The Science of Brain-Computer Interfaces in 2026
The year 2026 marks a structural transition for brain-computer interface (BCI) technology, shifting the field from proof-of-concept academic research to commercial clinical application and regulated industrial ecosystems. Early generations of BCIs, dominated by systems like the Utah Array, established the foundational neuroscience of decoding motor intent but were constrained by hardwired transcutaneous connections, low spatial resolution, and signal degradation resulting from the central nervous system's foreign body response 12. In contrast, the current landscape is defined by fully implantable, wireless systems leveraging microfabrication, advanced material science, and high-density electrode arrays.
This maturation is evidenced by major clinical and regulatory milestones achieved across the globe. In early 2026, the Chinese National Medical Products Administration (NMPA) granted the world's first commercial approval for an implantable BCI medical device, the epidural NEO system 34. Concurrently, United States and European clinical trials for deeply penetrating arrays and endovascular stents have expanded their patient cohorts, accumulating tens of thousands of hours of chronic recording data 456. Investment in the sector has accelerated rapidly, punctuated by funding rounds such as Neuralink's $650 million Series E and Inbrain Neuroelectronics' $50 million Series B, which are driving the transition from boutique laboratory production to automated, high-volume manufacturing 478.
Despite these advancements, the reality of BCI capability in 2026 diverges sharply from popularized concepts of consumer telepathy or cognitive enhancement. The clinical reality remains tightly focused on restoring functional independence - specifically communication, cursor control, and robotic limb manipulation - for patients with severe paralysis, amyotrophic lateral sclerosis (ALS), and spinal cord injuries (SCI) 910. Furthermore, the fundamental biological hurdle of integrating abiotic materials into the neuroinflammatory environment of the brain continues to dictate device longevity and signal fidelity 1112.
Architectural Approaches to Neural Interfacing
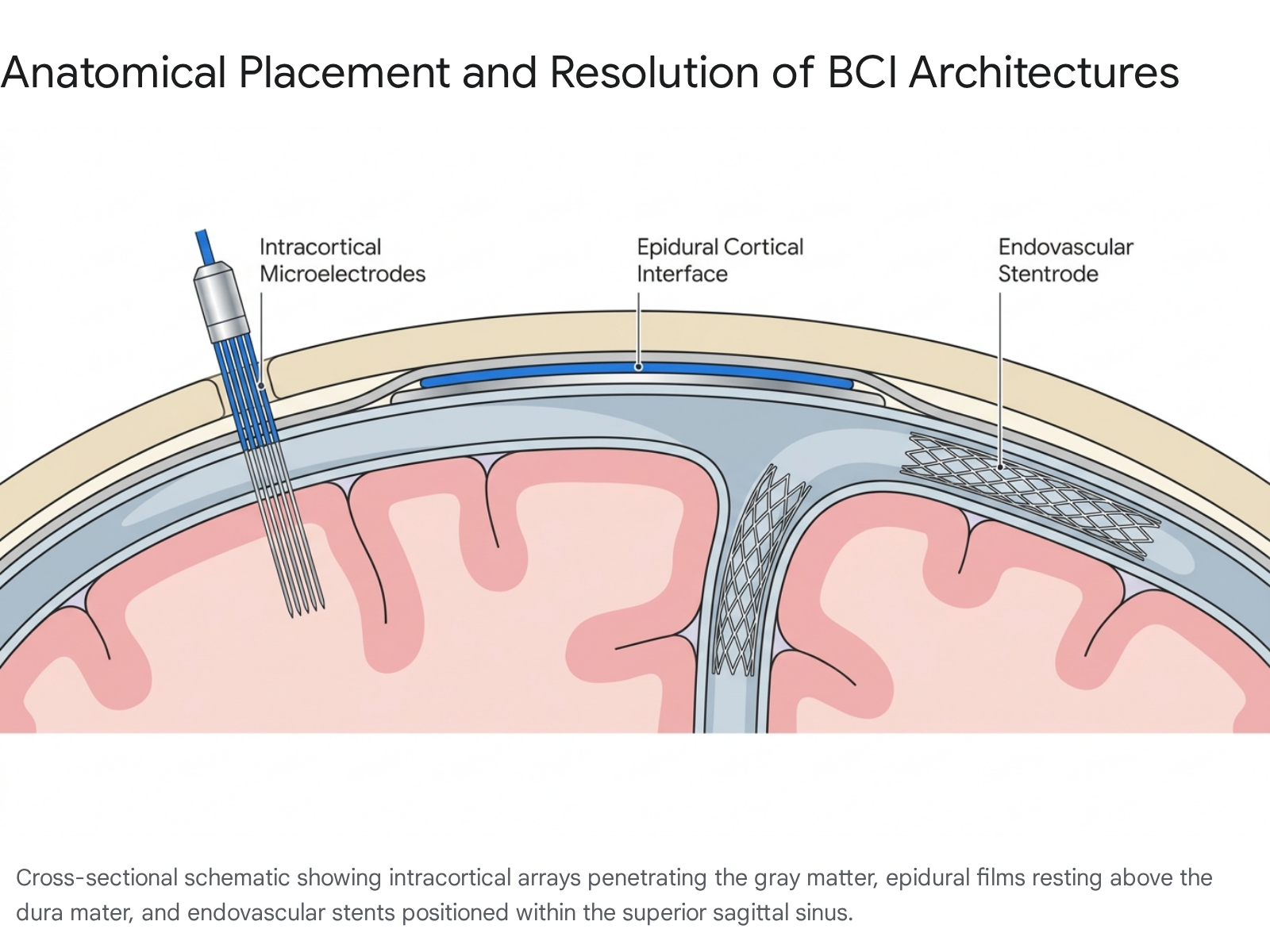
The central engineering challenge of BCI design is balancing signal fidelity against surgical invasiveness and long-term tissue damage. Systems that penetrate deep into the cortex access high-resolution, single-neuron action potentials but trigger the most severe immune responses. Systems that rest on the surface of the brain or within blood vessels minimize tissue damage but record lower-resolution, population-level field potentials. The industry in 2026 is sharply divided into three primary architectural approaches based on physical placement.
Intracortical Microelectrode Systems
Intracortical systems involve an open craniotomy and direct penetration of the pia mater into the cortical gray matter. This microscopic proximity allows the electrodes to detect extracellular voltage changes generated by individual neuron action potentials, commonly referred to as spikes 1314. Single-unit recording provides the highest possible information transfer rate (ITR) and is essential for decoding complex, high-degree-of-freedom motor intent, such as naturalistic speech production or fine digit manipulation on a robotic prosthesis.
Historically, this category was defined by the Utah Array, a rigid silicon microelectrode grid containing 96 to 128 channels. The Utah Array has been implanted in humans for nearly two decades, generating over 30,000 collective days of human clinical data and serving as the backbone for major academic milestones 215. However, its rigid architecture causes mechanical shear against the soft, pulsating tissue of the brain, leading to aggressive scar tissue encapsulation and progressive signal loss over several years 21516. To address these mechanical limitations, the current generation of intracortical devices utilizes ultra-flexible polymer microwires and drastically higher channel counts.
Epidural and Subdural Surface Interfaces
Surface arrays rely on the principles of electrocorticography (ECoG). These devices are inserted beneath the skull but generally sit outside the brain tissue, either above the dura mater (epidural) or just beneath it (subdural). Because they do not penetrate the cerebral cortex, they largely bypass the severe microglial immune response that degrades intracortical electrodes 1718.
The primary biological trade-off is a lower signal-to-noise ratio (SNR). The insulating layers of cerebrospinal fluid, pia mater, and dura mater diffuse the electrical signals before they reach the sensors 19. Consequently, surface arrays capture local field potentials (LFPs) - the synchronized firing of thousands of neurons - rather than discrete single-unit spikes. While insufficient for ultra-fast, phoneme-level speech decoding, high-density ECoG data can reliably decode broader motor intentions for cursor control and functional limb movement without the same level of surgical risk or chronic tissue damage 15.
Endovascular Interfaces
The least invasive modality borrows techniques from interventional neurology and cardiology. An endovascular BCI, typically a stent-mounted electrode array, is navigated through the jugular vein and deployed in the superior sagittal sinus, a major draining vein running adjacent to the motor cortex 152021. The device expands and records neural activity transvascularly through the vein wall.
This approach completely avoids open craniotomies and direct brain tissue trauma, drastically reducing perioperative risk and making the procedure comparable to routine stent placements. However, the physical distance from the target neurons limits signal acquisition primarily to broad gamma and high-gamma frequency bands, yielding lower bandwidths suitable for basic, discrete digital commands (such as clicking or simple cursor navigation) rather than fluid, complex articulation 23.
| Developer | Device Architecture | Electrode Count | Surgical Delivery Method | Target Clinical Status (Mid-2026) |
|---|---|---|---|---|
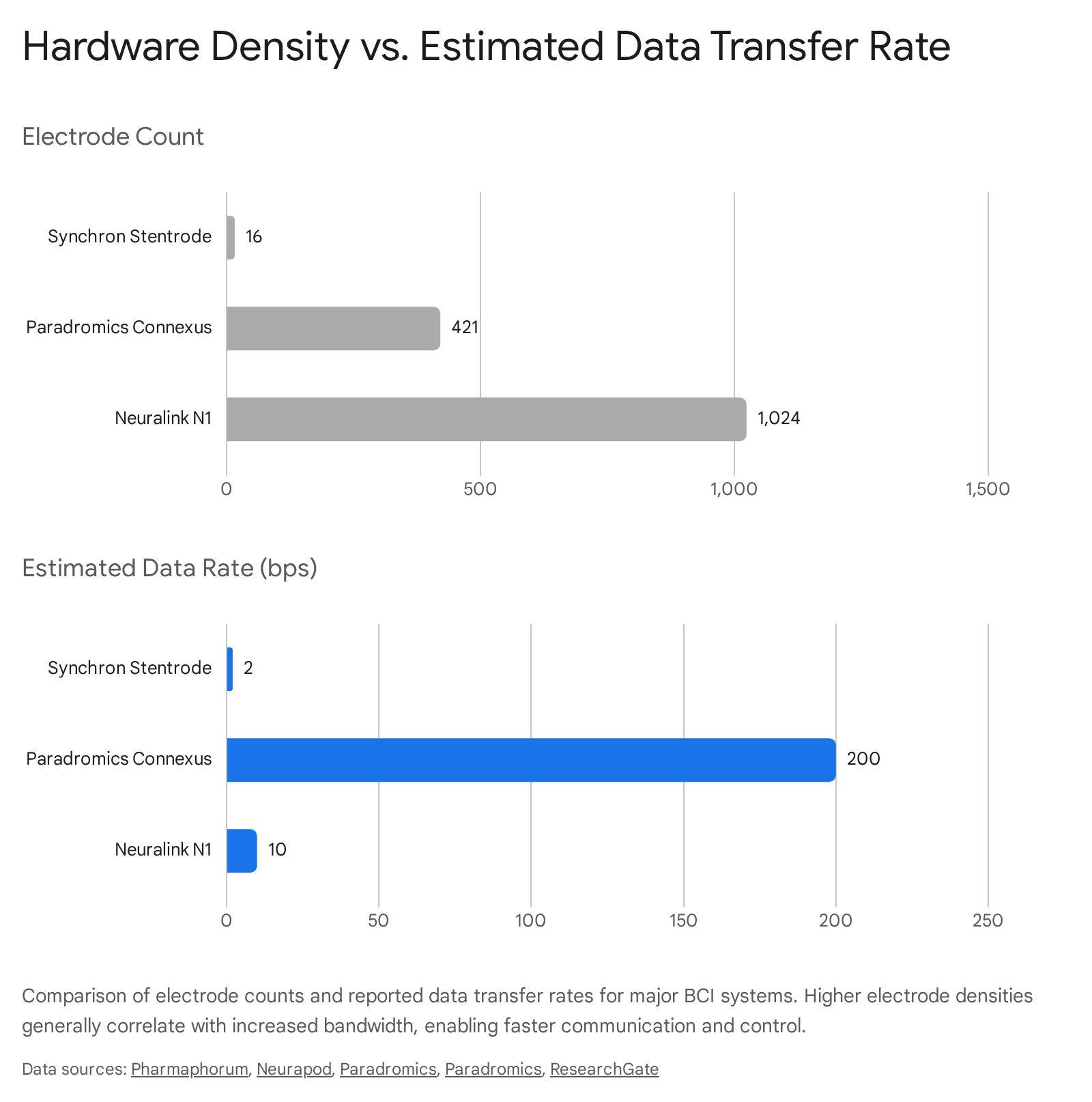
| Neuralink | Intracortical (Polymer Threads) | 1,024 | Robotic insertion (open craniotomy) | Human Trials (21+ patients) 4 |
| Paradromics | Intracortical (Platinum-Iridium) | 421 | Mechanical insertion (craniotomy) | First-in-Human Trials 24 |
| Precision Neuroscience | Epidural / Subdural (Thin-Film) | 1,024 | Micro-slit cranial insertion | FDA 510(k) Cleared (30-day use) 22 |
| Synchron | Endovascular (Nitinol Stent) | 16 | Transjugular catheter delivery | Pre-Pivotal Trial (COMMAND concluded) 523 |
| Neuracle / Tsinghua | Epidural (NEO System) | N/A | Minimally invasive burr hole | NMPA Commercially Approved 4 |
| Inbrain Neuroelectronics | Subdural (Graphene Interface) | Varies | Surgical placement | First-in-Human Cohort Completed 24 |
| Blackrock Neurotech | Intracortical (Utah Array / Neuralace) | 96 - 128 | Mechanical insertion (craniotomy) | Chronic human trials (MoveAgain) 125 |
Intracortical Innovators and High-Density Signal Decoding
The pursuit of single-unit recording drives the intracortical space, where the engineering focus has shifted toward maximizing electrode density while minimizing mechanical trauma. The ultimate objective is high-fidelity telemetry capable of decoding speech and restoring robotic autonomy at speeds mirroring able-bodied capability.
Neuralink N1 Architecture and Clinical Progress
Neuralink's N1 implant represents the most aggressive push toward high-bandwidth intracortical recording. The device employs 128 flexible polyimide threads, each containing 16 electrodes, for a total of 1,024 recording channels 1326. These threads, measuring 10 to 12 micrometers in diameter, are individually deployed into the motor cortex by the proprietary R1 surgical robot.
The rationale behind the R1 surgical robot is that the threads are too fine and flexible to be manipulated by human neurosurgeons. The robotic system uses advanced optical tracking to avoid cortical vasculature during insertion, theoretically reducing micro-hemorrhaging and the subsequent inflammatory response 26. The N1 device samples data at 20 kHz, capturing both extracellular action potentials and local field potentials, and transmits compressed data via secure Bluetooth to external devices 14. The internal battery is inductively recharged by an external unit, allowing the system to operate fully wirelessly without percutaneous connectors 2627.
By late 2025 and into 2026, Neuralink significantly expanded its PRIME (Precise Robotically Implanted Brain-Computer Interface) clinical study. After initial 2024 operations demonstrated reliable cursor control for gaming and digital interactions - achieving speeds of 7 to 10 bits per second - the company scaled its trial to 21 participants globally, including international expansion via the CAN-PRIME (Canada) and UAE-PRIME (United Arab Emirates) registries 4282930. As of late 2025, patients had logged over 15,000 hours of safe operation, providing petabytes of neural data used to optimize decoding algorithms 1314.
The clinical expansion was not without technical challenges. Early human trials revealed that normal brain pulsation within the cerebrospinal fluid caused some of the flexible polymer threads to retract from the cortical tissue, leading to a temporary loss of functional electrode channels 434. In response, Neuralink adjusted surgical protocols to insert threads deeper into the cortex - up to 8 millimeters 34. While this adjustment stabilized the signal, the long-term biological consequences of deeper thread penetration and potential tissue shear remain an active area of longitudinal monitoring. Following a $650 million Series E funding round, the company plans to move toward automated, high-volume production in late 2026, aiming to refine indications toward direct speech communication and assistive robotic limb control 4835.
Paradromics and Longevity Prioritization
Paradromics presents an alternative philosophy to high-density intracortical arrays. While Neuralink utilizes flexible polymer threads designed to move with the brain, Paradromics targets long-term durability using established medical-grade materials. Its Connexus BCI features 421 penetrating microwires made of platinum-iridium, backed by a hermetically sealed titanium alloy body 3036. This design choice is grounded in the historical failure rates of thin-film polymers in the harsh, corrosive, and fluid-filled environment of the human body. By utilizing materials commonly found in pacemakers and deep brain stimulators, Paradromics aims to ensure device viability extending into decades rather than years 36.
Paradromics prioritizes maximum data throughput specifically for speech restoration. In preclinical models, the Connexus system achieved information transfer rates exceeding 200 bits per second with negligible delay, leveraging a new benchmarking standard called SONIC 3631.
The system records at a spatial resolution sufficient to capture phoneme-level motor intent. Following FDA Investigational Device Exemption (IDE) approval in November 2025, Paradromics initiated the Connect-One Early Feasibility Study in Q1 2026, specifically enrolling patients with severe speech and motor impairments across major U.S. clinical sites, including Massachusetts General Hospital and the University of Michigan 2431.
Blackrock Neurotech and Legacy Infrastructure
Blackrock Neurotech remains a foundational pillar of the BCI industry. Founded in 2008, the company manufactures the 96-channel Utah Array, which has supplied the hardware for the vast majority of academic intracortical research over the past 15 years 1. Despite its tendency to elicit glial scarring over time, the array has been validated in over 2,000 published studies 2. In 2021, the FDA awarded Breakthrough Device Designation to Blackrock's MoveAgain system, aimed at transitioning their technology from lab environments to at-home patient use 125. Concurrently, Blackrock is developing a next-generation flexible lattice electrode known as Neuralace to mitigate the tissue damage associated with its legacy rigid spikes 15.
Endovascular Approaches and Scalability
Endovascular architectures compromise on raw signal bandwidth to prioritize surgical safety, targeting the large cohort of paralysis patients for whom open brain surgery presents an unacceptable risk.
Synchron Stentrode and the COMMAND Trial
Synchron is the definitive pioneer of endovascular BCI. Its flagship device, the Stentrode, consists of a self-expanding nitinol (nickel-titanium) stent embedded with 16 platinum-iridium recording electrodes 2132. A neurointerventionalist delivers the device transvenously via the internal jugular vein, navigating it into the superior sagittal sinus. Upon deployment, the stent expands, pressing the electrodes against the vessel wall adjacent to the primary motor cortex. The device is wired subcutaneously down the neck to an implantable receiver-transmitter unit (IRTU) placed in the chest, which wirelessly transmits data to external devices via Bluetooth 232732.
Because the Stentrode does not breach the brain parenchyma or the blood-brain barrier, it evades the aggressive microglial response that degrades penetrating arrays. Preclinical and human data show that the stent rapidly endothelializes - becoming fully incorporated into the blood vessel wall - which establishes a highly stable electrode-tissue interface without inhibiting venous blood flow 21.
In late 2024, Synchron concluded the 12-month evaluation phase of its COMMAND trial, a pivotal US-based feasibility study involving six patients with severe chronic bilateral upper-limb paralysis. The study successfully met its primary endpoint, demonstrating zero device-related serious adverse events, no neurological safety events, no vessel occlusions, and 100% deployment accuracy with a median deployment time of just 20 minutes 53340.
Signal analysis from the COMMAND trial confirmed the long-term viability of transvascular recording. Researchers analyzed electrocorticographic signals focusing on the low gamma (30 - 70 Hz) and high gamma (70 - 200 Hz) bands. The channel-averaged signal-to-noise ratio (SNR) and the effective signal bandwidth (averaging 233 Hz) remained consistent across the 12-month period with no significant channel dropout or baseline drift 2332. Users successfully generated Digital Motor Outputs (DMOs) - converting thought-derived intent into reliable digital commands, allowing patients to text, email, and browse the internet hand-free 52334. With technology development partnerships established with major firms like Apple and Nvidia, Synchron is currently utilizing patient registries to prepare for a broader pivotal trial, moving closer to commercial scalability 1523.
Surface Arrays and Novel Material Substrates
Occupying the middle ground between highly invasive penetrating arrays and lower-bandwidth endovascular devices, surface arrays utilize thin-film technologies and novel nanomaterials to record high-resolution cortical signals without piercing the brain tissue.
Precision Neuroscience and Minimally Invasive Mapping
Founded by former Neuralink researchers, Precision Neuroscience has developed the Layer 7 Cortical Interface. The device consists of a flexible microelectrode array containing 1,024 contacts printed on a polyimide film that is one-fifth the thickness of a human hair 152235. It is inserted through a sub-millimeter cranial slit and slides gently over the cortical surface, conforming to the brain's natural convolutions.
In April 2025, Precision Neuroscience achieved a critical regulatory milestone when the FDA granted 510(k) clearance for the Layer 7 interface for up to 30 days of temporary implantation 223637. The clinical data supporting this clearance involved 37 patients who received the temporary implant during procedures such as brain tumor resections 2235. While currently marketed for intraoperative brain mapping, the 30-day clearance allows the company to accumulate a vast repository of high-resolution neural data. Supported by a $104 million Series C funding round in late 2024, this dataset is being utilized to train decoding algorithms for their forthcoming permanent BCI platform targeted at chronic conditions like spinal cord injury and ALS 3638.
Inbrain Neuroelectronics and Graphene Interfaces
Material science is a major frontier in BCI research, primarily driven by the search for substrates that offer better biocompatibility and electrical conductivity than traditional metals. Spain-based Inbrain Neuroelectronics has pioneered the use of graphene - a single-layer carbon lattice - for neural interfaces. Graphene is exceptionally strong, flexible, and possesses superior charge injection capacity compared to platinum or iridium, allowing for smaller, more densely packed electrodes 4647.
In April 2026, Inbrain completed patient recruitment and surgical follow-ups for a first-in-human study involving eight patients undergoing brain tumor resections. The study utilized their 10-micrometer-thick graphene cortical interface 2446. Results demonstrated no perioperative device failures and no device-related adverse events over a 90-day post-operative period 72439. Clinical investigators confirmed that the graphene arrays captured neural signals - including language-associated gamma band activity during awake mapping surgeries - with exceptional fidelity, highlighting graphene's potential for high-definition decoding in next-generation BCI therapeutics 724. The company is also collaborating with Microsoft to explore agentic AI applications for patient monitoring, and with Merck KGaA for systemic bioelectronic therapies 4639.
The Wyss Center ABILITY Platform
The Wyss Center for Bio and Neuroengineering has advanced its fully implantable ABILITY system, utilizing subscalp Epios sensing electrodes. Aimed at patients who are completely locked-in, the system relies on intracortical microelectrode arrays connected to a subcutaneous transmitter that beams data wirelessly through the scalp 640. In a landmark clinical case study, the Wyss Center enabled a completely paralyzed patient with advanced ALS - who lacked any voluntary muscle control including eye movement - to communicate reliably via the BCI, proving that the motor cortex retains the ability to generate specific commands even after severe peripheral motor degradation 4142.
| Clinical Trial | Sponsor / Developer | Primary Pathology Target | Enrollment Status (2025/2026) | Key Milestone |
|---|---|---|---|---|
| PRIME Study | Neuralink | Quadriplegia, ALS, SCI | 21+ patients | 15,000+ hours of functional data collection 414. |
| COMMAND | Synchron | Severe Bilateral Paralysis | 6 patients | Met primary safety endpoint at 12 months 5. |
| Connect-One | Paradromics | Severe Motor/Speech Impairment | Actively enrolling | Achieved >200 bps data transfer rate 2431. |
| Layer 7 Mapping | Precision Neuroscience | Tumor Resection Mapping | 37 patients | FDA 510(k) clearance for 30-day use 22. |
| Empower BP | ONWARD Medical | Chronic SCI (Blood Pressure) | Actively enrolling | Global pivotal study initiated 43. |
| Graphene Interface | Inbrain Neuroelectronics | Tumor Resection Mapping | 8 patients | First-in-human cohort completed successfully 2447. |
Neuromodulation and Movement Restoration
While much of the BCI industry focuses on digital interaction and communication, restoring physical mobility remains a paramount objective. ONWARD Medical bridges the gap between BCI signal decoding and therapeutic neuromodulation through its ARC-BCI therapy. The system pairs a cortical BCI (specifically the WIMAGINE interface, originally developed by CEA-Clinatec) with the ARC-IM epidural spinal cord stimulator 54.
The BCI component, implanted epidurally over the motor cortex, decodes movement intent. It wirelessly transmits this data - forming a framework ONWARD terms the "DigitalBridge" - to the spinal implant. The spinal implant then delivers targeted electrical pulses to the spinal cord below the level of the injury, activating the paralyzed muscles in real-time . By January 2026, seven individuals with severe spinal cord injuries had been successfully implanted with the ARC-BCI system, restoring thought-driven movement to both upper and lower paralyzed limbs .
Simultaneously, ONWARD recognized that spinal cord injury disrupts autonomic nervous system functions. To address this, the company initiated the Empower BP global pivotal trial to evaluate the ARC-IM system's capacity to autonomously manage life-threatening blood pressure instability (hypotension) following SCI. Published results in Nature Medicine demonstrated that the system produced immediate and robust increases in blood pressure, greatly reducing hypotensive symptoms and enabling patients to tolerate upright rehabilitation postures 43.
The Chinese BCI Ecosystem and Commercial Approvals
The global regulatory landscape for BCIs saw a historic shift in early 2026. While U.S. and European regulators treat BCIs strictly as investigational devices progressing through IDE pathways and phased clinical trials, China's regulatory bodies aggressively accelerated commercial clearance to fulfill national industrial strategy.
Commercial Launch of the NEO System
In March 2026, the National Medical Products Administration (NMPA) formally approved the NEO (Neural Electronic Opportunity) BCI for commercial medical use, marking the world's first Class III market approval for an invasive BCI device 44445. Co-developed by Neuracle Technology and Tsinghua University, NEO is an epidural, wireless system designed for patients aged 18 to 60 with cervical spinal cord injuries who retain some arm mobility but cannot grip 446.
Unlike penetrating arrays, NEO's coin-sized processors rest on the dura mater above the sensorimotor cortex, prioritizing surgical safety and long-term tissue viability over single-neuron resolution 1718. The clinical data supporting NEO's approval was derived from 36 clinical procedures conducted across 11 top-tier medical institutions, including Huashan Hospital and Xuanwu Hospital 445.
The system decodes basic motor signals to operate a pneumatic robotic glove. Trial patients demonstrated a grasping accuracy rate exceeding 90%, enabling independent tasks such as holding a cup, drinking, or eating within one month of post-operative home rehabilitation 174445. Furthermore, clinical metrics recorded signs of neural remodeling and partial recovery of peripheral sensory-evoked potentials, suggesting the closed-loop feedback promotes active neurological rehabilitation 3417.
Regulatory Frameworks and Industrial Policy
The commercial launch of NEO is deeply intertwined with China's broader industrial policy and geopolitical posture. In April 2026, China's State Administration for Market Regulation issued a comprehensive batch of 18 national standards covering emerging technologies, explicitly codifying guidelines for BCI hardware, semiconductors, and intelligent connected vehicles 4761.
Industry analysts note a stark divergence in global AI and BCI governance frameworks. The European Union's AI Act relies on stringent risk-tiering and pre-market product safety constraints focused on fundamental rights, a regulatory approach that often slows market deployment 61. In contrast, China views BCI and agentic AI as foundational economic and social infrastructure. The Chinese state adopts a development-oriented, coordinated framework to rapidly push prototypes from the lab to scaled deployment, supported by massive state-backed industry funds 4461. Concurrently, new Chinese legislation on Industrial and Supply Chain Security increases regulatory oversight on multinational corporations, reflecting a strategic effort to insulate the domestic neurotechnology supply chain from foreign technological decoupling and geopolitical volatility 4849.
Fundamental Scientific Obstacles to Device Longevity
Beneath the commercial momentum and clinical successes, the long-term viability of BCI technology remains constrained by fundamental neurobiology. The human brain perceives penetrating electrodes as pathogenic invaders, triggering an aggressive and coordinated foreign body response (FBR) 1265.
The Biological Mechanism of the Foreign Body Response
The mechanical insertion of a rigid electrode into the soft parenchyma inherently causes localized micro-hemorrhaging and breaches the blood-brain barrier 12. This acute trauma immediately activates resident microglia, the central nervous system's primary immune cells. The microglia proliferate, migrate to the insertion site, and undergo a morphological transition to a reactive state. They secrete pro-inflammatory cytokines and reactive oxygen species that oxidize the electrode surface, ultimately corroding the implant and impeding electrical transmission 165051.
Concurrently, local astrocytes become hypertrophic and proliferate in a process known as reactive astrogliosis 1152. Driven by complex molecular cascades - including the upregulation of EphA4 receptors and the JAK/STAT3 signaling pathways - astrocytes interweave to form a dense physical barrier around the implant 115253. Crucially, these reactive astrocytes secrete extracellular matrix proteins, notably chondroitin sulphate proteoglycans (CSPGs). CSPGs actively inhibit axonal growth and prompt nearby neurons to retract from the injury site 5052.
The resulting structure, the glial scar, effectively isolates the electrode. Because the scar tissue acts as an electrical insulator and the target neurons have physically died back, the electrical signal-to-noise ratio degrades precipitously 121665. This neuroinflammatory cascade is the primary biological reason why legacy arrays lose substantial channel efficacy within 12 to 24 months of implantation.
Pharmacological and Material Mitigation Strategies
BCI longevity hinges on outmaneuvering the glial scar. Engineering strategies in 2026 focus heavily on material compliance and localized pharmacology:
- Mechanical Matching: Replacing rigid silicon with flexible polymers (such as polyimide) or ultra-thin nanomaterials (such as graphene) reduces the micromotion shear forces between the pulsing brain and the static electrode, significantly delaying the onset of chronic inflammation 124654.
- Pharmacological Elution: Systemic anti-inflammatory drugs are inadequate for localized brain scarring. Instead, researchers are integrating anti-inflammatory agents directly into the electrode coatings. Covalently binding dexamethasone (DEX, a potent synthetic glucocorticoid) to polyimide substrates (like BPDA-PDA) allows for sustained, localized drug release over many weeks 5556. In vitro and in vivo models demonstrate that DEX-eluting electrodes significantly reduce macrophage activation, downregulate pro-inflammatory markers, and minimize the thickness of the fibrotic capsule, resulting in substantially lower and more stable electrical impedance profiles 5657.
Battery Longevity and Power Management
Beyond biological rejection, power delivery remains a critical limiting factor for implant longevity. Modern high-density BCIs process massive amounts of data on-chip, requiring substantial power. While endovascular systems like the Stentrode transfer power wirelessly via near-field RF to an infraclavicular unit, fully cranial implants rely on small inductive batteries 2627.
Battery chemistry limits the number of recharge cycles an implant can undergo before capacity degrades. In 2026, advances in "smart pausing" algorithms and gallium nitride (GaN) charging technology - which optimize charge curves and manage thermal limits to prevent tissue heating - have extended battery lifespans 58. Nonetheless, if a cranial BCI battery degrades after five to seven years, the patient requires a surgical revision, underscoring the need for ultra-low-power telemetry protocols.
Neuroengineering Realities Versus Public Perception
As BCIs enter the commercial sphere, a pronounced gap exists between clinical neuroengineering capabilities and public expectations of "mind reading" or cognitive uploading. The prevailing media narrative often conflates decoding specific motor cortex commands with accessing higher-order semantic thought, memory, or intelligence 97559.
Motor Intent Versus Inner Thought
Modern BCIs do not "read thoughts." They intercept electrical commands intended for muscles. When a paralyzed patient uses a BCI to type, they are typically imagining the physical movement of a hand moving a joystick or a finger pressing a key. The BCI decodes the spatial and temporal firing patterns in the motor cortex associated with that specific physical intent and translates it to a digital cursor 10.
Even in advanced speech decoding - where researchers can decode attempted phonemes at high speeds - the system is monitoring the motor cortex's instructions to the larynx, tongue, jaw, and lips 31. A pivotal 2025 study by Kunz et al. at Stanford and UCSF highlighted that while the representation of internal speech (silent dialogue) correlates highly with attempted speech in the motor cortex, the neural signals contain a distinct "motor-intent" dimension that differentiates the two 60.
To protect privacy and prevent a speech BCI from constantly broadcasting a user's private internal monologue, engineers utilize keyword triggers. The BCI algorithm is trained to ignore baseline neural chatter and only begin decoding speech when the user explicitly thinks of a specific "password" or visualizes a specific initiation movement 60. This proves that the devices require active, conscious user cooperation and cannot secretly extract private thoughts.
The Technical Impossibility of Data Uploading
Furthermore, the physical architecture of neural circuitry renders the concept of "uploading" or "downloading" memories functionally impossible with current physics 910. Memories, knowledge, and intelligence are not stored as binary data in localized sectors; they are encoded in the distributed, dynamic synaptic weights of billions of interconnected neurons across multiple brain regions.
Current BCIs, even high-density arrays with 1,024 channels, sample less than a fraction of a percent of the brain's 86 billion neurons. Translating external digital code into a biological format that the central nervous system could integrate into localized semantic memory remains science fiction 975. The near-term reality of BCI is entirely focused on outputting motor commands and providing highly localized sensory feedback, not writing complex cognitive information into the cortex.
Conclusion
The state of brain-computer interfaces in 2026 reflects a sophisticated, rapidly commercializing medical technology sector. The field has bifurcated into distinct strategies: deep intracortical arrays (Neuralink, Paradromics) pushing the limits of bandwidth for rapid speech and complex robotics, and less invasive surface or endovascular systems (Precision Neuroscience, Synchron, Tsinghua NEO) offering stable, lower-risk solutions for functional independence and communication.
The approval of the NEO system in China demonstrates that the regulatory and industrial frameworks required to deliver these devices to patients are now active and scaling rapidly 4. However, the ceiling of BCI capability remains firmly capped by biological constraints. Until materials science fully circumvents the brain's foreign body response through pharmacological elution and nanomaterial design, and until electrode integration becomes seamless over decades, BCI will remain a specialized neuro-prosthetic tool rather than a ubiquitous consumer enhancement. As clinical data scales over the next five years, the industry focus will increasingly shift from raw signal acquisition to algorithmic and material longevity, ensuring that the digital bridges built today remain stable for the lifetime of the patient.