How to Build Better Sleep Habits According to Science
Building better sleep habits requires aligning daily behaviors with the body's internal biological clock and its homeostatic drive for rest. Science indicates that optimal sleep is achieved by anchoring circadian rhythms with morning sunlight, establishing a cool sleeping environment, avoiding late-day caffeine and alcohol, and reclaiming daytime autonomy to prevent psychological bedtime procrastination. By treating sleep as a 24-hour biological process rather than a switch flipped at night, individuals can achieve lasting, restorative rest.
The Dual-Process Model of Sleep Regulation
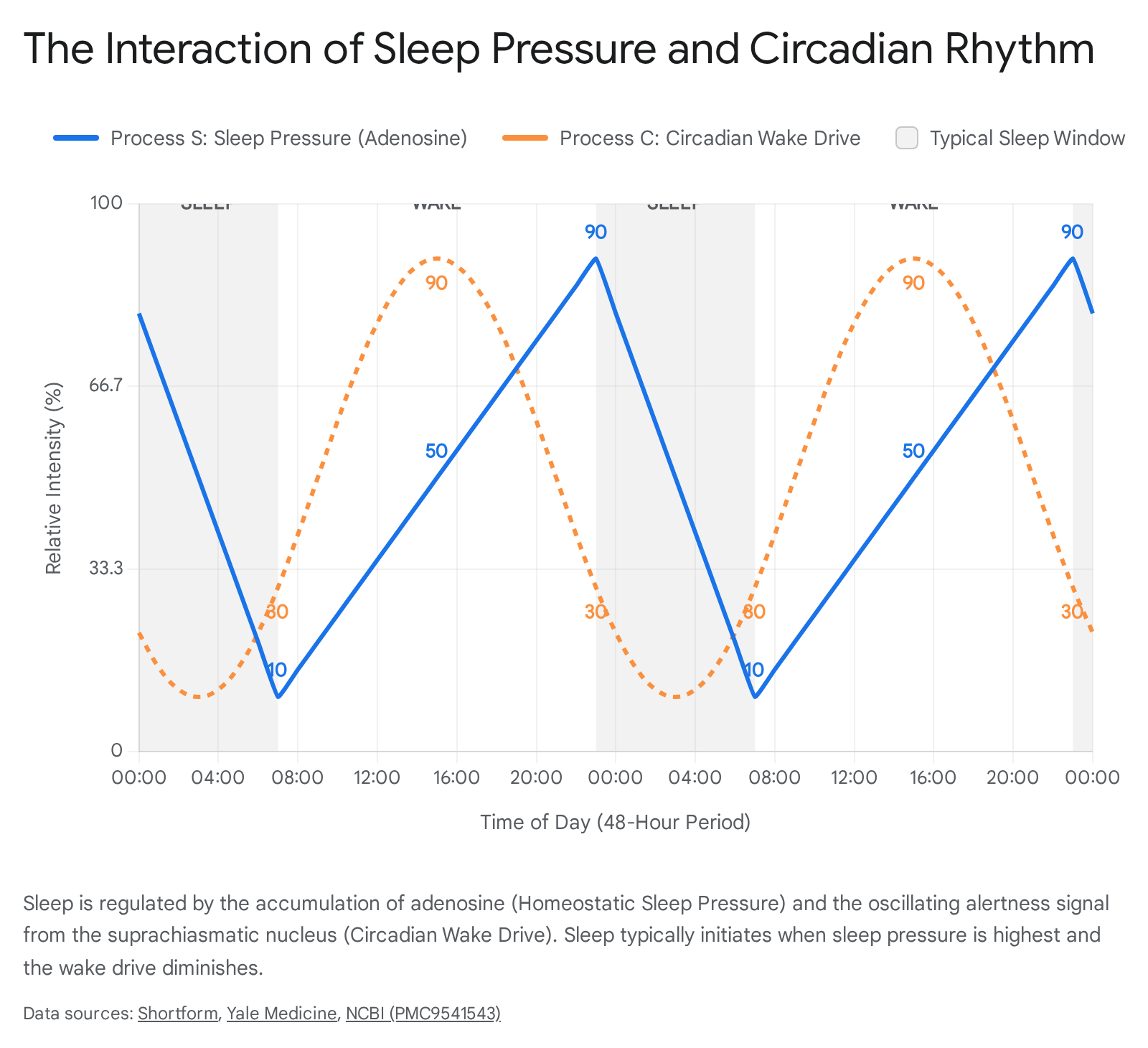
For decades, sleep scientists and neurobiologists have understood that human sleep is not merely a passive state of rest, but rather the result of a delicate, dynamic interplay between two distinct biological mechanisms. This framework, widely known in chronobiology as the two-process model of sleep regulation, involves Process S (the homeostatic sleep drive) and Process C (the circadian rhythm) 123. Understanding how these two systems operate independently - and how they ultimately converge - is the absolute foundational step in diagnosing poor sleep and building better, evidence-based habits.
Process S: The Adenosine Hourglass
Process S represents the body's homeostatic demand for sleep, which builds up progressively the longer an individual remains awake. The primary biochemical currency by which the brain measures this accumulated "sleep debt" is a neuromodulator called adenosine 234. Adenosine is a natural byproduct of cellular metabolism and the breakdown of adenosine triphosphate (ATP), the body's core energy molecule. From the moment a person wakes up and begins expending energy, adenosine steadily accumulates in the extracellular spaces of the brain, particularly in the basal forebrain 23.
As these extracellular adenosine levels rise, the molecule binds to specific inhibitory receptors - primarily the A1 and A2A receptors located in the brain's striatum and nucleus accumbens 35. This binding action creates a cascade of neurochemical events. It gradually inhibits the brain's wake-promoting regions while simultaneously stimulating sleep-promoting centers in the hypothalamus 34. The subjective experience of this biological process is what we call "sleep pressure," an overwhelming sensation of fatigue and cognitive heaviness that makes staying awake increasingly difficult.
When an individual finally succumbs to this pressure and falls asleep, the brain begins the critical work of clearing this accumulated adenosine. During restful, slow-wave sleep (often referred to as deep sleep), the brain's glymphatic system flushes out metabolic waste, and adenosine levels plummet, effectively resetting the hourglass for the following day 234. If a sleep opportunity is cut short, the adenosine is not fully cleared. This leaves a residual sleep debt that carries over into the following morning, manifesting as severe grogginess, impaired cognitive function, and a heightened vulnerability to stress 126.
Process C: The Master Internal Clock
While Process S builds on a linear trajectory throughout the waking hours, Process C operates on a cyclical, approximately 24-hour rhythm. The circadian rhythm is controlled by a tiny but immensely powerful region in the brain called the suprachiasmatic nucleus (SCN) 177. Consisting of roughly 20,000 neurons located in the hypothalamus just above the optic chiasm, the SCN acts as the body's master biological clock 78. It coordinates the timing of hormone release, core body temperature fluctuations, and metabolic processes across the entire body 178.
The master clock does not operate alone; it relies on a hierarchical system. The SCN coordinates countless "peripheral clocks" located in organs such as the liver, heart, kidneys, and even skeletal muscle 78. For example, in the morning, the SCN releases a surge of cortisol to mobilize energy, which signals the liver to adjust its own localized circadian rhythm to optimize glucose metabolism for the waking day 79. On a cellular level, these clocks are governed by specific clock genes (such as BMAL1, CLOCK, PER, and CRY) and energy-sensing proteins like AMPK and SIRT1, which link metabolic health directly to circadian timing 17.
Crucially, Process C sends a powerful alerting signal to the brain that counteracts the growing sleep pressure of Process S during the daytime hours 4. This circadian wake drive typically peaks in the late afternoon or early evening. This biological mechanism explains the common phenomenon of why individuals rarely fall asleep at 6:00 PM despite having accumulated a significant amount of adenosine since the early morning 4. As night falls, the SCN reduces its alerting signal and communicates with the pineal gland to release melatonin, the darkness hormone that chemically signals to the body that it is time to transition into a state of sleep 277.
Manipulating the Sleep Drive: The Complex Role of Caffeine
Because the homeostatic sleep drive is entirely dependent on the accumulation of adenosine, blocking this molecule is the primary biological mechanism by which humans artificially delay sleep and enhance daytime alertness. Caffeine is the most widely consumed psychoactive substance in the world, and it functions primarily as a direct adenosine receptor antagonist 25. The molecular structure of caffeine is remarkably similar to that of adenosine. This structural similarity allows caffeine molecules to bind to the A1 and A2A receptors in the brain without actually activating them 35. By occupying these receptor sites, caffeine effectively blocks the true adenosine from locking in, tricking the brain into perceiving an absence of sleep pressure and thereby promoting extended wakefulness 2.
Genetic Variability and Caffeine Metabolism
However, the efficacy, duration, and subsequent sleep disruption caused by caffeine are highly variable from person to person. Caffeine has a highly variable half-life ranging from 2 to 10 hours, heavily dependent on a myriad of endogenous factors (like genetics) and exogenous factors (such as nicotine use, which can accelerate caffeine metabolism by up to 50%) 10.
An individual's genetic makeup heavily dictates their baseline metabolic rate for caffeine. Certain individuals possess specific variations in liver enzymes that metabolize caffeine incredibly fast. For these "fast metabolizers," caffeine consumed in the late afternoon may be cleared rapidly enough to have negligible effects on their nighttime sleep architecture 1112. Conversely, for "slow metabolizers," a single cup of coffee consumed at noon can leave enough residual caffeine in the central nervous system to attenuate markers of deep sleep and shift brain oscillations toward wakefulness well past midnight 11.
Recent large-scale Mendelian randomization studies utilizing genetic data from hundreds of thousands of participants in the U.K. Biobank have provided a more nuanced perspective on caffeine's role in sleep disruption. These studies sought to separate the chemical effects of caffeine from the lifestyle behaviors of coffee drinkers. The data revealed that individuals genetically predisposed to fast caffeine metabolism successfully utilize the drug to reduce daytime napping and morning grogginess 1213. Surprisingly, these fast metabolizers do not suffer from higher causal rates of clinical insomnia or reduced total sleep duration compared to non-drinkers 1214. The researchers concluded that the severe sleep disruption often observationally blamed on coffee might actually be driven by different, overlapping lifestyle habits shared among heavy drinkers - such as high stress, poor diet, or lack of exercise - rather than the caffeine itself 12.
The Adaptation of Adenosine Receptors
Despite these genetic nuances, habitual caffeine use poses a structural challenge for long-term sleep hygiene. The brain is highly adaptive; it responds to chronic caffeine antagonism by upregulating the production of adenosine receptors 2. With more receptors available over time, the brain requires escalating doses of caffeine to block enough sites to achieve the same level of perceived alertness 210.
When a habitual user attempts to sleep, this increased density of receptors means that even minor amounts of residual adenosine can cause significant sleep pressure. Conversely, during waking hours, if caffeine is withheld, the overabundance of open receptors is flooded by baseline adenosine, resulting in profound withdrawal fatigue 2. To sustain the wake-promoting effects of caffeine without destroying nocturnal sleep quality, sleep medicine professionals recommend taking intermittent breaks from caffeine consumption. These designated "washout" periods allow the brain to downregulate adenosine receptors, resetting the individual's natural sensitivity to sleep pressure 210.
Synchronizing the Master Clock: Light as a Zeitgeber
While manipulating adenosine manages the homeostatic sleep pressure, carefully managing light exposure is the primary method for synchronizing the circadian rhythm. The SCN does not inherently know what time it is in the external world. It relies entirely on external environmental cues, known in chronobiology as zeitgebers (a German term translating to "time givers"), to align internal physiology with the 24-hour rotation of the Earth 789. Light is overwhelmingly the most powerful zeitgeber available to human biology 77.
The Anatomy of Light Detection
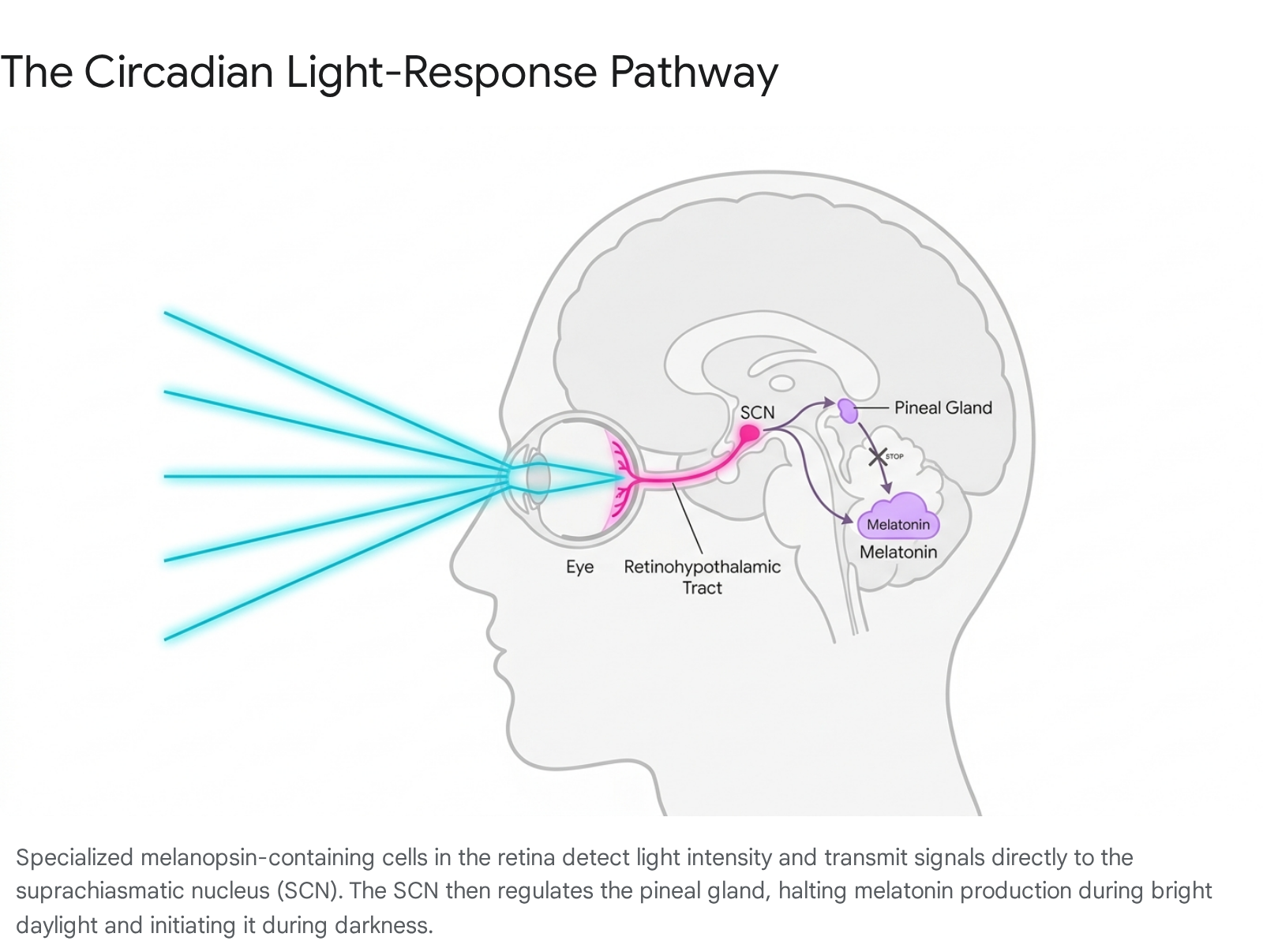
The process of circadian synchronization begins in the eye, but it utilizes a completely different pathway than visual sight. The retina contains a small subset of specialized ganglion cells equipped with a unique photopigment called melanopsin. These cells, known as intrinsically photosensitive retinal ganglion cells (ipRGCs), do not form visual images 715. Instead, they act strictly as biological light meters, constantly measuring the intensity and spectral composition of ambient light in the environment 7.
When these ipRGCs detect sufficient light, they transmit electrochemical signals directly to the SCN via a dedicated neural superhighway known as the retinohypothalamic tract 7. This direct line of communication bypasses the visual cortex entirely. Once the SCN receives this daylight signal, it halts the pineal gland's production of melatonin and orchestrates the release of daytime hormones to optimize alertness 7715.
Morning Light and the Phase Response Curve
The precise timing of light exposure dictates whether the circadian clock is shifted forward or backward. This bidirectional relationship is governed by a well-documented physiological model known as the human phase response curve 91617. Exposure to light in the late afternoon through the first part of the night induces a phase delay, pushing the internal clock later. Conversely, exposure to light in the early morning produces a phase advance, shifting the biological clock earlier so that an individual feels naturally sleepy earlier in the evening and wakes up earlier the following day 71617.
To effectively utilize light as an intervention for circadian synchronization or delayed sleep phase issues, both the intensity and the duration of the light must meet specific thresholds. Clinical protocols consistently recommend exposure to 2,500 to 10,000 lux of broad-spectrum white light for a duration of 30 to 120 minutes, ideally administered immediately upon awakening or within the first hour of the day 161718.
The efficacy of this morning light anchoring is profound. A recent 70-day daily diary study examining adult sleep patterns confirmed that every 30-minute increment of morning sun exposure (specifically before 10:00 AM) was associated with a 23-minute reduction in the midpoint of sleep, drawing the entire circadian rhythm earlier and improving overall sleep quality 1920. Interestingly, clinical research highlights that increasing the duration of morning light exposure may actually be more effective at shifting the human circadian clock than merely increasing the intensity of the light 17.
The Blue Light Debate and the mDFD Standard
While morning light is an essential anchor, light exposure in the evening is a potent circadian disruptor. The ipRGCs in the retina are most exquisitely sensitive to short-wavelength visible light, specifically in the blue spectrum spanning 460 to 480 nanometers 2122. When the eyes are exposed to this blue light in the evening, the brain interprets the signal as ongoing daylight. The SCN actively suppresses the pineal gland's secretion of melatonin, delaying sleep onset and disrupting the transition to rest 1522. The proliferation of LED lighting and digital screens has drastically increased human exposure to artificial blue light, leading to a widespread delay in circadian phases 2324.
However, the scientific narrative surrounding blue light is often distorted by commercial marketing. A pervasive myth asserts that blue light from digital devices causes permanent retinal damage or accelerates age-related macular degeneration. Comprehensive reviews by the American Academy of Ophthalmology have concluded that there is no clinical evidence to support this claim; the intensity of blue light emitted by consumer electronics is drastically lower than the blue light present in natural daytime sunlight 24. The true hazard of evening screen time is not ocular damage, but strict circadian disruption. A recent meta-analysis demonstrated that exposure to blue light in the two hours before bedtime delays sleep onset by an average of 22 minutes and truncates total sleep duration 24.
To combat this disruption, a massive industry of "blue light blocking" glasses has emerged. Yet, systematic reviews of randomized controlled trials historically showed inconsistent results regarding their efficacy 21. The core issue was a lack of standardization in lens quality. In recent years, researchers introduced a measurable metric known as the melanopic daylight filtering density (mDFD) to quantify a filter's actual capacity to reduce the specific ipRGC stimulation that drives melatonin suppression 22.
Studies published in Translational Vision Science & Technology establish that only lenses achieving an mDFD of 1.0 or higher - typically dark orange or heavy amber-tinted lenses - produce a clinically meaningful circadian benefit under standard indoor lighting 22. Clear or lightly tinted lenses, frequently bundled with electronics or sold as cheap anti-fatigue wear, generally achieve mDFD values below 0.5. While these clear lenses may reduce digital eye strain, they are biologically useless for preserving evening melatonin 2224. For effective sleep hygiene, individuals are advised to implement a "digital sundown," engaging in "virtual darkness" using high-mDFD filters or relying on software night-modes to dramatically dim and warm ambient lighting at least 90 to 120 minutes before attempting to sleep 1522.
The Thermodynamics of Slow-Wave Sleep
Once the psychological and circadian hurdles are managed, the physical environment of the bedroom plays a decisive role in dictating the depth, continuity, and efficiency of sleep. Sleep efficiency - defined as the percentage of time spent actively asleep while in bed - is highly sensitive to ambient temperature.
Human core body temperature does not remain static; it operates on a precise circadian curve. About two hours before habitual bedtime, the body begins a natural cooling process, dropping its core temperature by a fraction of a degree. This physiological temperature drop is an essential biological prerequisite for sleep onset 25. Furthermore, the body must continue to shed heat effectively to enter and maintain slow-wave sleep (SWS), the deepest and most restorative phase of sleep responsible for cellular repair, immune system bolstering, and memory consolidation 25.
If a bedroom environment is too warm, the body struggles to complete this vital thermoregulation. The inability to shed heat forces the cardiovascular system to work harder, disrupting the natural cooling cycle and pulling the sleeper out of deep rest 2526. A large-scale longitudinal study utilizing environmental sensors and wearable monitors demonstrated that ambient temperature is a powerful, independent predictor of sleep quality across various demographics 2728.
For the general adult population, sleep science suggests an ideal bedroom temperature falls between 60°F and 67°F (15°C to 19°C), though individual comfort levels vary slightly 25. When ambient temperatures exceed these optimal ranges, the physiological consequences are immediate. Overheating leads to increased wakefulness, significantly reduced slow-wave sleep, and frequent nighttime awakenings 2526.
Interestingly, thermal needs appear to shift with age. Recent analyses focusing specifically on community-dwelling older adults revealed that their optimal environmental temperature range may be slightly higher than the general population, with maximum sleep efficiency observed between 68°F and 77°F (20°C to 25°C) 2728. However, regardless of the individual's baseline, extreme deviations remain highly detrimental. When ambient nighttime temperatures rose from 77°F to 86°F (25°C to 30°C), older adults experienced a clinically significant 5% to 10% drop in sleep efficiency 2728. In practical terms, this level of sleep fragmentation is severe enough to impair next-day cognitive performance, mood, and even postprandial glucose regulation 27.
How Alcohol Dismantles Sleep Architecture
Aside from temperature, the most pervasive environmental disruptor of sleep efficiency is alcohol. Alcohol is frequently, yet misguidedly, utilized by the general public as an over-the-counter sleep aid to self-medicate for stress or insomnia. Because alcohol acts as a central nervous system depressant, it reliably reduces sleep onset latency - meaning it does, in fact, help people fall asleep faster by promoting muscular relaxation and rapid sedation 293031.
However, falling asleep is not the same as obtaining restorative sleep. Systematic reviews and meta-analyses analyzing polysomnography data published over the last decade overwhelmingly confirm that alcohol fundamentally destroys the architecture of nocturnal sleep 293031. The disruptions follow a highly specific, biphasic chronological pattern throughout the night:
- The First Half of the Night: Shortly after consumption, high doses of alcohol prematurely accelerate the onset of deep sleep (N3). While this may sound beneficial, it comes at a severe cost. During this early phase, alcohol drastically suppresses Rapid Eye Movement (REM) sleep 29313332. REM sleep is the cognitive workhorse of the night, essential for emotional regulation, complex problem solving, and long-term memory consolidation. Delaying and truncating this stage compromises daytime mental acuity 3132.
- The Second Half of the Night: As the liver works continuously to metabolize the ethanol, the initial sedative effects begin to wear off. The body processes the alcohol into toxic byproducts like acetaldehyde and acetate. The clearance of these chemicals triggers a physiological "rebound effect" characterized by sympathetic nervous system activation, elevated nocturnal heart rate, and increased body temperature 303132. This physiological stress results in profound sleep fragmentation. The sleeper experiences frequent, prolonged awakenings (Wake After Sleep Onset, or WASO), night sweats, and vivid, often stressful dreams as the brain attempts to cram in the REM sleep it missed earlier in the night 303332.
Furthermore, because alcohol acts as a potent muscle relaxant, it slackens the tissues of the upper airway. This significantly increases the risk of snoring and exacerbates sleep-disordered breathing events, such as obstructive sleep apnea, which further shatters sleep continuity by forcing the brain to awaken slightly to resume breathing 303132.
The scientific consensus is unequivocal: alcohol, including red wine despite its trace amounts of antioxidants, should never be utilized as a sleep aid 3031. Because alcohol is metabolized at a relatively fixed rate of roughly 0.01% to 0.02% blood alcohol concentration per hour, implementing a strict cutoff of alcohol consumption several hours before bed is vital to allow the body to clear the ethanol before sleep initiates, thereby preserving essential REM architecture 32.
Comparing Primary Sleep Disruptors
| Environmental Disruptor | Impact on Sleep Onset | Impact on Sleep Architecture | Primary Mechanism of Biological Disruption |
|---|---|---|---|
| High Ambient Temperature (>77°F/25°C) | Increases time taken to fall asleep as the body struggles to shed heat. | Reduces deep slow-wave sleep (SWS); increases night awakenings. | Prevents the necessary nocturnal drop in core body temperature. |
| Evening Blue Light (Unfiltered screens) | Significantly delays sleep onset (average delay of 22 mins). | Delays the timing of all sleep stages; truncates total sleep duration. | Suppresses endogenous melatonin secretion via SCN neural signaling. |
| Late Evening Alcohol (Moderate to High Dose) | Decreases sleep onset latency (creates a rapid sedative effect). | Suppresses REM sleep early; causes severe fragmentation late in the night. | Sympathetic rebound during ethanol metabolism; upper airway muscle relaxation. |
The Psychology of Sleep: Stress and Revenge Bedtime Procrastination
Even when individuals possess a flawless understanding of circadian biology, caffeine half-lives, and ambient temperature, many still find themselves chronically sleep-deprived. The modern crisis of insufficient sleep is not merely a biological failure, but a deeply psychological and sociological issue. Modern societal structures - characterized by constant digital connectivity, hybrid work models blurring the line between office and home, and high-stress professional environments - have fostered a lifestyle that actively overrides biological sleep needs 233334.
A prominent behavioral phenomenon undermining adult sleep health is "revenge bedtime procrastination." Originally coined as the Chinese internet expression bàofùxìng áoyè (retaliatory staying up late), the term describes the deliberate decision to sacrifice necessary sleep for leisure time, despite a clear awareness of the negative health consequences and an absence of external circumstances forcing the individual to stay awake 353637.
Autonomy Deprivation and the "Silent Protest"
Clinical psychological research indicates that revenge bedtime procrastination is not primarily a failure of general self-regulation, laziness, or poor sleep hygiene knowledge. Rather, it is deeply rooted in a profound loss of daytime autonomy 363738. When an individual's day is entirely consumed by externally controlled obligations - such as demanding supervisors, back-to-back meetings, and unrelenting family care duties - they reach the evening feeling as though they have had zero agency over their own existence.
Consequently, the late-night hours become the only available window to reclaim a sense of self-determination and personal freedom 363839. The exhausted individual engages in a "silent protest" against their own schedule, aggressively binge-watching media, scrolling through social media, or shopping online to secure instant dopamine hits that provide temporary relief from the cognitive depletion of the day 363840. A 2021 study demonstrated that people whose days were filled with highly restricted, externally controlled obligations were significantly more likely to delay sleep for this "revenge" leisure 37.
Behavioral Solutions: Micro-Autonomy and MCII
This psychological behavior highlights a critical flaw in traditional sleep advice: simply instructing a stressed, burnt-out worker to put their phone away at 10:00 PM is largely ineffective if they feel they have had zero personal time during the preceding 16 hours. The solution requires restructuring the waking day, not just the bedtime routine 3637.
Psychological interventions grounded in Self-Determination Theory suggest that introducing "micro-autonomy" - small, fiercely protected windows of unstructured, non-optimized time during the daytime - can alleviate the psychological need to retaliate against the schedule at midnight 3739.
Additionally, therapeutic frameworks like Mental Contrasting with Implementation Intentions (MCII) have proven effective 36. In this strategy, an individual visualizes the positive outcome of going to sleep on time (e.g., "I will have high energy for my presentation tomorrow") and immediately contrasts it with the specific internal obstacle triggering the procrastination (e.g., "I feel the need to scroll on my phone because I am stressed"). By identifying the exact emotional trigger, the individual can create actionable "if-then" plans to detour the behavior, gradually unwinding the habit of trading restorative rest for empty digital stimulation 36.
Beyond Eight Hours: Genetics, Chronotypes, and Individual Needs
A persistent myth in popular culture is the rigid expectation that every healthy adult must sleep precisely eight hours, ideally between the hours of 11:00 PM and 7:00 AM. Sleep science has thoroughly dismantled this one-size-fits-all approach, revealing that sleep requirements are highly individualized and deeply tied to human genetics.
The American Academy of Sleep Medicine (AASM) consensus guidelines recommend that adults obtain between 7 and 9 hours of sleep per night to maintain optimal metabolic, cognitive, and cardiovascular health, while teenagers require 8 to 10 hours, and infants require up to 16 hours 41. However, adult sleep duration is a quantitative trait that follows a natural bell-curve distribution across the population 42.
Massive genome-wide association studies (GWAS), such as those analyzing genetic data from over 446,000 participants in the U.K. Biobank, have identified at least 78 specific genetic regions associated with how long an individual naturally sleeps 43. Some individuals possess specific, inherited gene mutations that render them "natural short sleepers." These rare individuals can function flawlessly on just 4 to 6.5 hours of sleep per night without exhibiting any of the adverse cognitive, metabolic, or cardiovascular health consequences typically associated with sleep deprivation 42. Conversely, genetic long-sleepers may genuinely require 9 to 10 hours of rest to achieve baseline cognitive functioning 4243.
Expanding the Chronotype Spectrum
Equally important to the duration of sleep is the preferred timing of sleep, governed by an individual's chronotype. Chronotypes represent a natural, genetic inclination for peak wakefulness and sleep at specific times of the 24-hour cycle 4344. Research indicates that chronotype has a strong inherited component, influenced heavily by variations in circadian clock genes, such as the PER3 allele 44. Evolutionary biologists postulate that varying chronotypes within early human tribes provided a survival advantage; by having staggered sleep schedules, there was always someone awake to keep watch against nocturnal predators 44.
Historically, science roughly divided the population into "morning larks" and "night owls." However, high-resolution behavioral research utilizing modern clustering algorithms has revealed that the human population actually encompasses a broader spectrum of at least five distinct biological sleep subtypes 45. These range from highly advanced early risers to extremely delayed late sleepers. Crucially, these subtypes showcase distinctly different cognitive and health risk profiles. For example, specific groups of night owls demonstrate superior performance on cognitive tests but struggle disproportionately with emotional regulation and elevated risks of cardiovascular issues, likely due to chronic misalignment with societal schedules 45.
Forcing a genetically wired night owl to adhere to a traditional 7:00 AM corporate wake time results in a state of chronic circadian misalignment, akin to permanent jet lag. They may successfully wake up to an alarm, but their underlying biology remains anchored in a sleep state, rendering them cognitively impaired and metabolically sluggish for hours 44. Sleep medicine increasingly advocates for flexible, personalized work schedules that accommodate these biological realities rather than punishing individuals for their genetic baseline 4245.
Cultural Contexts: Reevaluating "Normal" Sleep
When examining sleep habits, it is vital to separate rigid biological requirements from flexible cultural constructs. Many practices viewed as sleep disorders or poor hygiene in Western medicine are actually functional, deeply ingrained cultural norms in other parts of the world.
The Monophasic Standard vs. Biphasic History
Modern industrialized society largely insists on monophasic sleep - a single, continuous 8-hour block of rest during the night 46. However, historical texts and sociological research suggest that human beings naturally engaged in biphasic sleep (two distinct sleep episodes per 24 hours, often separated by a period of quiet wakefulness in the middle of the night) prior to the widespread advent of artificial indoor lighting and the structured schedules of the Industrial Revolution 46. Today, biphasic sleep schedules (such as relying on a core nighttime sleep supplemented by a strategic daytime nap) are being actively studied as a protective strategy for shift workers and medical professionals attempting to mitigate the severe cognitive penalties of abbreviated monophasic sleep windows 4647.
Co-Sleeping, Independence, and Health Outcomes
The pediatric sleep model utilized predominantly in the United States places a heavy premium on infant independence, strongly advocating for solitary sleep. The American Academy of Pediatrics currently recommends room-sharing (placing the infant's crib in the parents' room) but strictly opposes bed-sharing to prevent sleep-related infant fatalities, such as Sudden Infant Death Syndrome (SIDS) or accidental suffocation 504849. The underlying cultural philosophy frames an infant's success in sleeping alone in a separate room as a developmental milestone of autonomy and "independence training" 48.
However, cross-cultural studies reveal that solitary infant sleep is a distinctly Western cultural phenomenon, rather than a universal biological mandate 4849. In many Asian, African, and Latin American societies, co-sleeping (specifically bed-sharing) is the undisputed norm, reflecting deep-seated cultural values of familial interdependence, communal living, and emotional bonding 505350.
In Japan, where the practice of kawa no ji (sleeping in close physical proximity, visualized as the child acting as the central line in the river character between the parents) is pervasive, rates of SIDS are paradoxically among the lowest in the world 504953. Longitudinal studies show that Japanese mothers routinely co-sleep with their children into the teenage years without adverse psychological outcomes 50. This data suggests that the safety outcomes of co-sleeping are heavily dependent on how the practice is executed - such as the firmness of the mattress, the absence of heavy Western-style bedding, and the strict avoidance of parental alcohol or sedative use - rather than the fundamental act of bed-sharing itself 5049.
Cross-Cultural Sleep Practices Compared
| Region / Culture | Primary Sleep Arrangement Norm | Cultural Value Emphasized | Associated Health & Sociological Outcomes |
|---|---|---|---|
| United States & Western Europe | Solitary sleep (infant placed in a separate crib/room). | Independence, self-soothing, and early autonomy. | Higher rates of formalized sleep training methods; societal stigmatization of bed-sharing. |
| Japan | Pervasive co-sleeping (kawa no ji), often extending into childhood. | Interdependence, emotional closeness, and security. | Paradoxically lower rates of SIDS compared to Western nations; robust parental bonding. |
| Global South (Various Regions) | Room-sharing and bed-sharing integrated with extended family. | Resource efficiency, continual maternal physical contact. | Facilitates prolonged and responsive breastfeeding; sleep is viewed as a communal event. |
Clinical Recommendations and Sleep Hygiene Efficacy
To bridge the gap between complex biological mechanisms and daily behavioral application, clinical sleep medicine relies heavily on sleep hygiene protocols. However, the medical community is careful to calibrate the expectations of these interventions.
Systematic reviews and meta-analyses comprising thousands of patients indicate that while sleep hygiene education is highly beneficial for the general public, it is often insufficient as a standalone, single-therapy treatment for chronic clinical insomnia 5152. For patients suffering from severe, persistent insomnia, sleep hygiene acts as a necessary foundation, but it is statistically inferior to comprehensive Cognitive Behavioral Therapy for Insomnia (CBT-I), which remains the gold standard, first-line medical treatment 515354. CBT-I goes beyond simple habit changes, actively restructuring the deep-seated psychological anxieties and maladaptive behaviors that prevent patients from achieving restful sleep 53.
Recognizing the vast public health implications of sleep deprivation - which is linked to higher risks of cardiovascular disease, obesity, depression, and cognitive decline - major institutions are aggressively elevating the status of sleep health 141555661. The AASM has recently issued groundbreaking clinical guidelines expanding beyond outpatient behavioral advice, establishing formal inpatient screening protocols to ensure that obstructive sleep apnea and sleep quality are managed as vital signs during hospitalizations, ensuring continuity of care from the hospital bed to the home environment 5758.
To optimize rest and build a robust foundation for long-term health, scientific literature recommends implementing the following evidence-backed sleep hygiene behaviors:
- Establish a Fixed Wake Time: Consistency in waking up anchors the circadian rhythm. The SCN relies on a predictable, rigid morning routine to accurately set the biological clock for the subsequent night's sleep onset 7853.
- Harness Morning Light: Expose the eyes to natural daylight or a bright clinical light therapy box (minimum 2,500 lux) for 30 to 60 minutes immediately upon waking. This suppresses residual melatonin production, clears morning sleep inertia, and pulls the circadian phase earlier 161819.
- Respect the Adenosine Curve: Avoid consuming caffeine in the late afternoon. If an individual is genetically prone to slow metabolism, a strict noon cutoff is recommended to ensure adenosine receptors are unblocked by the desired bedtime 21153.
- Create an Autonomy Buffer: To combat the psychological trap of revenge bedtime procrastination, deliberately carve out 30 to 60 minutes of unstructured, non-productive leisure time during the daytime or early evening, reducing the subconscious drive to stay up late 3739.
- Regulate the Thermal Environment: Keep the bedroom comfortably cool (optimally around 60°F to 67°F for the general population, slightly warmer for seniors) to facilitate the necessary core body temperature drop required to initiate and maintain deep slow-wave sleep 252753.
- Implement a Digital Sundown: Transition to warm, dim lighting at least 90 minutes before bed. If screens absolutely must be used, utilize high-mDFD amber lenses to protect endogenous melatonin secretion from short-wavelength blue light 152253.
- Limit Late-Night Alcohol: While a drink may induce rapid drowsiness, it severely truncates REM sleep and guarantees physiological fragmentation, elevated heart rates, and awakenings during the second half of the night 293032.
Bottom line
Building better sleep habits requires significantly more than merely spending eight hours in bed; it demands the active, daily synchronization of the body's master internal clock (the circadian rhythm) and the management of the natural cellular drive for rest (adenosine accumulation). While clinical science strongly supports physical interventions such as morning sunlight exposure, cool bedroom temperatures, and the elimination of evening alcohol and caffeine, it is equally important to recognize that ideal sleep duration and chronotype timing vary substantially based on individual genetics. Ultimately, addressing the psychological need for daytime autonomy is just as critical as optimizing the physical bedroom environment to achieve restorative, long-term sleep health.