barrier for some patients. Enter Foundayo (generic name: orforglipron), manufactured by Eli Lilly and granted FDA approval on April 1, 2026 3318.
Unlike Rybelsus (an oral version of semaglutide that requires rigid fasting rules before and after taking it), Foundayo is a small-molecule, non-peptide GLP-1 receptor agonist 3335. Because it is not a peptide, it does not get destroyed by stomach acid in the same way, meaning it can be taken once daily at any time of day, with or without food 3335.
In the Phase 3 ATTAIN-1 trial, individuals taking the highest dose of Foundayo (equivalent to the 17.2 mg commercial tablet) who adhered to the treatment lost an average of 12.4% of their body weight (27.3 pounds) over 72 weeks, compared to 0.9% for placebo 1835. When accounting for all participants regardless of trial completion, average weight loss was 11.1% (25 pounds) 18. While the total weight loss is lower than that of injectables like tirzepatide, the convenience of a daily pill with flexible timing is expected to capture a massive segment of the market 35.
The Lifestyle Variable: Diet and Exercise Still Matter
A common misconception regarding incretin therapies is that these medications work in a vacuum, melting away fat regardless of patient behavior. In reality, all of the major clinical trials evaluating these drugs - including the STEP, SURMOUNT, and ATTAIN programs - paired the medication with intensive, structured lifestyle interventions 101236.
For example, in the STEP 1 trial, participants were subjected to a 500-kilocalorie per day deficit relative to their estimated energy needs, and were required to engage in 150 minutes of physical activity each week 73619. They tracked their food intake and met with trained healthcare professionals every four weeks for counseling 3638. The SURMOUNT trials featured similar lifestyle lead-in periods and ongoing counseling 1012.
These interventions alone are effective, but limited. In the placebo arms of these trials, participants undergoing the exact same rigorous lifestyle counseling generally lost only between 2.4% and 3.1% of their body weight over 68 to 72 weeks 123638. The medications act as biological amplifiers, altering the gut-brain axis so that patients can successfully adhere to a caloric deficit without the overwhelming physiological pushback of hunger, cravings, and food noise 436.
The Hidden Cost of Weight Loss: Muscle Depletion
Perhaps the most critical nuance surrounding GLP-1 weight loss is the composition of the weight being lost. While the numbers on the scale drop dramatically, clinical data reveals that a significant portion of that weight is lean body mass, which includes skeletal muscle, bone, and organs 3940.
Dual-energy X-ray absorptiometry (DEXA) sub-studies of these trials show that roughly 25% to 40% of the total weight lost on GLP-1 and GLP-1/GIP medications comes from lean mass 402021.
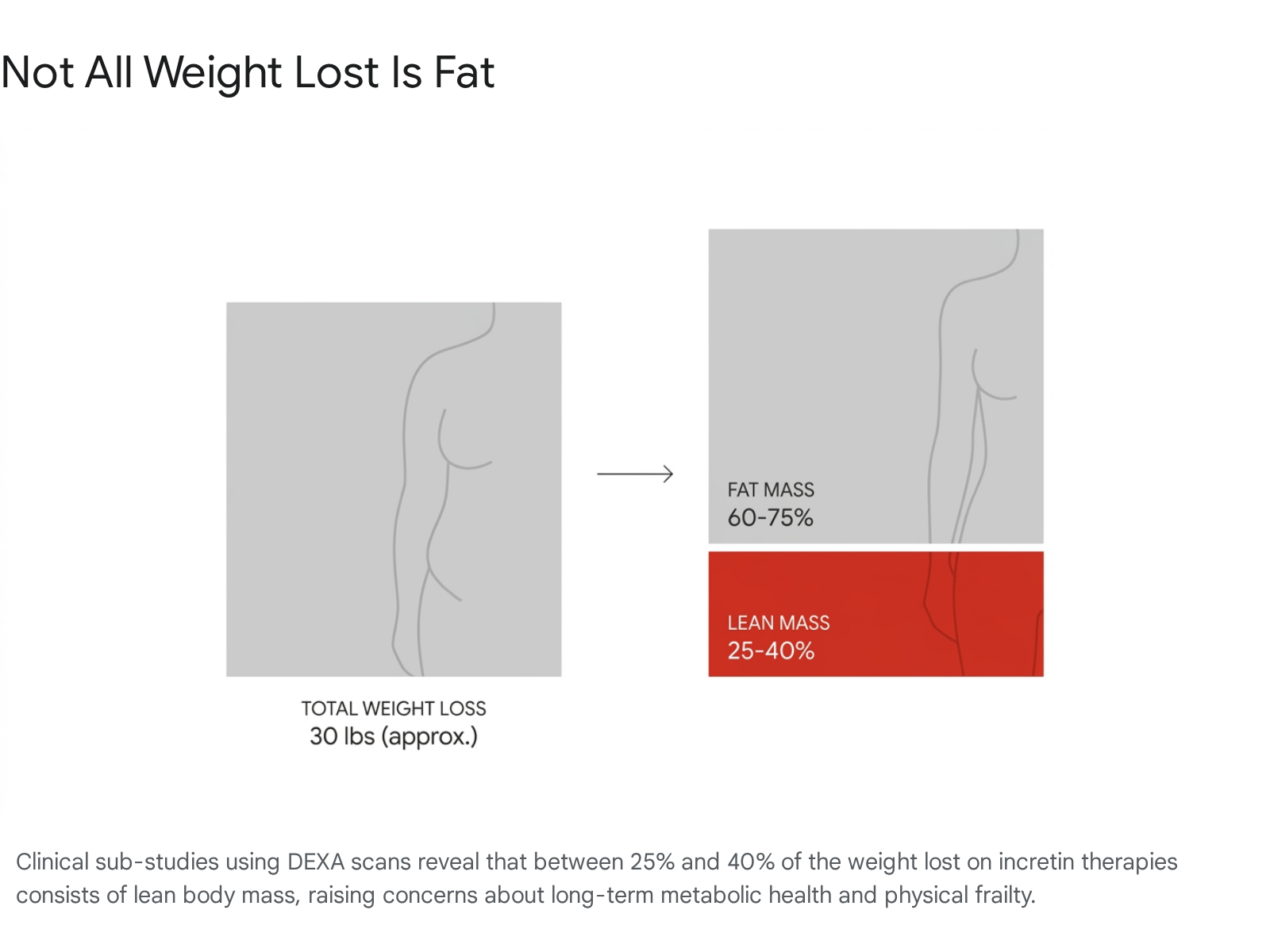
For context, in the STEP 1 trial, participants on semaglutide lost an average of 6.9 kg (about 15 pounds) of lean mass 4022. In the SURMOUNT-1 trial for tirzepatide, approximately 25% of the total weight lost was lean mass, a figure that remained relatively consistent across demographic subgroups 21.
Why Muscle Loss Matters
Muscle loss is not merely an aesthetic concern; it is a metabolic and functional crisis. Skeletal muscle stabilizes blood sugar, boosts immunity, protects joints, and drives the body's basal metabolic rate 3944.
For older adults, medication-induced muscle loss threatens to exacerbate age-related sarcopenia (natural muscle wasting). Natural aging reduces skeletal muscle mass by 12% to 16%, and adding a GLP-1 drug on top of this could push older patients over the edge into clinical frailty, increasing the risk of falls, fractures, and loss of independence 2346. Furthermore, a loss of lean mass lowers the body's basal metabolic rate, making it harder to maintain weight loss in the long term 4647.
Preventing Lean Mass Depletion
Medical consensus is shifting from simply celebrating weight loss to actively managing body composition. To protect lean mass while on GLP-1 medications, clinical guidelines suggest a targeted behavioral and pharmaceutical approach:
- High Protein Intake: Patients must overcome the drug's appetite-suppressing effects to consume adequate protein. Experts recommend 1.2 to 1.6 grams of protein per kilogram of body weight per day (roughly 90 to 120 grams for an average adult) to provide the necessary amino acids for muscle preservation 4824.
- Resistance Training: Cardiovascular exercise alone is insufficient. Resistance training 2 to 4 times per week is non-negotiable for signaling the body to retain muscle tissue while in a severe caloric deficit 464850.
- Adjunct Therapies: The pharmaceutical industry is currently testing muscle-preserving agents to pair with GLP-1s. For example, bimagrumab, a lab-made antibody that blocks a muscle-limiting protein called activin type II, is in clinical trials combined with semaglutide and tirzepatide to help patients shed fat while actually increasing lean muscle mass 44.
| Metric | GLP-1 Weight Loss Composition | Healthy Weight Loss Goal |
|---|---|---|
| Fat Mass Lost | 60% - 75% | > 85% |
| Lean Mass Lost | 25% - 40% | < 15% |
The Rebound Effect: Discontinuation and Weight Regain
Perhaps the most sobering data surrounding obesity medications is what occurs upon discontinuation. Obesity is increasingly recognized by the medical community not as a temporary state to be "cured" with a short course of treatment, but as a chronic metabolic condition - akin to hypertension or Type 2 diabetes - requiring long-term, possibly lifelong, management 135125.
Multiple randomized withdrawal trials have demonstrated a near-universal truth: if you stop the medication, the weight comes back.
In the SURMOUNT-4 trial, patients took tirzepatide for a 36-week lead-in period, achieving a mean weight reduction of 20.9% 512654. At week 36, half the participants were blindly switched to a placebo for a year. Those who maintained tirzepatide lost an additional 5.5% of their body weight, while the placebo group experienced a rapid mean weight gain of 14.0% 5126. Astonishingly, 82.5% of participants who stopped tirzepatide regained at least a quarter of the weight they had initially lost within a single year 25.
The STEP 1 extension and STEP 4 trials evaluating semaglutide showed identical trends. Patients withdrawn from semaglutide regained roughly two-thirds of their lost weight within one year 1354. A 2026 meta-analysis of 37 studies found that after stopping semaglutide or tirzepatide, patients regained an average of 9.9 kg (about 22 pounds) in the first year 2756. The data projects that practically all participants will return to their baseline weight within 17 to 18 months of stopping treatment 2756.
Furthermore, as the weight returns, the metabolic benefits - such as improvements in blood pressure, cholesterol, and glycemic control - reverse just as quickly 512556. This rebound effect underscores the necessity of continuous pharmacotherapy for the maintenance of both weight reduction and cardiometabolic health.
Systemic Benefits Beyond the Scale
While weight loss dominates the headlines, the most significant medical developments for GLP-1s lie in their pleiotropic (multi-system) effects on the heart, liver, and kidneys. The normalization of metabolic processes has ripple effects throughout the entire body.
Cardiovascular and Renal Protection
In March 2024, Wegovy was approved by the FDA to reduce the risk of major adverse cardiovascular events (MACE) in adults with cardiovascular disease 1728. A 2026 meta-analysis of over 85,000 patients found that GLP-1 receptor agonists reduce the risk of major cardiovascular events by 13%, kidney failure by 16%, and all-cause death by 12% 29.
Interestingly, these benefits extend beyond Type 2 diabetes. A massive target trial emulation study published in 2026 evaluated over 174,000 patients and showed that cardiovascular and kidney benefits extend to patients with Type 1 Diabetes, a group traditionally excluded from these therapies. In this cohort, GLP-1 users demonstrated a 15% reduced risk of MACE and a 19% lower risk of end-stage kidney disease without increasing the risk of diabetic ketoacidosis 30.
Liver Disease (MASH)
In August 2025, the FDA granted accelerated approval to Wegovy to treat metabolic dysfunction-associated steatohepatitis (MASH) - formerly known as NASH - with moderate to advanced liver fibrosis 3161. MASH is a serious liver disease characterized by excessive scar tissue and inflammation. In the Phase 3 ESSENCE trial, 63% of participants receiving Wegovy achieved MASH resolution without worsening of liver scarring, compared to just 34% on placebo 3132. This approval marks the first time a GLP-1 agonist has been cleared for a condition that affects an estimated 22 million people in the United States 63.
Obstructive Sleep Apnea (OSA)
In December 2024, Zepbound (tirzepatide) received FDA approval as the first pharmaceutical treatment for moderate to severe obstructive sleep apnea (OSA) in adults with obesity 3334. OSA occurs when the upper airway becomes blocked during sleep, a condition severely exacerbated by excess adiposity around the neck and airway.
In the SURMOUNT-OSA trials, tirzepatide reduced the apnea-hypopnea index (AHI) by roughly 25 to 29 events per hour, effectively resolving the condition for a significant proportion of participants by targeting the underlying adiposity driving the airway collapse 333466. This represents a major paradigm shift, offering a biological treatment option rather than relying solely on mechanical interventions like CPAP machines 6667.
Bottom line
GLP-1 and dual-agonist therapies are highly effective, delivering sustained weight loss between 15% and 22.5% of total body weight, with upcoming triple-agonists threatening to break the 28% mark. However, these drugs are not short-term fixes; clinical withdrawal studies prove that ceasing the medication leads to rapid weight regain, reverting patients to their baseline weight within 18 months. Furthermore, because up to 40% of the weight lost is metabolically crucial lean muscle mass, patients must engage in aggressive protein consumption and resistance training to avoid long-term physical frailty.