GLP-1 receptor agonists in aging, cognition, and addiction
The landscape of metabolic, neuroendocrine, and preventive medicine has been fundamentally transformed over the past decade by the advent of nutrient-stimulated hormone-based therapeutics. Specifically, the widespread clinical integration of glucagon-like peptide-1 (GLP-1) receptor agonists and dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 receptor agonists has reshaped the foundational algorithms of chronic disease management. Originally developed, tested, and approved for the treatment of type 2 diabetes (T2D) by enhancing glucose-dependent insulin secretion and suppressing glucagon release, these agents have subsequently demonstrated profound efficacy in chronic weight management.
As prescribing volumes have surged globally, longitudinal observation and retrospective analyses have begun to catalog an array of unexpected, pleiotropic benefits extending well beyond these initial metabolic indications. Recent large-scale clinical trials and rigorous pharmacovigilance studies conducted between 2024 and 2026 have illuminated potential applications across a spectrum of systemic pathologies, ranging from the attenuation of neurodegenerative diseases and biological aging to the mitigation of substance use disorders.
However, the rapid expansion of off-label prescribing, fueled by a pervasive public narrative framing these therapeutics as universal panaceas, necessitates intense and objective scientific scrutiny. It is critical for the clinical community to systematically dissect the emerging evidence. This exhaustive report synthesizes the highest levels of current evidence - prioritizing 2023 - 2026 peer-reviewed literature from major journals (e.g., NEJM, JAMA, The Lancet), active Phase 2/3 clinical trial data, and massive retrospective cohort studies - to evaluate the true efficacy, underlying neurobiological mechanisms, and formidable limitations of incretin mimetics in three novel domains: Biological Aging, Cognition, and Addiction. Furthermore, this analysis explores the crucial disparities in global metabolic baselines (particularly within Asian cohorts), the emerging risks of clinical sarcopenia and frailty, and the critical lack of long-term (five-year) safety data for these agents at maximal, obesity-targeted dosages.
Deconstructing the Paradigm: Direct Pharmacological Action vs. Secondary Benefits
A pervasive and often dangerous misconception in both public discourse and primary care prescribing regarding GLP-1 and dual GIP/GLP-1 receptor agonists is the routine conflation of their direct pharmacological effects with the indirect, secondary benefits resulting from massive weight loss. To accurately evaluate the therapeutic potential of these agents for off-label, non-metabolic conditions, it is imperative to explicitly separate these two distinct physiological paradigms 11235.
Indirect Benefits Mediated by Adipose Tissue Reduction
The most rapidly visible and clinically celebrated improvements in patients prescribed high-dose semaglutide or tirzepatide often stem entirely indirectly from the massive reduction of ectopic and visceral adipose tissue. With modern incretin therapies frequently inducing weight loss ranging from 15% to 25% of total body mass, the physiological sequelae are profound but largely mechanical or indirectly systemic 456.
For example, the dramatic reduction of body weight mechanically unloads the skeletal system, resulting in substantial improvements in weight-bearing osteoarthritis symptoms and overall mobility. Furthermore, the reduction in parapharyngeal and cervical adiposity physically widens the upper airway architecture, leading to the marked improvement or complete resolution of obstructive sleep apnea 45. From an immunological perspective, the depletion of visceral fat profoundly alters the systemic adipokine profile. Visceral adiposity functions as a highly active endocrine organ that chronically secretes pro-inflammatory mediators. By shrinking these fat depots, incretin therapies indirectly downregulate systemic interleukins (such as IL-6) and tumor necrosis factor-alpha (TNF-α), simultaneously reducing the hemodynamic burden on the myocardium and improving endothelial function 710. Similar secondary effects are observed in respiratory health; new research presented at the European Congress on Obesity indicates that asthma exacerbations fall by 26% in patients on GLP-1 RAs, largely attributable to the mechanical reduction of thoracic pressure and systemic inflammatory modulation secondary to weight loss 8. These are unequivocally secondary consequences of restoring a negative energy balance, rather than direct actions of the GLP-1 or GIP molecules on the affected respiratory or articular tissues.
Direct Pharmacological Effects on the Brain and Aging Biology
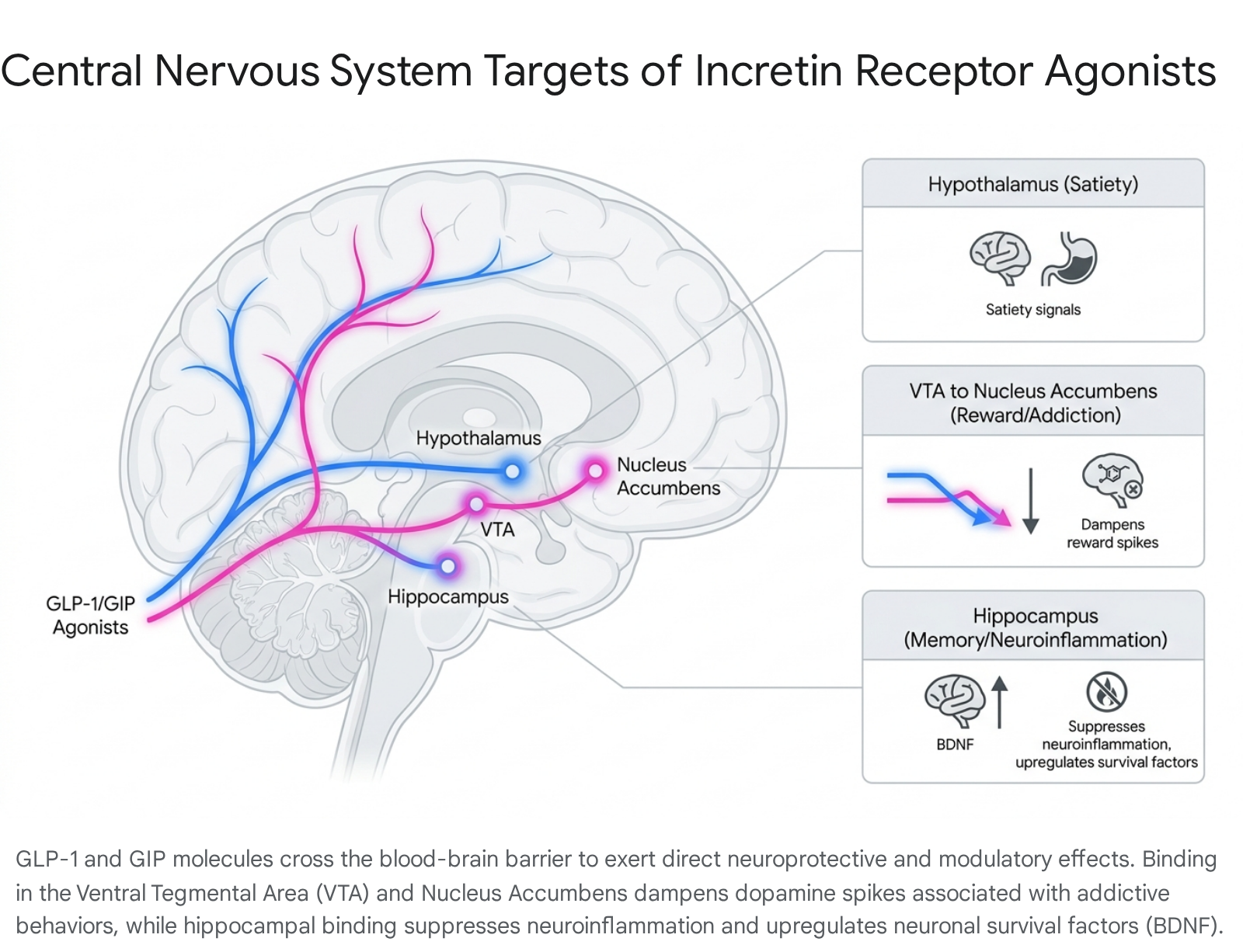
Conversely, the true direct pharmacological effects of incretin mimetics are mediated by the expression and activation of GLP-1 and GIP receptors directly on target tissues, entirely independent of body weight alterations. Central to their efficacy in non-metabolic domains is the ability of GLP-1 receptor agonists to cross the blood-brain barrier (BBB) and directly bind to receptor populations in highly specific regions of the central nervous system (CNS). These include the hypothalamus (which regulates energy homeostasis and satiety), the ventral tegmental area (VTA) and nucleus accumbens (NAc) (which modulate dopaminergic reward and addiction circuitry), and the hippocampus (which heavily influences memory consolidation, synaptic plasticity, and neuroinflammation) 1112.
At the cellular and molecular levels, direct GLP-1 receptor activation on endothelial cells enhances nitric oxide signaling, mitigates reactive oxygen species (ROS) production, and stabilizes atherosclerotic plaques independently of downstream lipid lowering 710. Within the complex context of biological aging and cellular senescence, direct GLP-1 agonism has been shown to suppress nuclear factor-kappa B (NF-κB) - a master regulator of the inflammatory cascade. Activation of these receptors also increases the expression of apurinic/apyrimidinic endonuclease 1 (APE1) to enhance DNA repair mechanisms and activates the PI3K/Akt/mTOR intracellular survival pathways 91415. These direct, receptor-mediated actions attenuate cellular senescence and apoptosis regardless of the patient's baseline adiposity or the magnitude of subsequent weight loss 914. Recognizing this mechanistic divergence is fundamentally essential when evaluating these drugs for neurocognitive, psychiatric, or longevity-focused interventions, where weight loss may not be the primary therapeutic goal and, in some cases, may even be contraindicated.
Comparative Pharmacology and Clinical Efficacy: Semaglutide vs. Tirzepatide
The contemporary clinical landscape is currently dominated by two distinctly engineered pharmacological approaches: semaglutide, a highly selective GLP-1 receptor agonist, and tirzepatide, a dual GIP and GLP-1 receptor agonist. The deliberate addition of GIP receptor agonism in the tirzepatide molecule synergistically enhances glucose-dependent insulin secretion, exerts independent effects on lipid metabolism, further suppresses centrally mediated appetite, and fundamentally alters adipose tissue partitioning in ways that a selective GLP-1 agonist cannot achieve alone 12161718.
Recent head-to-head clinical trials and large retrospective cohorts have established highly significant clinical disparities between the two agents. The SURMOUNT-5 Phase 3b open-label randomized clinical trial provided definitive comparative data for weight loss in adults with obesity or overweight, explicitly excluding those with diabetes. At 72 weeks, participants treated with tirzepatide (Zepbound) yielded an average body weight loss of 20.2% (50.3 lbs), compared to 13.7% (33.1 lbs) for those treated with semaglutide (Wegovy) 41920. This translates to a 47% greater relative weight loss efficacy for the dual agonist. Furthermore, in a key secondary endpoint of SURMOUNT-5, 31.6% of patients on tirzepatide achieved at least a massive 25% reduction in total body weight, nearly double the 16.1% achievement rate observed in the semaglutide arm 20.
Real-world epidemiological evidence heavily corroborates these tightly controlled trial findings. A rigorously designed 2024 cohort study published in JAMA Internal Medicine, involving 18,386 propensity-matched patients, revealed that individuals receiving tirzepatide were significantly more likely to achieve clinically meaningful weight loss across all progressive thresholds 101112. At the one-year mark, hazard ratios (HR) heavily favored tirzepatide for 5% weight loss (81.8% achievement for tirzepatide vs. 66.5% for semaglutide; HR 1.76), 10% weight loss (62.1% vs. 37.1%; HR 2.54), and 15% weight loss (42.3% vs. 18.1%; HR 3.24) 101112. These treatment effects were observed consistently across subgroups, regardless of underlying T2D status.
However, while the sheer metabolic efficacy of dual agonism appears superior in the domains of weight reduction and glycemic control (with tirzepatide frequently reducing HbA1c by 2.0% to 2.5%, compared to semaglutide's 1.0% to 2.0% reduction), the precise differences in long-term hard cardiovascular endpoints - specifically Major Adverse Cardiovascular Events (MACE) - remain under active investigation 418. Semaglutide currently possesses a highly established longitudinal safety database for cardiovascular risk reduction, proven in trials such as SELECT for both primary and secondary prevention 416. Tirzepatide's CVOTs (such as the SURPASS-CVOT trial, which demonstrated noninferiority to dulaglutide but narrowly missed statistical superiority) are still maturing 418.
Table 1: Contrast of Mechanisms and Emerging Clinical Data: Semaglutide vs. Tirzepatide
| Feature / Clinical Domain | Semaglutide (Ozempic, Wegovy, Rybelsus) | Tirzepatide (Mounjaro, Zepbound) |
|---|---|---|
| Receptor Target | Selective GLP-1 receptor agonist 121617 | Dual GLP-1 and GIP receptor agonist 121617 |
| Maximal Clinical Weight Loss | ~13.7% - 15.0% (at 2.4 mg weekly) 1920 | ~20.2% - 25.0% (at 15 mg weekly) 51920 |
| Glycemic Control (HbA1c) | Substantial reduction (1.0% - 2.0%) 4 | Superior reduction (2.0% - 2.5%) 418 |
| Cardiovascular Outcomes | Proven MACE reduction in T2D and non-T2D obesity (SELECT trial) 41618 | MACE reduction trials ongoing (SURPASS-CVOT showed noninferiority to dulaglutide) 418 |
| Neuroprotective Signal (Real-World) | Associated with lower dementia risk 1314 | Associated with significantly lower MCI and stroke risk compared directly to semaglutide 1314 |
| Body Composition Nuance | Emerging preprint data suggests a potentially better lean mass preservation ratio during active weight loss 26 | Induces greater absolute fat loss, but commands stricter monitoring for accelerated lean mass reduction 2615 |
The Sarcopenia Paradigm: Body Composition, Bone Density, and Frailty Risk
As the absolute magnitude of weight loss achievable with high-efficacy agents like tirzepatide approaches, and occasionally matches, that of bariatric surgery, endocrinologists and geriatricians are raising profound concerns regarding the qualitative composition of that weight loss. While total body mass reduction is the primary therapeutic objective for mitigating metabolic syndrome, the concurrent and disproportionate loss of fat-free mass (FFM) - specifically skeletal muscle tissue and bone mineral density (BMD) - poses severe long-term risks for clinical sarcopenia, functional impairment, and frailty 182615.
The human body's physiological adaptations to the extreme caloric deficits induced by profound, incretin-mediated appetite suppression inevitably involve muscle catabolism. Emerging body composition data derived from DXA (dual-energy X-ray absorptiometry) scans embedded within clinical trials indicate that up to 25% to 40% of the total weight lost on high-dose incretin therapies may consist of lean body mass 151629. If this steep trajectory of muscle degradation is maintained over half a decade, particularly in older adults, patients with low baseline muscle mass, or those in prefrail states, the pharmacological cure for their obesity may inadvertently precipitate advanced age-related functional decline. The loss of metabolically active skeletal muscle combined with diminished skeletal loading reduces BMD, drastically heightening fall risk, accelerating osteoporosis, and ultimately compromising long-term metabolic resilience 3182629.
Recent clinical debate has centered around the differential preservation of lean mass between the two leading agents. Preliminary, albeit currently unpublished, preprint data has signaled that semaglutide may preserve lean body mass more effectively than tirzepatide during periods of rapid weight loss. This difference is hypothesized to stem from tirzepatide's distinct impact on tissue partitioning driven by its GIP receptor agonism, which may aggressively mobilize both fat and lean stores when caloric intake plummets 26. While these findings remain unverified by peer review and must be interpreted with intense clinical caution, they highlight a critical paradigm shift.
Regardless of the specific agent chosen, the medical community is increasingly acknowledging that sole reliance on Body Mass Index (BMI) or total body weight as longitudinal clinical benchmarks is dangerously reductive 1826. Modern obesity management mandates the routine incorporation of body composition assessments to rigorously track specific fat-to-muscle ratios over time 2615. Mitigation strategies - most notably, mandatory, supervised resistance training regimens and highly optimized, protein-sparing dietary protocols - must become non-negotiable concomitant therapies to protect bone microarchitecture and muscle reserves from the immense catabolic stress induced by GLP-1/GIP receptor agonism 1830.
Neurobiology of Addiction: Modulating the Mesolimbic Dopamine Circuit
Perhaps the most culturally and scientifically profound intersection of metabolic hormones and psychiatric disease represents one of the most promising frontiers for GLP-1 receptor agonists: addiction medicine. Over the past several years, real-world pharmacovigilance reports and vast swathes of patient anecdotes have consistently highlighted a striking phenomenon. Patients treated with incretin mimetics for diabetes or obesity frequently report a sudden, virtually effortless cessation of compulsive behaviors. This dampening of "food noise" has been observed to cascade into the cessation of alcohol consumption, tobacco smoking, illicit opioid use, and even non-substance behavioral addictions such as compulsive gambling or shopping 3132.
The Dopaminergic Mechanism
The biological plausibility for these profound anti-addictive effects lies deep within the brain's neurocircuitry, specifically within the reward architecture. The mesolimbic pathway, originating in the ventral tegmental area (VTA) and projecting heavily to the nucleus accumbens (NAc), regulates dopamine release in response to rewarding and salience-inducing stimuli, including both highly palatable foods and drugs of abuse 3117.
Through extensive mapping, researchers have identified that GLP-1 receptors are highly expressed throughout these specific midbrain regions. Preclinical primate and rodent models have definitively demonstrated that the central administration of GLP-1 analogues directly dampens the pathological dopamine spikes in the NAc that are normally triggered by the self-administration of cocaine, fentanyl, heroin, nicotine, and alcohol 171819. By modulating these neural circuits, GLP-1 therapies effectively extinguish the neurochemical reinforcement of the substance 3117. Importantly, instead of inducing anhedonia or aversive reactions, GLP-1 RAs appear to restore physiological homeostasis to a severely dysregulated reward system. They simply blunt the obsessive craving and impulsive drive that pulls patients toward the object of their addiction, replicating the satiation response universally across various substance modalities 20.
Emerging Clinical Evidence
Human clinical data regarding addiction is rapidly moving from observational curiosity to rigorously controlled empirical science. In a landmark Phase 2 randomized controlled clinical trial involving 108 treatment-seeking patients with severe alcohol use disorder (AUD) and comorbid obesity, once-weekly administration of semaglutide, combined with standard cognitive behavioral therapy, yielded dramatic results. Over a 26-week period, patients receiving semaglutide achieved a 41.1% reduction in heavy drinking days - a statistically significant 13.7% greater reduction than those receiving placebo alongside therapy 2138.
At the epidemiological level, massive retrospective cohort analyses are cementing these findings across a broader spectrum of substances. A highly powered 2026 cohort study, published in The BMJ, analyzed health records from over 600,000 U.S. veterans with T2D. The study demonstrated that a GLP-1 prescription was associated with a 14% lower relative risk of developing any new substance use disorder compared to patients prescribed non-GLP-1 antidiabetic medications 3120. When stratified by specific substance, the risk of developing an incident disorder declined by 18% for alcohol, 14% for cannabis, 20% for cocaine and nicotine, and 25% for opioids 20. More critically for public health, among patients with a pre-existing opioid use disorder (OUD), the initiation of GLP-1 therapy correlated with a massive 40% drop in opioid overdoses in the first month, alongside significantly lower long-term rates of hospitalization and suicidal ideation 3132.
The "Cure-All" Fallacy: Critiques from Neurologists and Addiction Specialists
Despite the overwhelming biochemical optimism and the tantalizing clinical data, neurologists and addiction specialists caution vehemently against the rising public narrative framing GLP-1s as a pharmacological "cure-all" or "magic bullet" for addiction. Critics from within the psychiatric and addiction medicine communities emphasize that while GLP-1 RAs may effectively modulate the physiological craving and neurobiological reward loop, they absolutely do not address the complex structural, psychological, and socioeconomic root causes of substance abuse 3940.
Addiction is frequently a deeply entrenched coping mechanism for underlying trauma, generational poverty, food insecurity, and chronic clinical depression 39. A purely pharmacological intervention that numbs the craving without accompanying psychosocial support, housing stability, trauma counseling, and comprehensive psychiatric care risks creating a temporary metabolic band-aid that masks a deeper wound 3940. Furthermore, real-world attrition rates for GLP-1 therapies remain stubbornly high due to chronic gastrointestinal intolerability (nausea, vomiting, gastroparesis) and insurmountable financial cost barriers 103922. This raises acute concerns regarding rebound cravings and heightened overdose risk if an addicted patient abruptly loses access to the medication, as their unaddressed trauma remains intact while the pharmacological suppression suddenly vanishes.
The prevailing consensus among specialists is that incretin mimetics should be viewed as powerful adjuncts - potentially replacing or complementing legacy treatments like buprenorphine, methadone, or naltrexone - rather than standalone cures. True recovery requires the patient to build a life where they do not need to self-medicate, a goal no peptide can achieve in isolation 311839.
Cognition, Neuroinflammation, and the Alzheimer's Paradox
The compelling hypothesis that GLP-1 receptor agonists could alter the devastating trajectory of neurodegenerative diseases, particularly Alzheimer's Disease (AD) and Parkinson's Disease (PD), stems from their proven ability to cross the BBB and exert profound, direct neuroprotective effects. The mechanisms of action in the brain are extensive: they include the activation of the PI3K/Akt/mTOR signaling pathways (promoting neuronal survival and anti-apoptotic cascades), the robust upregulation of brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF), the reduction of reactive oxygen species (ROS), and the intense suppression of neuroinflammation via microglial inhibition 123. Furthermore, because severe insulin resistance in the brain is a well-recognized pathological feature of AD (frequently prompting researchers to dub the condition "type 3 diabetes"), restoring cerebral glucose metabolism and energy conversion via central GLP-1 signaling provided a highly compelling therapeutic rationale for intervention 169.
Retrospective Successes vs. Prospective Trial Failures
Initial retrospective electronic health record (EHR) studies tracking patients over several years were highly encouraging, seeming to validate the neuroprotective hypothesis. A massive, real-world cohort analysis published in JAMA Network Open evaluated adults with T2D taking semaglutide or tirzepatide. The study found that users of incretin therapies exhibited significantly lower risks of developing mild cognitive impairment (MCI), all-cause dementia, and ischemic stroke compared to closely matched cohorts on other antidiabetic agents 1314. Interestingly, within this study, tirzepatide demonstrated a notably stronger protective signal against the onset of MCI (Relative Risk 0.12) and stroke than semaglutide. This disparity is likely attributable to the synergistic neuroprotective effects of GIP agonism, which independently regulates neurotransmitter release and has been shown to promote hippocampal stem cell proliferation 11314.
However, the attempt to translate these promising retrospective correlations into prospective, randomized, double-blind Alzheimer's clinical trials has resulted in a stark and sobering reality check for the field. In late 2025, at the Clinical Trials on Alzheimer's Disease (CTAD) conference, Novo Nordisk presented the highly anticipated full results of the Phase 3 EVOKE and EVOKE+ trials. These trials evaluated oral semaglutide (at a dose of 14 mg daily) in 3,808 patients with early-stage symptomatic Alzheimer's disease (mild cognitive impairment or mild dementia with confirmed amyloid pathology) over a period of up to three years 64223.
The trials were an unequivocal clinical failure. Over the duration of the study, oral semaglutide completely failed to demonstrate any significant slowing of cognitive or functional decline compared to placebo, as measured by the primary endpoint, the Clinical Dementia Rating-Sum of Boxes (CDR-SB) 422324. For every primary and secondary cognitive and functional outcome, the progression curves for the semaglutide and placebo groups were virtually indistinguishable 24. Vexingly, while the drug did appear to induce nominally significant shifts in certain Alzheimer's fluid biomarkers in the cerebrospinal fluid (CSF) - indicating some degree of biological target engagement and reduced neuroinflammation - these biological shifts absolutely did not translate into any measurable clinical or cognitive benefit for the patients 4224.
Neurologist Skepticism and the Path Forward
The glaring mismatch between the retrospective data suggesting prevention and the EVOKE trial failure demonstrating an inability to treat has sparked intense analysis and skepticism among neurologists. Many leading experts argue that a single-agent metabolic drug is fundamentally insufficient to halt or alter the course of a disease driven by deeply entrenched amyloid-beta and tau protein pathology once overt clinical symptoms have appeared 4225.
The EVOKE failure underscores a critical, sobering reality in neuropharmacology: while GLP-1 RAs may effectively prevent or significantly delay the onset of dementia in metabolically diseased, pre-symptomatic populations (as seen in the TriNetX and VA retrospective cohorts), they are not capable of rescuing degenerating neurons or restoring lost synaptic connections in patients who already have established, symptomatic Alzheimer's disease 642. Consequently, the future of neurodegenerative pharmacotherapy will likely necessitate precision combination therapies. This would involve pairing targeted anti-amyloid monoclonal antibodies (such as lecanemab or donanemab) designed to clear existing plaques, with GLP-1 RAs designed to simultaneously quench background neuroinflammation and improve metabolic resilience in the surviving neural tissue 4223.
Cellular Senescence and the Hallmarks of Aging
Moving beyond distinct disease pathologies, GLP-1 receptor agonists are increasingly being viewed and evaluated through the lens of geroscience as potent, systemic anti-aging agents. Biological aging is not a single disease, but rather is driven by a series of interconnected, foundational biological processes known as the "hallmarks of aging." These include genomic instability, epigenetic alterations, mitochondrial dysfunction, altered nutrient sensing, stem cell exhaustion, and cellular senescence 51526. A pervasive state of chronic, low-grade systemic inflammation, highly prevalent in older adults and individuals with obesity - termed "inflammaging" - serves as an accelerant, driving telomere attrition, mutagenesis, and tissue degradation 1415.
Recent multi-omic studies evaluating the effects of GLP-1 signaling in aged animal models have revealed remarkable evidence of body-wide physiological rejuvenation. In a prominent 2024 study published in Cell Metabolism, researchers demonstrated that chronic administration of the GLP-1RA exenatide in aged mice effectively counteracted molecular aging signatures across transcriptomic, epigenetic, and metabolomic layers 2927. Crucially, the treated mice exhibited progressive improvements in forelimb grip strength and motor function compared to the placebo group 27.
What makes these findings profoundly significant is that this biological reversal occurred in a largely weight-neutral context. This proves that the age-counteracting effects were directly mediated via central GLP-1 signaling (specifically showing a strict hypothalamic dependence) rather than merely being the secondary consequence of shedding adipose tissue 27. By attenuating ROS production, suppressing the NF-κB inflammatory pathway, and actively preserving the efficiency of DNA repair enzymes, GLP-1 therapies directly intervene in the molecular pathogenesis of cellular senescence. Theoretically, by targeting these multiple overlapping pathways - improving mitochondrial energy production, reducing chronic inflammation, and stabilizing genomic integrity - these agents hold the potential to significantly extend the overall "healthspan" (the period of life lived free from chronic disease) of the human organism 91415.
Global Heterogeneity: Asian Cohorts and MACE Disparities
The clinical efficacy, long-term outcomes, and establishing prescribing paradigms of GLP-1 RAs are highly sensitive to genetic lineage, geography, and global metabolic variations. Observational data and randomized cardiovascular outcome trials (CVOTs) have consistently demonstrated that East and South Asian populations exhibit markedly distinct metabolic responses to incretin therapy when compared to Western, predominantly White populations.
In a massive 2026 meta-analysis of nine randomized placebo-controlled CVOTs (including the recent, large-scale SOUL trial) encompassing 8,164 Asian, 4,036 Black or African American, and 62,503 White participants, GLP-1 RAs were definitively shown to reduce Major Adverse Cardiovascular Events (MACE) across diverse populations. However, the magnitude of the cardiovascular risk reduction was significantly greater in Asian cohorts. The pooled Hazard Ratio (HR) for MACE in Asian populations was a striking 0.73, compared to a more modest HR of 0.86 in White populations 282930. Furthermore, the pooled absolute risk reduction for MACE was 2.9% in Asian patients versus only 1.4% in White patients, yielding a Number Needed to Treat (NNT) of 35 for Asians compared to 73 for Whites 29.
This stark disparity highlights a fundamentally different baseline metabolic architecture. Due to genetic and phenotypic differences in fat distribution, Asian populations generally develop highly pathogenic visceral adiposity, severe insulin resistance, and atherosclerotic cardiovascular disease at significantly lower total body weights and BMIs than Caucasian populations 2931. Consequently, the diagnostic criteria and prescribing thresholds for obesity medications in Asian countries are radically different from those established by the US FDA or the European EMA.
For instance, in South Korea and Taiwan, severe obesity is frequently defined as a BMI ≥ 30 kg/m2, rather than the Western standard of ≥ 35 kg/m2 or 40 kg/m2. Moreover, GLP-1 therapies like Wegovy and Mounjaro are often legally indicated and prescribed for Asian patients with a BMI of 27 kg/m2 presenting with comorbidities - or even a BMI as low as 25 kg/m2 under certain regional guidelines 3132. Applying standard Western BMI thresholds (such as >30 kg/m2 for uncomplicated obesity) universally fails to capture the high-risk metabolic phenotypes present in globally diverse populations. This underscores the absolute necessity for nuanced, region-specific guidelines and localized clinical trials in global obesity management to ensure equitable access to cardiovascular protection 31.
Pharmacovigilance and the Five-Year High-Dose Data Gap
Despite the pervasive clinical euphoria surrounding the pleiotropic benefits of GLP-1 and dual GIP/GLP-1 receptor agonists, a critical and potentially dangerous blind spot remains glaringly apparent in the current clinical literature: the explicit lack of actual five-year (or longer), prospective safety data for these drugs when utilized at the maximum dosages specifically approved for chronic weight management (e.g., semaglutide at 2.4 mg/week and tirzepatide at 15 mg/week).
While the short- and medium-term safety profiles (spanning 1.5 to 3 years) have been extensively and rigorously characterized in massive Phase 3 programs like the STEP, SURMOUNT, and SELECT trials, and a decade of safety data exists for the significantly lower T2D doses (e.g., semaglutide 1.0 mg or liraglutide), extrapolating low-dose safety profiles to high-dose, lifelong, continuous therapy is scientifically perilous 333455.
Global pharmacovigilance databases, such as the FDA Adverse Event Reporting System (FAERS), are already beginning to flag highly concerning safety signals associated with these newer, more potent agents. These include severe gastrointestinal motility disorders leading to clinical gastroparesis (stomach paralysis), and significantly increased risks of rare optic neuropathies, specifically non-arteritic anterior ischemic optic neuropathy (NAION), which can lead to permanent vision loss 51835. Furthermore, as previously discussed, the unquantified long-term consequences of maintaining a highly catabolic state on bone microarchitecture and skeletal muscle reserves over a decade remain entirely unknown.
The rapid expansion of off-label use for aging, cognition, and addiction is occurring in an environment where the ultimate physiological cost of chronic, high-dose incretin receptor saturation is still being calculated. Until large-scale, 5-to-10-year longitudinal registries of patients strictly on maximum-dose tirzepatide and semaglutide mature and publish their findings, clinicians prescribing these medications outside of their core metabolic indications are effectively operating without a definitive, long-term safety net 3335.
Summary of Clinical Evidence for Novel Domains
To encapsulate the current therapeutic frontier, Table 2 summarizes the highest level of clinical evidence supporting the use of incretin mimetics in the three highly anticipated domains outside of traditional glycemic and weight control.
Table 2: Evidence Landscape for Novel GLP-1/GIP Applications
| Novel Clinical Domain | Highest Level of Current Evidence | Key Findings & Trial Status (2024-2026 Data) | Clinical Limitations & Future Outlook |
|---|---|---|---|
| Addiction & SUDs | Phase 2 RCTs; Massive Retrospective Cohort Studies 322021 | 41.1% reduction in heavy drinking (Phase 2); 14-25% reduction in new SUD diagnoses in 600k VA cohort. Direct modulation of mesolimbic dopamine 2021. | Structural/psychosocial factors of addiction remain unaddressed. Phase 3 trials are desperately needed. High discontinuation rates may precipitate severe relapse 3940. |
| Cognition & Alzheimer's | Large Retrospective Cohorts; Failed Phase 3 RCTs 134223 | Retrospective EHR data shows significantly lower MCI/Dementia risk 13. EVOKE/EVOKE+ Phase 3 trials unequivocally failed to slow cognitive decline in early AD 4223. | Monotherapy is insufficient for established amyloid/tau-driven AD. May only be viable as early, preventive neuroprotection rather than acute symptomatic treatment 4225. |
| Biological Aging | Preclinical Multi-omic Models; Observational Biomarker Data 141527 | Aged animal models show weight-neutral reversal of transcriptomic/epigenetic aging. Reduces DNA damage markers and suppresses systemic inflammaging 1427. | Complete lack of dedicated human longevity RCTs. It remains highly difficult to separate direct anti-aging effects from general metabolic improvement in human subjects 527. |
Conclusion
The evolution of GLP-1 and dual GIP/GLP-1 receptor agonists from single-purpose anti-diabetic agents to systemic metabolic, cardiovascular, and neurobiological modulators is unequivocally a watershed moment in the history of contemporary medicine. The ability of molecules like tirzepatide and semaglutide to directly cross the blood-brain barrier to suppress neuroinflammation, extinguish the neurochemical dopamine reinforcement of addiction, and theoretically attenuate the cellular hallmarks of biological aging provides a tantalizing, biologically plausible glimpse into the future of unified, multi-system pharmacotherapy.
However, the medical and scientific communities must rigorously guard against the seductive "cure-all" narrative that currently dominates public discourse. The catastrophic clinical failure of the massive EVOKE Alzheimer's trials serves as a stark, empirical reminder that while these agents can brilliantly correct metabolic dysfunction and delay systemic physiological decline, they cannot unilaterally reverse entrenched, structural pathologies once symptoms manifest. Furthermore, the very real risks of inducing clinical sarcopenia, the nuanced complexities of global metabolic diversity requiring tailored BMI thresholds, and the glaring, critical absence of five-year high-dose safety data demand an immediate paradigm shift. Primary care and specialty prescribing must move away from aggressive, indiscriminate off-label use toward precise, body-composition-monitored, and multimodal patient care. The true, lasting potential of incretin mimetics lies not in their mythical status as standalone panaceas, but rather as extraordinarily powerful, foundational pillars integrated within comprehensive, holistic treatment paradigms.