How GLP-1 Drugs Work, Cost, and Affect Your Body
Glucagon-like peptide-1 (GLP-1) medications are a class of metabolic drugs that mimic natural gut hormones to regulate blood sugar, dramatically slow digestion, and suppress appetite by interacting with the brain's reward centers. While they offer unprecedented benefits for weight loss, cardiovascular health, and potentially addiction management, patients must navigate high financial costs, gastrointestinal side effects, and the clinical risk of muscle loss. With the recent resolution of global supply shortages and the introduction of highly effective daily pills in 2026, the landscape of obesity and metabolic treatment has definitively shifted from acute intervention to long-term chronic maintenance.
The Science of Satiety and Metabolic Reset
To understand how GLP-1 medications exert such profound effects on the human body, it is necessary to examine the endogenous hormones they are designed to mimic. Glucagon-like peptide 1 is an incretin hormone produced primarily by the L-cells of the intestines in response to nutrient ingestion 12. In a natural, unmedicated state, this native GLP-1 has an exceedingly short lifespan, lasting approximately two minutes in the bloodstream before it is rapidly degraded by an enzyme known as dipeptidyl peptidase-4 (DPP-4) 1. Synthetic GLP-1 receptor agonists, such as semaglutide and liraglutide, are molecularly engineered to resist this enzymatic degradation, transforming a transient biological signal into a sustained pharmacological intervention that can last for days or weeks 1.
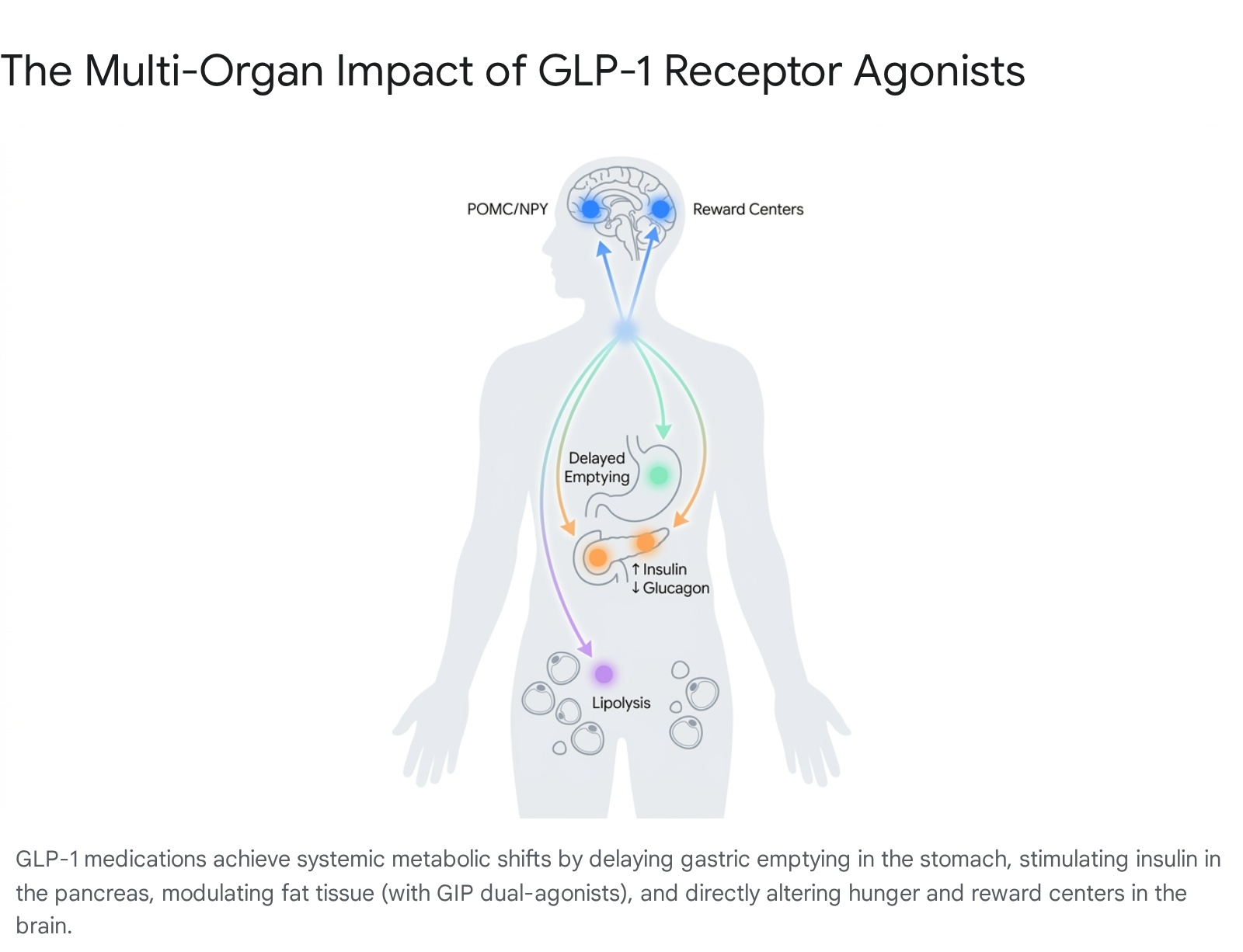
The resulting weight-loss and metabolic regulation do not arise from a single mechanism, but rather from a symphony of interconnected physiological pathways operating concurrently across the neuroendocrine system. The most localized effect occurs in the digestive tract through delayed gastric emptying. Peripheral GLP-1 receptors located on gastric smooth muscle actively slow the rate at which food leaves the stomach and enters the duodenum 12. This extended transit time prolongs gastric distension, maximizing the mechanical sensation of fullness during and after meals 1. Simultaneously, GLP-1 enhances the sensitivity of vagal afferent mechanoreceptors in the stomach wall. This amplifies the nerve signals generated by physical stretching, providing a direct, fortified link between the gut's mechanical state and the brain's hormonal interpretation of satiety 1.
However, the most profound driver of weight loss occurs within the central nervous system. Synthetic GLP-1 medications are capable of crossing the blood-brain barrier, allowing them to directly engage with the hypothalamus, the brain's primary control center for energy balance and homeostasis 23. Within the hypothalamic arcuate nucleus, the medication stimulates pro-opiomelanocortin (POMC) neurons, which essentially act as the body's appetite brake pedal. Simultaneously, the drug inhibits neuropeptide Y and Agouti-related peptide (NPY/AgRP) neurons, which function as the physiological gas pedal for intense hunger 23.
Modern pharmaceutical development has expanded upon this single-hormone approach. Dual-agonist medications, most notably tirzepatide, combine GLP-1 receptor activation with glucose-dependent insulinotropic polypeptide (GIP) 3. While GLP-1 acts primarily on the brain and stomach, GIP receptors are highly abundant in adipose (fat) tissue. Activating these GIP receptors appears to directly improve insulin sensitivity within fat cells, facilitating more efficient lipolysis, which is the breakdown of stored fats for energy, while simultaneously reducing the systemic inflammation typically associated with visceral fat accumulation 3.
The 2026 Shift from Injections to Oral Therapies
Historically, GLP-1 receptor agonists were exclusively available as subcutaneous injections. Because they are structurally based on fragile peptide hormones, exposing them to the highly acidic environment of the human stomach would rapidly destroy the active ingredients before they could be absorbed into the bloodstream 1. This delivery method created a natural bottleneck, as needle aversion deterred a significant portion of the eligible patient population from initiating therapy 26.
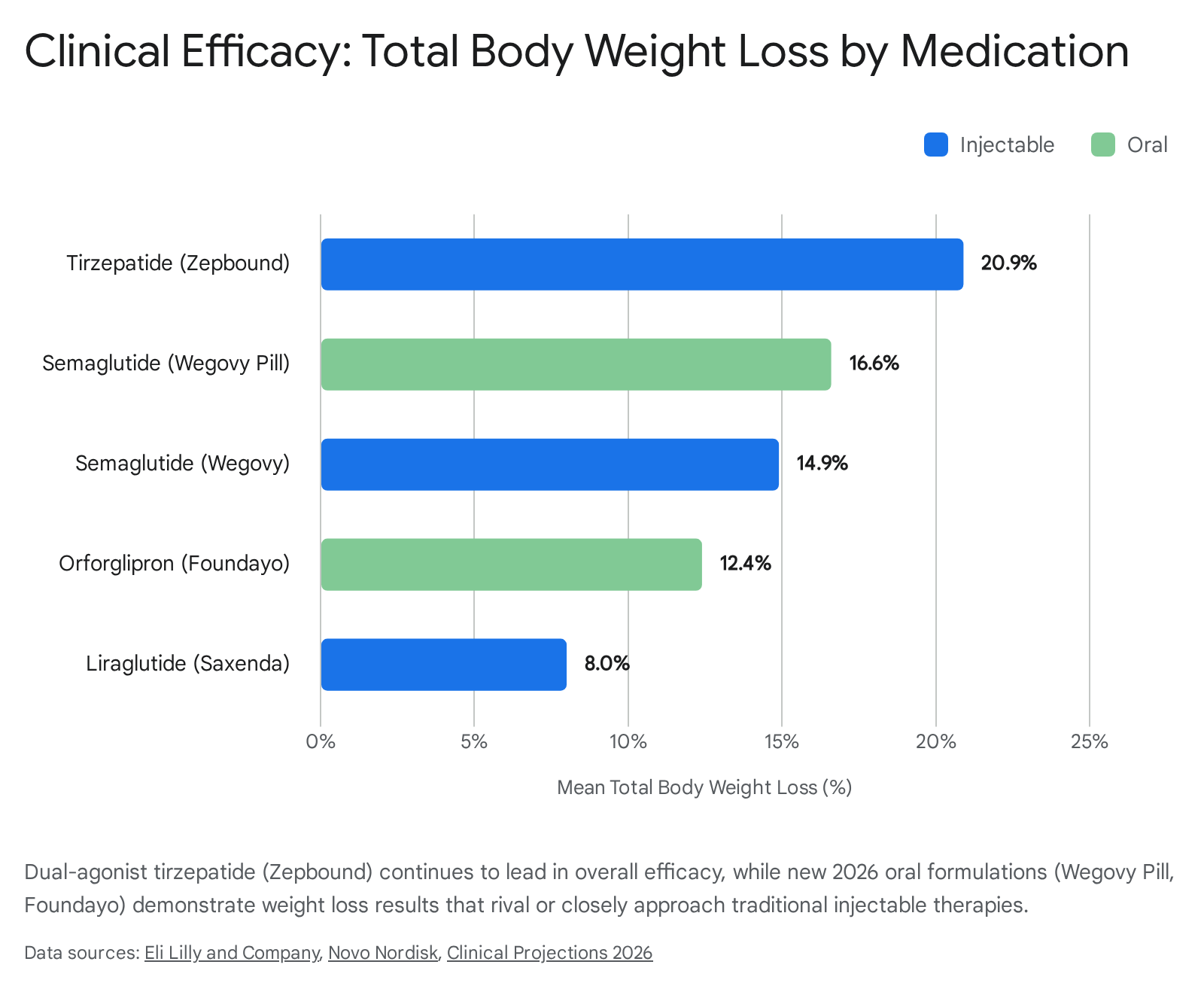
The regulatory landscape transformed dramatically at the beginning of 2026 with the approval of sophisticated oral formulations designed for mass consumer markets. In January 2026, the U.S. Food and Drug Administration approved the Wegovy pill, produced by Novo Nordisk 3. This medication relies on a massive dose of oral semaglutide - 25 milligrams daily, compared to the 2.4 milligram weekly injection - combined with a specialized absorption enhancer that temporarily neutralizes stomach acidity, allowing a sufficient fraction of the peptide to survive digestion and enter the bloodstream 13. The results from the OASIS 4 clinical trial demonstrated that this daily pill achieved a 16.6% mean weight loss over 64 weeks, mirroring the efficacy of its injectable counterpart 13. However, the peptide-based nature of oral semaglutide still requires patients to adhere to strict fasting windows and highly specific fluid intake rules to ensure proper absorption 4.
A secondary, perhaps more disruptive, breakthrough followed in April 2026 with the FDA approval of Eli Lilly's Foundayo, known generically as orforglipron 56. Foundayo represents the first non-peptide, small-molecule oral GLP-1 receptor agonist approved for chronic weight management 46. Because it is a synthetic small molecule rather than a delicate hormone chain, it is remarkably stable in the digestive tract. Patients can take the pill at any time of day, entirely independent of meals or fluid restrictions, fundamentally resolving the adherence barriers associated with previous oral therapies 46.
Clinical trials supporting Foundayo's approval, specifically the ATTAIN-1 study, showed that patients taking the highest dosage lost an average of 12.4% of their body weight, or roughly 27 pounds, over a 72-week period 4. These approvals have dramatically expanded the total addressable market for incretin therapies, opening a new frontier for patients who previously refused injectable medications and cementing projections that the global incretin market will reach $200 billion by 2030 26.
Systemic Benefits Beyond the Scale
While weight reduction remains the primary driver of consumer demand, the medical consensus has firmly repositioned GLP-1 receptor agonists as systemic cardiometabolic and neuropsychiatric therapies. The physiological ripple effects of these medications demonstrate that treating obesity naturally mitigates a constellation of downstream chronic diseases.
Cardiovascular Protection and the SELECT Trial
The most consequential data regarding the long-term health benefits of GLP-1 therapies stems from the SELECT trial, a massive, multi-year outcomes study published in late 2025 and heavily analyzed throughout 2026. The trial tracked 17,604 participants across 41 countries. Crucially, all participants were over the age of 45, had overweight or obesity, and suffered from pre-existing cardiovascular disease, but none had a diagnosis of clinical diabetes 127.
The findings definitively proved that semaglutide offers potent cardiovascular protection independent of its role as a diabetes medication. Participants receiving a 2.4 milligram weekly dose of semaglutide experienced a 20% lower risk of major adverse cardiovascular events (MACE), a composite metric that includes cardiovascular death, nonfatal heart attacks, and nonfatal strokes 128.
Perhaps the most fascinating revelation from the SELECT data was the speed at which these cardiovascular benefits materialized. Kaplan-Meier event curves showed a statistically significant separation between the semaglutide and placebo groups after just three months, and sometimes as early as three weeks into treatment 8. At this early stage, the average weight loss among participants was less than 5% of their total body weight, indicating that the cardiovascular benefits were not simply a byproduct of becoming thinner 8. Detailed mediation analyses confirmed this hypothesis, revealing that early reductions in waist circumference and body weight accounted for only 33% of the observed cardiovascular benefit 910. The remaining cardioprotective effects are likely driven by semaglutide's direct influence on underlying inflammatory pathways, improved vascular endothelial function, and stabilized hemodynamics, establishing the drug as a foundational therapy for cardiovascular risk reduction 1210.
Silencing "Food Noise" and Reshaping Brain Reward Circuits
One of the most frequently reported subjective benefits of GLP-1 therapy is the sudden elimination of "food noise" - the persistent, intrusive, and obsessive mental chatter regarding food planning, cravings, and meal anticipation that plagues many individuals with obesity 1711. Historically dismissed as anecdotal, 2026 clinical research presented at the European Congress on Obesity provided empirical quantification of this psychological phenomenon.
Utilizing the validated Food Noise Questionnaire (FNQ), researchers tracked patients undergoing digital behavioral weight management. The group that initiated GLP-1 therapy alongside behavioral interventions experienced a massive 4.05-point drop in their food noise scores within a single month, compared to a nominal 1.15-point drop in the behavioral-only cohort 1213. This rapid mental relief is increasingly viewed by obesity medicine specialists as a reliable early indicator of overall treatment response 1213.
The mechanism behind this psychological shift lies deep within the brain. Advanced neurobiological studies published in 2026 demonstrated that GLP-1 medications, particularly the newer small-molecule oral variants, penetrate specific circuits connecting the hindbrain to the central amygdala and dopamine-producing neurons 212223. The central amygdala is a region closely associated with desire and reward. When activated by GLP-1 agonists, this circuit actively suppresses the release of dopamine during hedonic feeding - eating purely for pleasure rather than energy demand 23. By blunting the dopamine spike normally triggered by high-calorie foods, the medication effectively strips the "reward value" away from the stimuli, helping patients effortlessly bypass cravings that previously required immense willpower to resist 2122.
Investigating Suicidality and the Anhedonia Risk
Because these medications so directly modulate the brain's reward and motivation pathways, extensive scrutiny has been applied to their broader psychiatric safety profile. Throughout 2023 and 2024, isolated case reports and disproportionality analyses raised alarms regarding a potential link between semaglutide use and severe suicidal ideation, prompting massive regulatory investigations 1415.
By early 2026, both the U.S. Food and Drug Administration and the European Medicines Agency concluded their exhaustive safety reviews, determining there is no causal relationship between GLP-1 receptor agonists and suicidal thoughts or actions 1426. In fact, massive real-world data analyses using Swedish nationwide registry data demonstrated the opposite effect. When comparing patients' periods on GLP-1 therapy versus periods without treatment, researchers found that medication use was strongly associated with reduced clinical anxiety, a lower rate of suicidal behavior, and a significant drop in psychiatric-related sick leave 14.
However, clinical neuropsychiatry is increasingly monitoring a different affective side effect: anhedonia. Because GLP-1s lower dopamine responses to curb food cravings, some patients report a broader emotional blunting or a reduced capacity to experience pleasure in social interactions, hobbies, and daily life 2127. While typically transient as the brain adjusts to new neurochemical baselines, this diminished motivation highlights the profound reach of metabolic drugs into affective neurocircuitry, prompting calls for more precise, targeted drug design in the future 2127.
A New Paradigm for Addiction and Substance Use Disorders
The same dopaminergic modulation that strips the reward value from junk food has positioned GLP-1 receptor agonists as one of the most promising new frontiers in addiction medicine. Preclinical animal models have consistently demonstrated that exposure to GLP-1 agonists reduces the voluntary self-administration of alcohol, cocaine, fentanyl, heroin, and nicotine, signaling a class-wide anti-craving mechanism 1629.
Clinical validation in humans reached a critical milestone in 2026 with a landmark randomized controlled trial published in The Lancet. The study tracked 108 treatment-seeking patients diagnosed with alcohol use disorder (AUD) and comorbid obesity 1718. Participants receiving weekly semaglutide injections alongside cognitive behavioral therapy experienced a 41.1% reduction in heavy drinking days over 26 weeks, performing significantly better than the placebo group 17. Notably, the number needed to treat (NNT) - a standard epidemiological metric indicating how many patients must receive a drug for one to benefit - was calculated at 4.3 for semaglutide in this context, markedly superior to the NNT of 7 or higher seen in older, currently approved AUD medications 17. Given the vast underutilization and limited efficacy of existing addiction pharmacotherapies, federal health authorities are accelerating research into how these metabolic agents can be repurposed to address the ongoing addiction crisis 2917.
Mitigating Physical Side Effects and Muscle Loss
While the benefits of GLP-1 therapies are transformative, they are not achieved without physiological friction. The very mechanisms that induce weight loss - delayed digestion and severe appetite suppression - inevitably disrupt the body's digestive rhythm and body composition. Efficacy on these medications requires proactive, structured dietary and physical interventions.
Managing Gastrointestinal Adjustment
The vast majority of adults initiating GLP-1 therapy experience gastrointestinal adverse events, particularly during the first few months of treatment when the dosage is being gradually increased 19. Common side effects include nausea, vomiting, diarrhea, dyspepsia, and chronic constipation 20. These symptoms are a direct physical consequence of the drug slowing gastric emptying; food literally remains in the stomach longer, increasing the likelihood of reflux and bloating if dietary habits remain unchanged 119.
To minimize discomfort, clinical nutritionists emphasize that patients must abandon traditional three-meal-a-day structures in favor of small, highly frequent meals 192021. High-fat foods, greasy takeaways, and spicy dishes must be heavily restricted, as fat naturally takes longer to digest; combining a high-fat diet with a drug that already delays digestion creates a severe bottleneck that routinely triggers vomiting and belching 192035. Furthermore, because the delayed gastric emptying can disrupt normal bowel motility and patients naturally eat less food overall, constipation is exceedingly common 19. Mitigating this requires a deliberate increase in fluid intake to a minimum of 64 to 80 ounces daily, alongside a structured, gradual increase in dietary fiber 2135.
Combating the Muscle Loss Crisis
The most insidious physical side effect of GLP-1-induced weight loss is the rapid depletion of lean body mass. When appetite is chemically suppressed and patients enter a steep caloric deficit, the body does not exclusively burn fat for energy; it readily catabolizes skeletal muscle and organ tissue to meet its metabolic demands 3637. Exploratory DEXA scan analyses from the foundational STEP 1 clinical trials revealed that approximately 39% of the total weight lost by patients taking semaglutide consisted of lean body mass 3638. Similar data from tirzepatide trials showed lean tissue accounted for 30% to 40% of the total reduction 36. Losing such a massive volume of muscle tissue is perilous, as it significantly lowers the patient's resting metabolic rate, increases the likelihood of rapid weight regain upon discontinuation, and elevates the risk of osteopenia and physical frailty in older adults 3639.
Fortunately, extensive sports medicine research indicates that this muscle loss is preventable if specific countermeasures are strictly implemented during the weight-loss phase. Adherence to a three-pillar protocol can preserve upwards of 90% of a patient's lean mass while actively shedding fat 3637:
- Aggressive Protein Titration: Patients must override their blunted appetites to consume between 1.6 and 2.2 grams of protein per kilogram of body weight daily 3637. For a 180-pound individual, this translates to a rigorous intake of 130 to 180 grams of protein daily, which must be spread across multiple meals to maintain a steady supply of essential amino acids for muscle protein synthesis 3639.
- Mandatory Resistance Training: Diet alone cannot preserve muscle in a severe caloric deficit. Patients must engage in heavy resistance training two to four times per week, focusing on progressive overload and compound movements (e.g., squats, hinges, pushing, and pulling patterns) 363739. Aerobic cardiovascular exercise, while excellent for heart health, does not provide the mechanical tension required to signal the body to retain muscle mass under GLP-1 therapy 3738.
- Controlled Deficit Pacing: The weekly rate of weight loss should be artificially capped at 0.5% to 1.0% of the patient's total body weight. Shedding weight faster than this threshold almost guarantees a disproportionate loss of lean tissue 3637.
Global Economics, Pricing, and Access in 2026
The global availability of GLP-1 therapies reached a turning point in early 2026. Following unprecedented demand that caused rolling shortages from 2022 through 2024, pharmaceutical giants Novo Nordisk and Eli Lilly completed massive manufacturing capability expansions 4041. By the first quarter of 2026, the FDA "Shortage Era" had officially concluded for all dosage strengths of both semaglutide and tirzepatide, transforming an acute supply crisis into a landscape characterized by robust availability 4041.
The International Pricing Disparity
Despite stabilized supply chains, the cost of GLP-1 medications remains one of the most contentious issues in modern healthcare, characterized by stark geographic disparities. The United States continues to shoulder the highest list prices globally, though out-of-pocket costs vary wildly based on an individual's insurance formulary tier and the aggressive use of manufacturer savings coupons 4243.
| Region / Country | Estimated Monthly Out-of-Pocket Cost (Brand-name, without insurance coverage) | Market and Access Dynamics in 2026 |
|---|---|---|
| United States | ~$900 - $1,400 USD 4445 | High list prices are heavily obscured by PBM rebates and manufacturer coupons. Access hinges entirely on commercial insurance coverage mandates. |
| Canada | ~$350 - $700 CAD 44 | Provincial public coverage varies widely. The private-pay market is robust due to list prices being roughly half of the U.S. equivalent. |
| United Kingdom | £150 - £300 GBP 44 | NHS rollout remains highly regulated and phased through specialist clinics, driving intense demand toward an affordable, fast-moving private prescribing market. |
| Germany | €180 - €380 EUR 44 | Highly restrictive public health insurance (GKV) coverage for obesity indications forces the majority of weight-loss patients into the self-pay sector. |
The U.S. Medicare Pivot
A tectonic shift in the American access landscape occurred on July 1, 2026, driven by evolving federal policy and the accumulation of cardiovascular outcome data. Under a newly implemented "most-favored-nation" pricing framework negotiated by the Centers for Medicare & Medicaid Services (CMS), Medicare Part D began providing coverage for brand-name GLP-1 medications for eligible beneficiaries 241.
This federal intervention capped the negotiated monthly Medicare price for prominent drugs like Wegovy and Zepbound at a drastically reduced $245 per month, leaving eligible seniors with a maximum out-of-pocket copay of just $50 monthly 241. Because over 70 million Americans are covered by Medicare, this policy shift immediately enfranchised a massive demographic of older adults who were previously entirely priced out of the obesity medication market, fundamentally accelerating the growth of the U.S. prescription drug sector 2.
The FDA Crackdown on Compounded GLP-1s
During the height of the 2022 - 2024 drug shortages, a massive secondary market emerged in the United States. Under specific exemptions in the Federal Food, Drug, and Cosmetic Act, state-licensed compounding pharmacies were legally permitted to mass-produce unbranded, inexpensive copies of semaglutide and tirzepatide to meet the overwhelming public demand 4647.
However, the resolution of the official FDA drug shortage list triggered a swift and severe regulatory crackdown. By May 2025, the grace periods allowing large-scale 503B outsourcing facilities to mass-compound these peptides expired, rendering bulk production non-compliant 4648. The regulatory environment tightened further on April 30, 2026, when the FDA formally proposed removing semaglutide, tirzepatide, and liraglutide from the 503B bulks list entirely, explicitly stating there was no longer a clinical need for these workarounds since the approved, branded drugs were widely available 474950.
While a narrow legal pathway - known as 503A patient-specific compounding - remains technically legal for individuals with specific, documented medical needs (such as a verified allergy to an inactive ingredient in the commercial pen), the era of widespread, affordable, mass-dispensed compounded GLP-1s facilitated through digital telehealth platforms has effectively been shut down by federal regulators 464850.
The Long Game: Maintenance and Tapering Strategies
Because obesity is fundamentally classified as a chronic, relapsing metabolic disease, the physiological changes induced by GLP-1 medications are not permanent cures. Clinical data unequivocally shows that if a patient abruptly stops taking the medication after reaching their goal weight, their neurochemical appetite signals return to baseline, resulting in the rapid regain of a significant portion of the lost weight 5152.
However, keeping a patient on the highest, most expensive, and most side-effect-heavy maximum dosages indefinitely is practically and financially unsustainable. Throughout 2025 and 2026, clinical trials began defining viable "off-ramps" and maintenance protocols that allow patients to sustain their physiological victories with less burden.
The SURMOUNT-MAINTAIN trial evaluated patients who achieved massive weight loss on the maximum tolerated dose of tirzepatide (Zepbound). Researchers found that patients who stepped their dosage down to a significantly lower 5 milligram maintenance injection successfully preserved nearly all of their prior weight loss over a subsequent one-year period, shedding side effects while maintaining efficacy 51. Similarly, the ATTAIN-MAINTAIN trial demonstrated that patients who transitioned from intense weekly injections over to the daily oral Foundayo pill maintained their new body composition seamlessly, offering a highly flexible and convenient alternative for long-term adherence 51.
For patients paying out of pocket, dose-spacing has emerged as a successful strategy. A retrospective case series from the Scripps Clinic tracked patients who, upon reaching their weight-loss plateau, gradually reduced the frequency of their injections from once a week to once every two, four, or even six weeks. These patients successfully stabilized their skeletal muscle mass, maintained their total weight loss, and preserved all metabolic improvements in blood pressure and HbA1c, proving that structured de-escalation is a safe and highly economical path forward for chronic obesity management 5354.
Bottom line
GLP-1 medications have proven to be much more than simple appetite suppressants; they are potent neuro-metabolic regulators that fundamentally alter brain reward circuits to drive sustained weight loss and provide dramatic cardiovascular protection. While the resolution of historic drug shortages, the arrival of daily oral pills, and expanding Medicare coverage in 2026 have vastly improved access, patients must still navigate complex gastrointestinal side effects and the critical risk of rapid muscle depletion. Long-term success on these medications is rarely passive; it requires a disciplined, lifelong protocol of aggressive protein intake, heavy resistance training, and physician-guided maintenance dosing to preserve both physical health and financial stability once target weights are achieved.