What Is Retatrutide and How Does It Compare to GLP-1s
Retatrutide is an investigational, next-generation weight-loss medication that targets three distinct metabolic hormone pathways simultaneously to achieve unprecedented weight reduction. By mimicking GLP-1, GIP, and glucagon, the drug has demonstrated an average weight loss of up to 30.3% over two years in clinical trials, rivaling the effects of bariatric surgery. However, retatrutide remains strictly experimental, carries higher rates of certain gastrointestinal side effects, and is not expected to receive FDA approval until late 2027 at the earliest.
The Evolution of Metabolic Medicine
The landscape of obesity and metabolic treatment has progressed at a blistering pace over the last decade, evolving from single-target medications to complex, multi-receptor therapies.
Early medical interventions were dominated by single-agonist therapies that targeted the glucagon-like peptide-1 (GLP-1) receptor. Medications like semaglutide (sold as Wegovy and Ozempic) became standard-of-care by suppressing appetite and yielding average body weight reductions of roughly 15% 12. The next generation introduced dual-agonist therapies, most notably tirzepatide (sold as Zepbound and Mounjaro). By adding glucose-dependent insulinotropic polypeptide (GIP) to the GLP-1 backbone, tirzepatide pushed average weight loss closer to 21% 12.
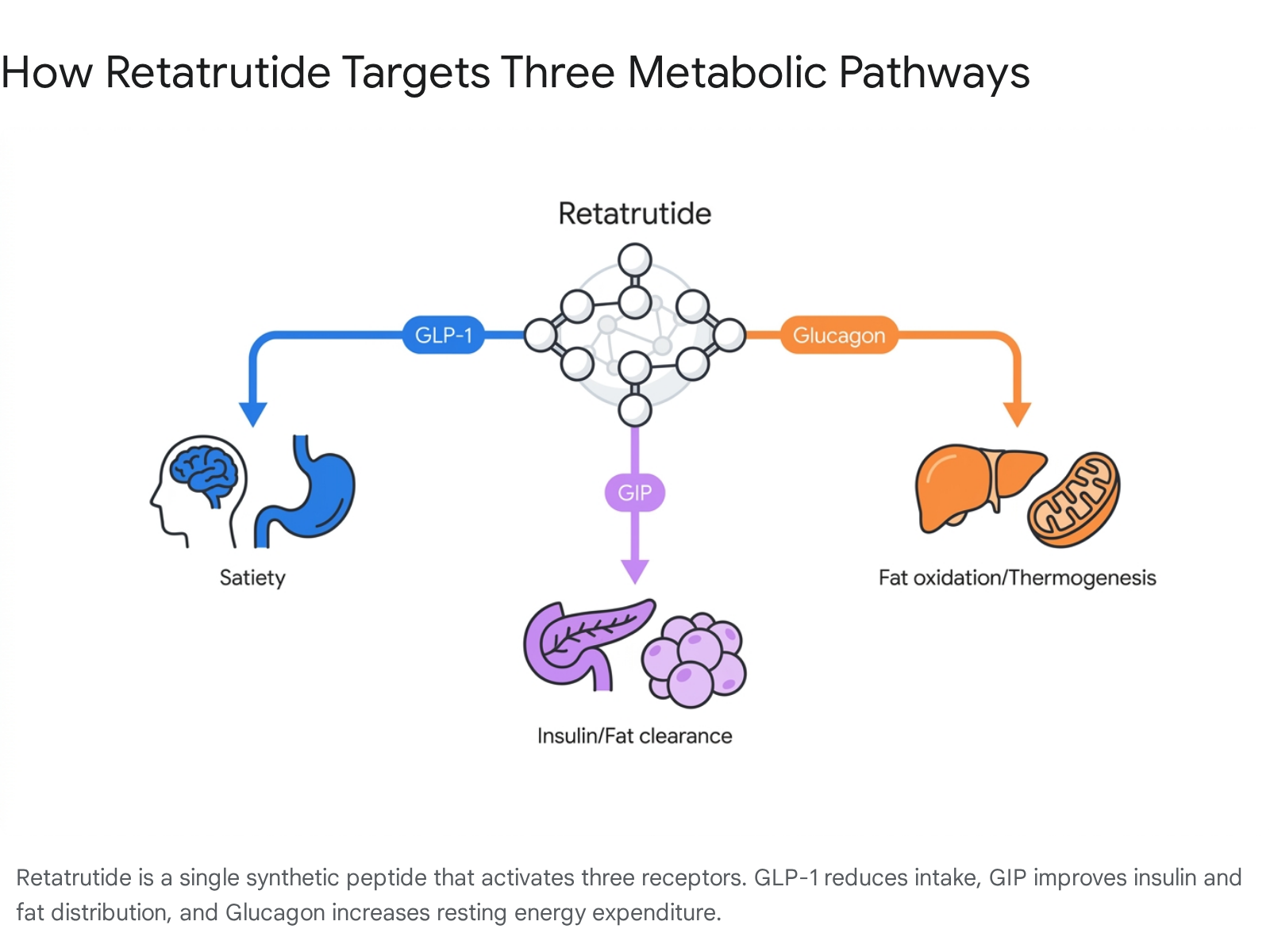
Now, researchers are evaluating the "triple agonist" approach. Retatrutide (development code LY3437943), developed by Eli Lilly, is a single synthetic peptide engineered to simultaneously activate three critical hormonal pathways: GLP-1, GIP, and the glucagon receptor (GCGR) 345. By engaging all three receptors, retatrutide represents a major shift from simply suppressing appetite to actively reprogramming how the human body metabolizes and expends energy 67.
| Generation | Medication (Brand Names) | Mechanism of Action | Average Phase 3 Weight Loss | Current FDA Status (as of 2026) |
|---|---|---|---|---|
| First | Semaglutide (Wegovy, Ozempic) | GLP-1 (Single Agonist) | ~15% | Approved |
| Second | Tirzepatide (Zepbound, Mounjaro) | GLP-1 + GIP (Dual Agonist) | ~21% | Approved |
| Third | Retatrutide (Investigational) | GLP-1 + GIP + Glucagon (Triple Agonist) | ~28 - 30% | Investigational (Expected 2027+) |
Note: Averages are based on maximum studied doses across pivotal Phase 3 trials in non-diabetic populations 125.
How Retatrutide Works: The Triple Agonist Mechanism
To understand why retatrutide is producing such dramatic clinical results, it is helpful to look at how the three hormonal pathways complement one another.
Traditional weight loss is notoriously difficult to maintain because of metabolic adaptation 6. When a person consumes fewer calories and loses weight, the body instinctively responds by slowing its resting metabolic rate to conserve energy, leading to a plateau 67. Retatrutide is uniquely designed to counteract this biological defense mechanism.
Researchers often use a railway analogy to explain this complex interaction. Imagine the body's metabolism is a train system struggling with faulty signals and slow engines. Most medications send one "engineer" to fix the problem. Retatrutide sends three 6.
GLP-1: The Appetite Suppressor
The GLP-1 receptor is the foundational target for modern obesity drugs. When retatrutide activates GLP-1 receptors, it delays gastric emptying, meaning food moves from the stomach to the small intestine much more slowly 610. Furthermore, it acts directly on appetite centers in the hypothalamus (such as parabrachial neurons), reducing hunger signals and generating robust feelings of satiety 610. This is the "engineer" that repairs the signaling lights, preventing the metabolic train from taking on excess fuel 6.
GIP: The Insulin and Fat Manager
The GIP receptor works synergistically with GLP-1 to enhance insulin secretion in a glucose-dependent manner, helping to stabilize post-meal blood sugar 410. Beyond the pancreas, GIP receptors are abundant in adipose (fat) tissue. Engaging GIP promotes the breakdown of adipose tissue and healthier fat storage, preventing toxic lipid buildup 10. Notably, combined GIP and GLP-1 activation creates a synergistic appetite-suppressing effect in the brain that exceeds what either hormone can achieve alone 10.
Glucagon: The Energy Burner
The inclusion of glucagon receptor (GCGR) agonism is the defining feature that separates retatrutide from approved weight-loss drugs 45. Historically, elevating glucagon was avoided in metabolic therapies because it prompts the liver to release stored glucose 7. However, when perfectly balanced with GLP-1 and GIP (which keep insulin and glucose optimized), glucagon activation drives lipolysis (the breakdown of fat) and significantly increases resting energy expenditure via thermogenesis 46.
In practical terms: while the GLP-1 component reduces the calories coming in, the glucagon component increases the calories going out, fighting the body's natural urge to slow its metabolism 67.
Efficacy: The TRIUMPH Phase 3 Trial Program
The clinical development of retatrutide is being driven by the TRIUMPH program, a massive global initiative encompassing multiple Phase 3 trials involving over 5,800 participants 89. Preliminary data released in late 2025 and mid-2026 has sent shockwaves through the medical community, suggesting efficacy that touches the outcomes typically reserved for invasive bariatric surgery 510.
To capture diverse patient populations, Eli Lilly utilized a "basket trial" design, nesting various comorbidity evaluations (like sleep apnea and osteoarthritis) inside broader weight management trials 8.
| Phase 3 Trial | Target Population | Primary Endpoints | Expected Readout/Status |
|---|---|---|---|
| TRIUMPH-1 | Obesity/overweight without diabetes | Weight loss percentage | Topline results reported May 2026 |
| TRIUMPH-2 | Obesity/overweight with Type 2 Diabetes | Weight loss, HbA1c reduction | Anticipated mid-to-late 2026 |
| TRIUMPH-3 | Obesity with Cardiovascular Disease | Long-term safety, weight loss | Expected late 2026 |
| TRIUMPH-4 | Obesity with Knee Osteoarthritis | Weight loss, WOMAC pain scores | Topline results reported Dec 2025 |
| TRIUMPH-Outcomes | Obesity with ASCVD or CKD | Reduction of Major Adverse Cardiovascular Events (MACE) | Expected 2027 - 2028 |
Data aggregated from ClinicalTrials.gov and Eli Lilly trial design publications 91516.
TRIUMPH-1: General Obesity Results
TRIUMPH-1 is the flagship 80-week, randomized, double-blind master trial evaluating 2,339 adults with obesity or overweight without diabetes 1011. The topline results reported by Eli Lilly in May 2026 revealed staggering figures.
Participants on the maximum 12 mg dose lost an average of 28.3% of their body weight (an average of 70.3 lbs) over 80 weeks 1012. The trial demonstrated that 45.3% of individuals in the highest dose group lost 30% or more of their body weight, an efficacy ceiling previously untouched by pharmacotherapy 1013. Consequently, 65.3% of the 12 mg cohort saw their BMI drop below 30, meaning they were no longer clinically classified as obese 1013.
To test the drug's durability, TRIUMPH-1 included a blinded extension for a subset of 532 patients with severe obesity (BMI ≥35). After 104 weeks, average weight loss for this group reached 30.3% (85.0 lbs), showing that the medication could sustain prolonged weight loss without the traditional plateau 1013.
Even at lower doses, the results were highly significant. The 4 mg dose - which requires only a single dose-escalation step from the starting dose - yielded a 19.0% body weight reduction over 80 weeks. This places a low dose of retatrutide in the same efficacy tier as the maximum approved dose of semaglutide, but with potentially better real-world tolerability due to fewer dose-escalation phases 101314.
TRIUMPH-4: Obesity and Osteoarthritis
Obesity frequently exacerbates structural joint conditions. The TRIUMPH-4 trial specifically evaluated retatrutide in 445 patients with obesity and moderate-to-severe knee osteoarthritis (Kellgren-Lawrence Grade 2 or 3) 1516.
Reported in late 2025, the 68-week trial showed a 28.7% average weight reduction for the 12 mg dose 1516. Beyond the scale, the trial met its co-primary endpoints by demonstrating a 75.8% reduction in WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) pain scores 1617. Remarkably, up to 14.1% of participants receiving the 9 mg dose and 12.0% on the 12 mg dose reported being completely free of knee pain at 68 weeks, compared to just 4.2% on placebo 16.
Beyond the Scale: Body Composition and Liver Health
As highly potent weight-loss drugs enter the mainstream, the medical community has begun scrutinizing them over concerns regarding "skinny fat" outcomes - situations where patients lose a significant proportion of lean muscle mass alongside body fat.
Fat Loss vs. Muscle Loss
Data from Phase 2 and Phase 3 sub-studies (including those published in The Lancet) indicate that retatrutide users do lose lean mass, which is a physiological reality of all rapid weight loss. Specifically, about 20% to 35% of the total weight lost on GLP-1 and incretin therapies is lean tissue 1224.
Body composition analysis shows that retatrutide yields a fat-to-lean mass loss ratio of roughly 3:1 (approximately 75% fat to 25% lean mass). This proportion is identical to the muscle loss ratio seen with tirzepatide and semaglutide 2425.
However, because the total weight loss on retatrutide is substantially higher, the absolute volume of lean mass lost is also higher 25. For example, if a patient loses 35 lbs on semaglutide, they may lose 9 lbs of lean mass. If a patient loses 70 lbs on retatrutide, they could lose up to 24 lbs of muscle 1225. Detailed DXA scans from Phase 2 studies showed that the 8 mg dose reduced total fat mass by 26.1% and visceral (belly) fat by up to 31.4% at 36 weeks 18. Experts emphasize that this profound weight reduction makes regular resistance training and high protein intake critical components of a retatrutide regimen to prevent frailty 225.
Reversing Hepatic Fat (MASLD)
Where retatrutide severely outperforms its single and dual-agonist predecessors is in clearing hepatic (liver) fat, largely thanks to the glucagon receptor pathway 1025.
A dedicated Phase 2 sub-study focusing on metabolic-associated steatotic liver disease (MASLD), published in Nature Medicine, showed extraordinary results. Participants on the 12 mg dose experienced an average 86.0% reduction in liver fat at 48 weeks 327. Even more striking, 93% of patients achieved completely normal liver fat levels (under 5%) 327. This degree of lipolysis suggests retatrutide could eventually become a frontline therapy for severe metabolic liver conditions, acting as a highly effective tool against fatty liver disease 2719.
Safety, Side Effects, and Tolerability Concerns
The unprecedented potency of retatrutide comes with a proportional increase in side effect severity. While the general safety profile is consistent with the broader incretin class, the intensity of adverse events at high doses poses questions about patient adherence.
Gastrointestinal and Neurological Effects
The most common side effects are gastrointestinal, generally peaking during the dose-escalation phase as the body adjusts to the medication 513. In the TRIUMPH-1 trial's 12 mg cohort, patients frequently reported nausea (42.4%), diarrhea (32.0%), constipation (26.1%), and vomiting (25.3%) 1314.
Additionally, researchers observed a neurological side effect called dysesthesia - abnormal skin sensations typically described as burning, tingling, or "pins and needles." In TRIUMPH-1, 12.5% of highest-dose users experienced this 12. In the TRIUMPH-4 osteoarthritis trial, the rate was even higher, reaching 20.9% in the 12 mg group compared to 0.7% on placebo 16. While these events were generally mild to moderate and resolved during treatment, the rate is significantly higher than what is observed with tirzepatide 1214.
Heart Rate and Bone Density Monitoring
Two mechanism-specific side effects require ongoing clinical monitoring: 1. Elevated Heart Rate: The glucagon component of retatrutide directly increases cardiac output and sympathetic drive. This results in an increased resting heart rate by an average of 5 to 7 beats per minute (bpm) at the 12 mg dose 2920. This is slightly higher than the 3 to 5 bpm increase typical of semaglutide and tirzepatide. Phase 2 data showed no dose-dependent increase in dangerous arrhythmias, but long-term cardiovascular safety is still being monitored closely 2920. 2. Bone Mineral Density (BMD): Rapid, profound weight loss is highly correlated with bone density reductions. Preliminary medical data suggests approximately 1% to 3% BMD loss for every 10% of body weight lost 12. Given retatrutide's 30% weight loss ceiling, researchers are tracking osteoporosis risks, especially considering that in some non-diabetic studies, intense weight loss was linked to higher osteoporosis risk compared to those maintaining stable weights 1221.
Discontinuation Rates
Tolerability is the ultimate test of any chronic weight management drug. If a patient cannot stomach the side effects, the efficacy is moot. In the TRIUMPH-1 trial, 11.3% of retatrutide participants on the highest 12 mg dose abandoned the treatment due to adverse events 1213.
For context, discontinuation rates for maximum-dose tirzepatide and semaglutide in their respective pivotal trials were roughly 6.1% and 8.0% 12. Analysts and clinicians project that while tirzepatide may remain the standard "go-to" medication for the broader public due to its balanced tolerability, retatrutide may eventually be reserved for patients at the extreme high end of the BMI spectrum, or for those who plateau on dual-agonists 1221.
Cardiovascular Outcomes: The TRIUMPH-Outcomes Trial
Weight loss and pain reduction are excellent clinical milestones, but the ultimate goal of metabolic medicine is reducing mortality. Does retatrutide prevent heart attacks and strokes?
Initial data shows strong improvements in surrogate cardiovascular risk factors. Topline Phase 3 results demonstrate that retatrutide lowers systolic blood pressure (by up to 14.0 mmHg), significantly reduces waist circumference (up to 24.1 cm or 9.5 inches), and lowers LDL cholesterol by roughly 20%, likely due to glucagon-receptor-driven PCSK9 degradation 151316.
To confirm these benefits translate to longer lives, Eli Lilly initiated the TRIUMPH-Outcomes trial (NCT06383390) 22. This massive, five-year study is currently tracking approximately 10,000 patients aged 45 and older with obesity and established atherosclerotic cardiovascular disease (ASCVD) or chronic kidney disease (CKD) 2923. The primary endpoint is the reduction of Major Adverse Cardiovascular Events (MACE). Because cardiovascular outcome trials require years to accumulate sufficient clinical events to prove statistical significance, readout for this trial is not expected until 2027 or 2028 29.
FDA Approval Timeline: When Will Retatrutide Be Available?
Despite the immense public interest and strong topline Phase 3 data, retatrutide is still years away from reaching pharmacy shelves. It remains strictly an investigational molecule.
The regulatory path requires the completion and full analysis of the core TRIUMPH trials before an application can be filed. * NDA Submission: Eli Lilly is expected to analyze the final Phase 3 data and submit a New Drug Application (NDA) to the FDA in Q4 2026 or Q1 2027 2724. * FDA Review Window: A standard FDA review for a new molecular entity takes approximately 10 months from the date the application is accepted 2425. * Projected Launch: Assuming the safety profile remains acceptable and manufacturing logistics are established, formal FDA approval and commercial launch are anticipated between late 2027 and mid-2028 2724.
UK and European approvals (via the MHRA and EMA) typically follow 6 to 12 months after FDA authorization, placing international availability squarely in 2028 2726.
The Dangers of the Unregulated Gray Market
The viral hype surrounding retatrutide's efficacy has fueled a dangerous gray market, amplified by social media influencers and unregulated online telehealth platforms 27.
Because the drug is still entirely investigational, it does not hold a USP (United States Pharmacopeia) monograph, is not an approved drug component, and is not on the FDA's drug shortage list 2829. Consequently, it is federally illegal for compounding pharmacies to manufacture or sell retatrutide under standard 503A or 503B compounding exemptions 2829. The compounding loophole that allowed patients to access semaglutide and tirzepatide during national shortages does not legally apply to a drug that has never been approved 30.
In late 2025, the FDA issued a wave of warning letters to online entities and compounding pharmacies attempting to sell unapproved retatrutide 2728. Medical experts warn that gray-market retatrutide - often sold under the guise of "research peptides" or "not for human consumption" - carries severe health risks 2931. Patients buying these bulk compounds face the threat of contamination, wildly incorrect dosing, or receiving entirely counterfeit substances 2531. Furthermore, utilizing an experimental triple-agonist without rigorous medical oversight exposes users to unmonitored cardiac, hepatic, and gastrointestinal risks 2731.
Bottom line
Retatrutide's triple-agonist mechanism represents a genuine scientific breakthrough in metabolic medicine, pushing average weight loss past 30% and directly rivaling bariatric surgery. Its unique ability to activate the glucagon receptor alongside GLP-1 and GIP allows it to aggressively clear liver fat and increase energy expenditure, making it highly effective for severe obesity. However, this potency comes with higher rates of gastrointestinal side effects, potential muscle mass loss, and a resting heart rate increase that requires long-term cardiovascular monitoring. Until formal FDA approval - expected no earlier than late 2027 - retatrutide remains strictly experimental, and acquiring it outside of registered clinical trials is both illegal and unsafe.