How to Read Health News Without Being Misled
The core strategy for reading health news critically relies on shifting focus away from sensationalized relative risk claims and isolated novel findings, and instead anchoring comprehension in absolute risk, the hierarchy of scientific evidence, and established medical consensus. By rigorously evaluating the methodological validity of underlying studies and cross-referencing bold claims against institutional health watchdogs, consumers can effectively neutralize manipulative media framing. Ultimately, digital health literacy demands a robust diagnostic filter that systematically screens out unverified social media anecdotes, artificial intelligence hallucinations, and financially motivated wellness influencers to uncover verifiable, peer-reviewed data.
The modern information ecosystem has engineered a pervasive and psychologically exhausting societal phenomenon known as "health whiplash" 12. It is a uniquely relatable and ubiquitous frustration: a consumer reads a widely circulated headline on a Tuesday hailing coffee as a miraculous antioxidant elixir capable of adding decades to human life, only to encounter an equally viral article by Thursday condemning that exact same beverage as a deadly toxin irrevocably linked to heart failure 12. This jarring oscillation in public health advice is not merely an annoyance; it is a structural failure of science communication that actively degrades public trust in scientific institutions, fosters widespread cynicism, and leaves patients paralyzed by contradictory guidance 23.
Health whiplash is the direct byproduct of an attention economy that monetizes human anxiety and hope. Historically, scientific discourse advanced through slow, meticulous, and heavily caveated academic journals designed to be read by subject-matter experts. Today, this inherently complex and nuanced scientific process is violently compressed into 280-character micro-blogs, 60-second algorithmic short-form videos, and hyper-condensed, artificially generated search summaries 4567. The consequence of this compression is a profound and dangerous disconnect between the slow, incremental, and probabilistic nature of genuine medical research and the absolute certainty demanded by modern news consumers 18.
To survive and thrive in a landscape where clickbait headlines and influencer-driven "miracle cures" aggressively compete for attention alongside rigorous, peer-reviewed epidemiological data, individuals must cultivate advanced, critical health literacy. Defined by the World Health Organization (WHO) as the cognitive and social skills required to access, understand, and apply information in ways that promote and maintain good health, health literacy is no longer merely about a patient's ability to read a prescription label 91011. In the post-2023 digital age, functional health literacy has evolved into critical health literacy; it now requires the capacity to dissect study methodologies, detect mathematical manipulation, identify algorithmic biases, and recognize the inherent boundaries of generative artificial intelligence 91213. Furthermore, modern health literacy is recognized through a socio-ecological model, acknowledging that an individual's ability to process health information is heavily influenced by the surrounding digital environment, cultural norms, and the regulatory frameworks governing media platforms 1014.
This comprehensive report deconstructs the mechanics of modern medical journalism, outlines international frameworks for evaluating health claims, and provides actionable, data-driven strategies to dismantle misinformation across all contemporary media vectors.
Why Does Health Advice Always Seem to Change?
A fundamental driver of health whiplash is a widespread public misunderstanding of how the scientific method operates in practice. Scientific knowledge does not advance in clean, linear, and definitive steps that culminate in an absolute, unassailable truth. Instead, it is a messy, iterative, and highly probabilistic process characterized by continuous refinement 18.
The most common misconception propagated by poor medical journalism is the idea that a single new study definitively "proves" a novel claim or entirely invalidates decades of established scientific consensus 1215. In reality, science builds upon a vast, interconnected aggregate of data 228. When a novel study contradicts previous findings, it rarely means the older science was entirely fraudulent or that researchers are mindlessly flip-flopping. More often, the new research has explored a different demographic subset, utilized a larger and more statistically significant sample size, controlled for a previously unrecognized confounding variable, or extended the timeline of clinical observation 18.
The perception of constant instability in health advice is artificially amplified by systemic biases within academic publishing and media reporting. The media exhibits a profound bias toward novelty; a single preliminary study - especially one yielding unexpected, counterintuitive, or contrarian results - is highly newsworthy and commands massive digital engagement 1. Conversely, replication studies that meticulously confirm existing knowledge, or studies that yield null results (finding no statistically significant effect), are rarely published by top-tier journals and almost never make the evening news 1716. This dynamic creates a pervasive "publication bias" and a phenomenon known in academia as the "drawer effect," where researchers file away negative or inconclusive results and only publish positive findings 171617. Consequently, the public is bombarded with statistical anomalies rather than the stable, albeit boring, accumulation of scientific consensus 1716. Furthermore, the pressure on researchers to secure funding and tenure often pushes them to engage in "p-hacking" - manipulating statistical analyses until a significant, publishable p-value is achieved, even if the real-world effect is negligible 16.
Compounding this issue is the media's insistence on binary framing. Scientific conclusions are almost always probabilistic, expressed in terms of confidence intervals, hazard ratios, and margins of error 116. A responsible researcher might conclude that an intervention is "slightly more likely to help than harm for most people under specific, controlled conditions" 1. The media ecosystem, however, translates this delicate nuance into binary, absolutist directives: "Do this" or "Don't do that." When subsequent, higher-powered research refines the initial probability, the media reports it as a total reversal, creating the illusion of scientific incompetence 12.
It is also crucial to differentiate between healthy scientific skepticism and outright denialism. History is replete with examples of "heretical" ideas that eventually overturned consensus, such as Ignaz Semmelweis's early, highly mocked advocacy for handwashing, or the discovery of the bacterial causes of ulcers 2. Because of these historical precedents, some modern content creators weaponize the concept of skepticism to peddle pseudoscientific wellness products 28. However, true scientific skepticism involves evaluating the totality of available evidence for its methodological quality 8. Denialists and cranks, conversely, cherry-pick isolated data points, vastly exaggerate the quality of preliminary studies, and ignore the overwhelming weight of aggregate evidence - such as the massive epidemiological consensus linking obesity to adverse health outcomes or HIV to AIDS 8.
Resistance to updating one's beliefs in the face of changing advice also reflects a deep cognitive vulnerability. Research from Brown University indicates that individuals who drastically overestimate their own understanding of a complex topic are the most likely to deviate from established scientific consensus 18. This overconfidence creates a barrier to learning; if people falsely believe they already possess a thorough understanding of viral transmission or nutritional biochemistry, they exhibit minimal motivation to absorb new, corrective information 18. Conversely, frameworks like the Gateway Belief Model (GBM) demonstrate that effectively communicating the actual percentage of scientific consensus on an issue can directly shift public perception and correct dangerous misperceptions, highlighting the critical need for journalists to report the aggregate consensus rather than focusing exclusively on outlier studies 19. The ability of the scientific community to update beliefs and revise guidelines in light of new, high-quality evidence is not a weakness of the medical establishment; it is the defining, self-correcting strength of the scientific method 18.
What Does "Peer-Reviewed" Actually Mean?
The phrase "peer-reviewed" is frequently touted in health journalism as the ultimate gold standard of scientific validity, but the term is severely misunderstood by the general public, who often view it as an ironclad guarantee of absolute truth 217. In reality, peer review is merely a quality control mechanism - a baseline threshold for basic academic credibility, not a divine declaration of infallibility 217.
When a researcher submits a manuscript to a legitimate academic journal, the editorial board sends it to independent experts (peers) operating within the same highly specialized field. These reviewers scrutinize the study's experimental design, statistical methods, ethical compliance, and the internal logic of its stated conclusions 2. They may recommend outright rejection, request major methodological revisions, or approve the manuscript for publication. While this grueling process filters out blatant methodological errors, gross miscalculations, and entirely unfounded claims, it cannot catch every instance of subtle data manipulation, nor does it guarantee that the findings will apply broadly to the general human population 216.
The integrity of the peer-review process is currently under unprecedented assault by the proliferation of "predatory journals" 21622. These entities operate on a pay-to-play model, charging authors exorbitant publication fees to host their work online while providing little to no actual peer review or editorial oversight 216. Because these predatory journals often adopt legitimate-sounding names, a layperson - and even a rushed journalist - might mistake a completely unvetted, pseudoscientific paper for a rigorous medical breakthrough 216. Sophisticated readers and journalists must look beyond the mere claim of peer review and evaluate the journal's "Impact Factor," a metric indicating how often the average article in that journal is cited by other scientists, while actively cross-referencing publishers against watchdogs like Beall's List of potential predatory open-access publishers 222. Furthermore, assessing the credentials of the researcher using tools like Google Scholar to check their H-index (a measure of scientific productivity and citation impact) helps verify if the author is actually an expert in the specific field they are publishing in, rather than a contrarian building a career by speaking authoritatively on topics outside their discipline 2.
Crucially, even within legitimate, high-impact journals, not all studies that pass peer review are created equal. The quality and reliability of evidence provided by medical research are strictly governed by the hierarchy of study designs 20212223.
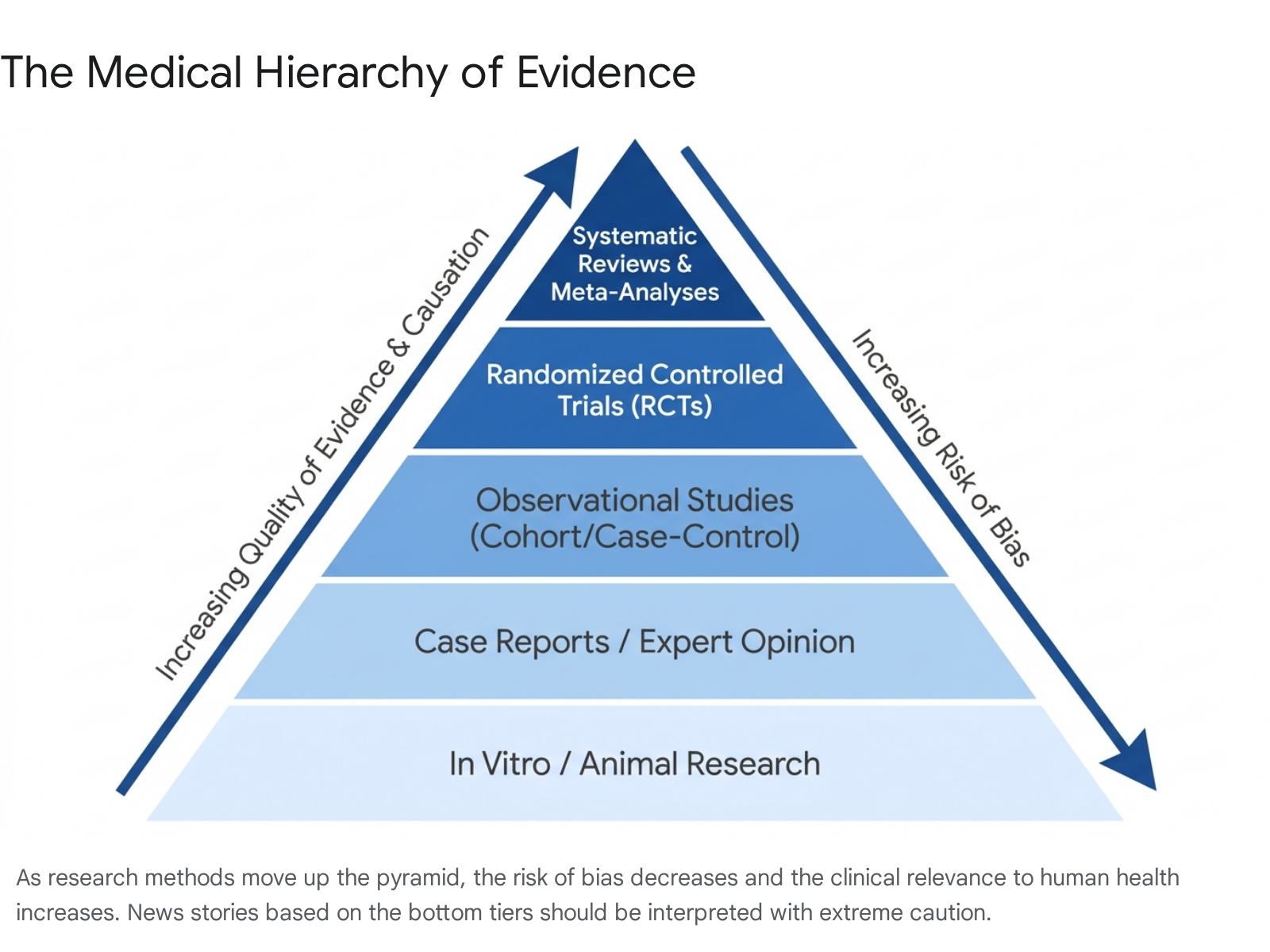
A meticulously peer-reviewed animal study carries vastly different clinical weight than a peer-reviewed human randomized controlled trial 202728. Relying on an in vitro (test tube) study to dictate widespread human dietary habits is a hallmark of poor health literacy and irresponsible journalism 28.
To effectively navigate medical news, one must intimately understand the differences between study types, their inherent strengths, and their critical limitations, as detailed in the comprehensive table below:
| Study Type | Definition & Mechanism | Scientific Strengths | Limitations & Caveats |
|---|---|---|---|
| In Vitro & Animal Studies | Foundational research conducted on isolated cellular structures in a laboratory setting (in vitro) or on animal models (e.g., mice, rats, primates) 202728. | Offers highly controlled environments; essential for initial testing of biological mechanisms, genetic pathways, and basic chemical toxicity before human exposure 202728. | Lowest clinical relevance for humans. Animal metabolisms and cellular environments differ vastly from humans. A compound that destroys cancer cells in a mouse model may be highly lethal or entirely ineffective in a human body. These studies do not reliably predict real-world human outcomes and should never be the basis for lifestyle changes 1728. |
| Observational Studies (Cohort, Cross-Sectional & Case-Control) | Researchers observe large populations over extended periods without actively interfering or prescribing treatments, tracking their organic habits, environments, and subsequent health outcomes 202123. | Excellent for identifying long-term epidemiological trends and associations (e.g., the historical link between smoking and lung cancer) that would be highly unethical or practically impossible to test experimentally 823. | Cannot definitively prove causation. Highly vulnerable to "confounding variables." For example, an observational study might find that people who drink red wine have lower COVID-19 infection rates. However, red wine drinkers might also be wealthier, have better access to healthcare, or work from home - these confounders, not the wine, likely explain the health outcome 172829. |
| Randomized Controlled Trials (RCTs) | Human participants are randomly assigned to either an experimental group (receiving the active treatment) or a control group (receiving a placebo or the current standard of care). Both researchers and subjects are ideally "blinded" to who is receiving what 20212729. | The gold standard for establishing causation in primary research. The process of randomization mathematically neutralizes confounding variables, effectively isolating the true physiological effect of the specific intervention 21232729. | Incredibly expensive, highly time-consuming, and often conducted on highly specific, less diverse clinical populations. Because they occur in strictly controlled clinical settings, their results may not perfectly mirror how an intervention performs in the chaotic "real world" (implementation science) 23. |
| Systematic Reviews & Meta-Analyses | A comprehensive, exhaustive mathematical synthesis of all existing high-quality RCTs and observational studies on a specific topic, aggregating data from tens of thousands of participants 202122. | The absolute highest level of clinical evidence. By aggregating data, it smooths out the statistical anomalies of individual studies, drastically increases statistical power, and reveals the true, overarching scientific consensus 20212223. | Only as reliable as the underlying studies it analyzes ("garbage in, garbage out"). Remains highly vulnerable to publication bias if null results were never published in the primary literature, potentially skewing the aggregated data 1716. |
When evaluating a news article, identifying exactly where the referenced study sits on this established hierarchy is the absolute first step in critical appraisal 202324. If a media outlet declares a new "miracle cure" based solely on an open-label observational study or an isolated animal model, the claim should be immediately dismissed as dangerously sensationalized 172829.
How Can I Spot a Sensationalized Headline?
The most potent, ubiquitous, and mathematically deceptive weapon in a health journalist's arsenal for generating clicks - and the most dangerous analytical trap for the everyday reader - is the deliberate conflation of relative risk and absolute risk 25262734.
Headlines are meticulously engineered to capture fleeting digital attention, which means they heavily and almost exclusively favor relative statistics. A headline that screams, "Eating Processed Meat Increases Bowel Cancer Risk by 50%!" or "New Drug Cuts Heart Attack Risk in Half!" sounds terrifying or miraculous, respectively 262728. However, relative risk merely compares the likelihood of an event happening in one specific group versus another, without ever providing the baseline probability of the event happening in the first place 253428. When researchers communicate with the lay public, using absolute risk represented as a tangible proportion is scientifically proven to be the best way to help populations accurately understand their true vulnerability 34.
To understand how catastrophically misleading relative framing can be, consider a real-world mathematical analogy. Imagine a rare genetic condition that affects 1 in 10,000 people. This means the absolute risk - the actual, tangible probability of an individual developing the condition in reality - is an incredibly low 0.01%. Now, imagine a sensationalized new study finds that drinking a specific brand of soda increases the risk of this condition by a staggering 50% relative to non-drinkers. A 50% relative risk increase means the absolute risk jumps from 1 in 10,000 to merely 1.5 in 10,000 25.
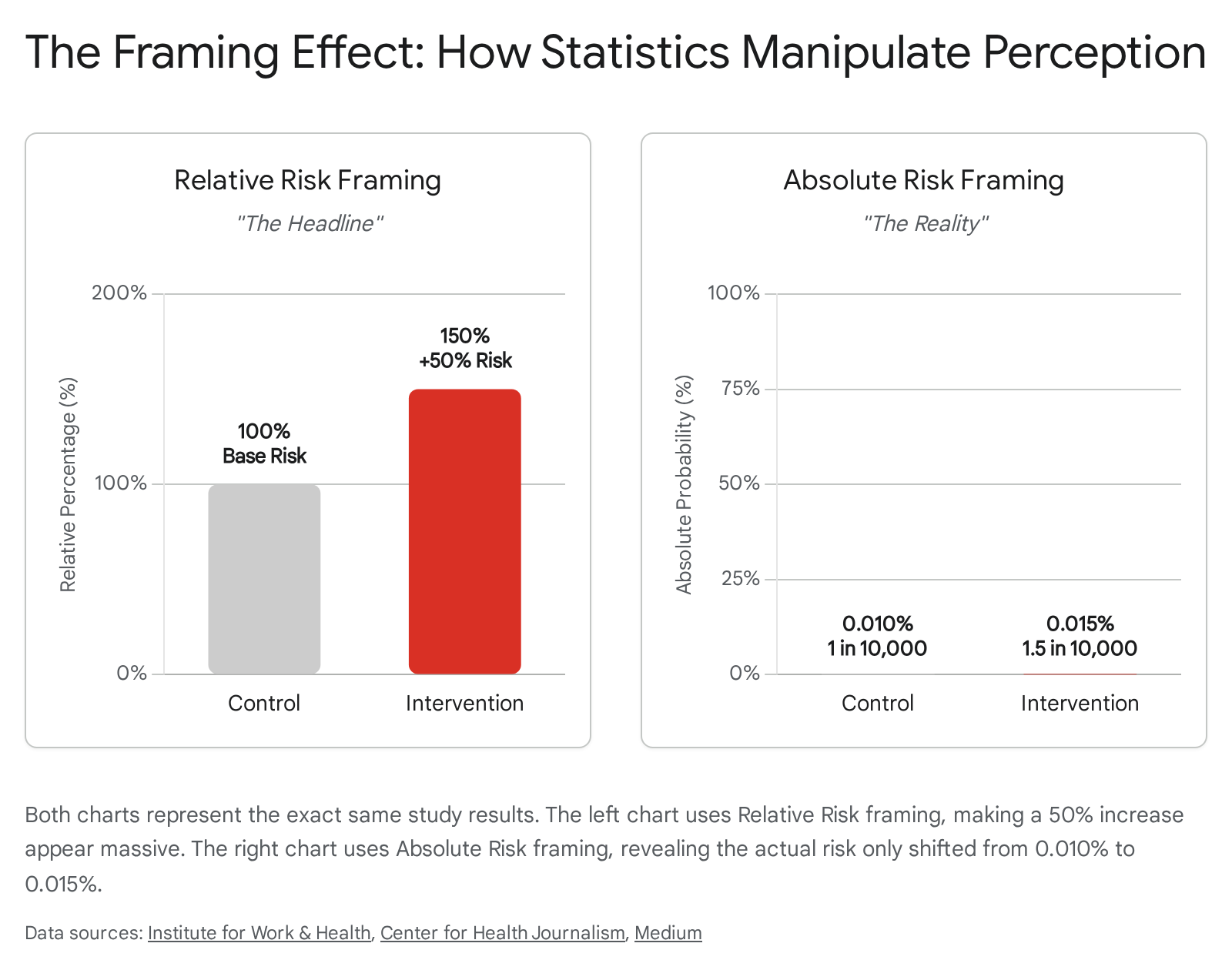
Expressed in absolute, real-world terms, the risk to the individual has risen by an almost imperceptible 0.005 percentage points. The individual's chance of not getting the disease shifted from an overwhelmingly safe 99.99% to 99.985%. Yet, the marketer of a competing health product, or the sensationalist journalist seeking viral engagement, will actively ignore the absolute numbers and proudly publish the 50% relative increase because it sounds infinitely more dramatic 2634.
As noted by researchers at the Dartmouth Institute for Health Policy, relying solely on relative risk data is akin to holding a "50% off" coupon for a massive department store, but having no idea if the coupon applies to a diamond necklace or a single pack of chewing gum; without knowing the absolute baseline value of the item, the percentage itself has absolutely no actionable meaning 26. Similarly, Cancer Research UK utilizes the analogy of a deck of cards: the absolute risk of picking any Heart is 25%, but the absolute risk of picking the Queen of Diamonds is roughly 2% 27. Therefore, one could truthfully claim that the "risk" of picking a Heart is over ten times greater (a relative metric) than picking the Queen of Diamonds, but this sounds far more intimidating than the underlying absolute reality 27.
Responsible medical journalism watchdogs, such as the US Health News Review and the Australian Media Doctor initiative, strictly penalize articles that report relative risk without providing the grounding context of absolute risk 172629. A hallmark of high-quality, ethical reporting is the inclusion of both metrics, empowering the reader to judge the true clinical significance of the findings for themselves 263031. For example, when STAT reported on new aspirin guidelines, they were praised for providing both data points: they noted a 20 percent relative reduction in cardiovascular risk, but explicitly grounded it in the absolute reality that serious cardiovascular events dropped from a mere 0.57 percent to 0.51 percent 26. This is the critical context that entirely neutralizes health whiplash. In contrast, the Guardian once reported a terrifying "70% increase" in cancer among women following the Fukushima Daiichi nuclear disaster, while the Wall Street Journal correctly framed the exact same data by noting the absolute increase was a "tiny" 0.5 percent (moving from a baseline of 0.77 percent to 1.29 percent) 27.
Beyond mathematical statistics, the actual vocabulary and phrasing used by journalists, marketers, and content creators offer immediate, glaring clues about the reliability of the information presented. Recognizing manipulative language is a core, foundational component of media literacy. Below is a comparative matrix designed to help readers instantly identify linguistic red flags versus green flags in health reporting 1517222839.
| 🚩 Red Flag Phrases & Tactics | 🟢 Green Flag Phrases & Tactics | What It Indicates About the Source |
|---|---|---|
| "Miracle cure," "Revolutionary," "Breakthrough," "Game-changing," "Holy Grail" | "Incremental progress," "Preliminary findings," "Contributes to existing knowledge," "Exploratory" | Authentic science is inherently slow, cautious, and cumulative. Sensational adjectives (red flags) indicate marketing, hyperbole, or pure clickbait, whereas measured, caveated language (green flags) reflects actual scientific reality and journalistic integrity 1517. |
| "A new study definitively proves..." or "Science now proves..." | "A new study suggests..." or "Evidence increasingly indicates..." or "Demonstrates a strong association..." | Single, isolated studies never definitively prove broad, complex biological claims. Reliable sources acknowledge the probabilistic nature of research and avoid absolutist declarations 115. |
| "Doubles the risk" or "Cuts risk by 80%" (Stating relative risk in isolation) | "Increases absolute risk from 1% to 2%" alongside relative metrics. | Red flags intentionally hide the baseline probability to maximize fear or hope. Green flags provide necessary context so the reader can gauge the actual, tangible danger or benefit to themselves 152627. |
| "Toxins," "Detox your system," "Chemicals" (Used vaguely without specification) | Specific biochemical agents are named, accompanied by precise dosage context and exposure limits. | The dose makes the poison. Vague, ominous terms like "toxins" are fear-mongering buzzwords predominantly used to sell unregulated supplements or diets, not legitimate scientific terminology 40. |
| "Doctors hate this," "The hidden medical secret," or "What the establishment won't tell you" | "Consult your healthcare provider," "Aligns with current institutional guidelines," "Supported by clinical consensus" | Conspiracy framing is a psychological manipulation tactic used to bypass critical thinking and establish a false "insider" authority, almost exclusively utilized to sell unregulated products or ideologies 1740. |
| Heavy reliance on emotional anecdotes ("It worked for my cousin," "My journey to healing") | Reference to aggregated data, RCTs, statistical significance, and large cohort observations. | Humans are evolutionarily wired to trust compelling narrative stories, but anecdotes are not empirical data. Quality reporting relies on structured, peer-reviewed population data, not isolated personal experiences 2240. |
| No links to primary sources, or "Data available upon request" | Direct hyperlinks to the peer-reviewed study (e.g., DOI numbers, PubMed links, or direct journal references). | If a publisher or influencer cannot be bothered to link to the source material, they likely misread it, never read it at all, or are intentionally obfuscating the original context to prevent verification 1628. |
How Do I Evaluate Health News from Modern Vectors (TikTok, Instagram, and Influencers)?
While traditional print and broadcast journalism have long suffered from sensationalism, the post-2023 digital landscape has violently shifted the epicenter of health misinformation away from newsrooms and directly onto social media platforms. Networks like TikTok and Instagram have fundamentally transformed the delivery of health news from nuanced, text-based articles to highly engaging, parasocial, and algorithmically driven short-form video content 45.
This architectural shift in media consumption has successfully bypassed traditional editorial gatekeepers, elevating charismatic "health influencers" - who overwhelmingly lack formal medical credentials or epidemiological training - to positions of immense, unchecked authority 3. A comprehensive, landmark 2025 study from the University of Sydney, published in JAMA Network Open, analyzed nearly 1,000 Instagram and TikTok posts reaching an audience of almost 200 million followers, revealing staggering systemic issues regarding medical truth online 432. The research focused specifically on the viral promotion of trendy, highly controversial health screenings, such as full-body MRI scans, anti-mullerian hormone (AMH) "egg timer" tests, direct-to-consumer testosterone blood panels, genetic cancer testing, and unverified gut microbiome assessments 432.
The findings of the Sydney study paint a remarkably grim picture of the realities of social media health advice: * 85% of the analyzed posts failed to mention any potential downsides, risks, or financial costs of the medical procedures they aggressively promoted 432. * Only 6% of posts mentioned the severe risk of overdiagnosis or overtreatment. This is a massive, widely recognized issue in preventative medicine, where finding incidental, harmless biological anomalies leads to highly invasive biopsies, unnecessary surgeries, and severe psychological anxiety 432. * 68% of the influencers producing this content had undisclosed or implicit financial conflicts of interest, profiting via sponsorships, affiliate links, or direct sales of the tests they were recommending 432. * Only 6% of the content referenced actual, verifiable scientific evidence, instead relying almost entirely on highly emotional, cherry-picked personal anecdotes to drive their narratives 32.
The profound danger of this specific vector is that it weaponizes the aesthetic of wellness. Influencers often present themselves in peak physical condition, utilizing professional lighting and editing to create a powerful "halo effect" that makes their medical advice seem implicitly credible and aspirational 4032. They peddle expensive, clinically unnecessary interventions to completely healthy individuals under the empowering but misleading guise of "taking control of your own health" 32. For example, the AMH "egg timer" test is heavily marketed to young, healthy women as a definitive measure of fertility, despite clinical consensus that it is unreliable for this purpose outside of specific infertility treatments, driving women toward costly and unnecessary interventions 32.
The mental health space on platforms like TikTok is particularly vulnerable to this phenomenon. A 2025 journalistic investigation by The Guardian into the top 100 videos under the #mentalhealthtips hashtag revealed that more than half of the top trending videos contained blatant, dangerous misinformation 5. Content creators frequently misused complex clinical therapeutic language, offered scientifically unsupported "quick fixes" (such as claiming specific herbal supplements like saffron or magnesium glycinate can instantly cure severe anxiety or heal deep trauma in an hour), and routinely pathologized normal human emotional experiences by falsely labeling them as definitive symptoms of borderline personality disorder, ADHD, or trauma 5.
To safely navigate this modern vector, consumers must adopt an absolute, baseline stance of extreme skepticism toward any health advice encountered on social media. The fundamental algorithmic design of these platforms actively rewards emotional intensity, controversy, and rapid engagement, not clinical accuracy or nuance 3343. A 2024 study published in Otolaryngology - Head and Neck Surgery examining sinusitis information on TikTok found that nearly 60% of videos produced by nonmedical influencers contained non-factual information, compared to only 15% of videos from actual medical professionals 3. However, because the algorithm heavily favors entertaining, simplified content over dry, caveated medical facts, the misinformation generated by non-experts achieved vastly more views and visibility 3.
Recognizing that misinformation travels faster than evidence, public health entities are beginning to fight back. Initiatives like the Harvard T.H. Chan School of Public Health's Creator Program, led by Amanda Yarnell, actively partner with social media creators to help them counter health misinformation and spread evidence-based science 33. These programs teach creators to use built-in platform tools, such as TikTok's "Stitch" feature, to execute "prebunking" and "debunking" strategies - briefly showing the misinformation and immediately explaining why it is scientifically flawed in an engaging format 33344. Nonetheless, when consuming health content on these platforms, the end-user must aggressively verify the creator's clinical credentials and immediately distrust any content accompanied by a discount code, affiliate link, or monetization strategy.
What is the Impact of AI-Generated Content on Health Misinformation?
If social media algorithms structurally prioritize emotional engagement over objective truth, the rapid advent of Generative Artificial Intelligence (GenAI) and Large Language Models (LLMs) such as ChatGPT, Claude, and Google Gemini has introduced an entirely new, highly sophisticated paradigm of risk: the industrial-scale automation of plausible falsehoods 61213.
Historically, identifying medical misinformation was somewhat aided by obvious, human-level markers: poor grammar, aggressive formatting, highly emotional language, or obvious spelling errors. Generative AI entirely eliminates these tells. LLMs are explicitly engineered to predict the most statistically probable next word in a sequence based on vast internet scraping, allowing them to produce text with absolute grammatical perfection and a highly authoritative, academic tone 1344. This creates a dangerous psychological phenomenon known as "false fluency" 12. Users read a well-structured, impeccably formatted paragraph and subconsciously equate its linguistic competence with factual accuracy, dropping their critical guard 1213. Controlled empirical studies have terrifyingly demonstrated that AI-generated health disinformation is often rated by users as harder to identify and more persuasive than human-authored fake news 12.
The epistemic reality, however, is that LLMs are not truth-seeking engines; they are, in essence, "statistical parrots" 13. They entirely lack factual grounding, do not possess medical reasoning, and cannot understand contextual clinical risks 13. This architectural limitation leads to the critical danger of "AI hallucinations," where the model confidently invents facts, biological mechanisms, statistics, and even entirely fabricated academic citations 3435. For instance, if a user asks a chatbot to summarize the benefits of a niche, unproven supplement, the AI might generate a highly convincing summary of a clinical trial that never actually took place, complete with fake authors, fabricated p-values, and a non-existent publication journal 4435.
A 2025 study conducted by researchers at the Icahn School of Medicine at Mount Sinai demonstrated this specific vulnerability explicitly. Researchers fed popular AI chatbots fictional patient scenarios containing made-up diseases, fabricated symptoms, and fake medical tests 34. Without specific prompt engineering to force the AI to verify facts, the chatbots blindly accepted the fake medical details, elaborated on them, and confidently generated complex explanations and treatment plans for diseases that literally do not exist in medical science 34. The study highlighted that while adding simple warning prompts reduced these hallucinations, current AI systems remain highly vulnerable to expanding upon false premises 34.
Furthermore, the sheer scale at which AI can generate disinformation is entirely unprecedented. A single bad actor, utilizing automation, can use an LLM to generate thousands of medically plausible but entirely false articles, synthetic social media posts, and fake expert testimonies attributed to non-existent doctors in a matter of minutes, completely flooding the information ecosystem 61244. This threat is particularly acute in low- and middle-income countries (LMICs), where overburdened health systems and limited digital literacy result in populations treating AI models as de facto triage systems and primary medical advisors, creating a dangerous "generative illusion" of authority 13.
Conversely, AI is also being leveraged as a powerful tool for public health. In 2025, researchers at the Annenberg School for Communication developed an automated AI system capable of creating effective, evidence-based public health social media campaigns in real time, drastically outperforming traditional unscientific campaigns by analyzing vast datasets to find messages that truly resonate with specific communities 36. Search engines and digital platforms are also attempting to mitigate AI risks by adjusting their algorithms to heavily weigh E-E-A-T signals (Experience, Expertise, Authoritativeness, and Trustworthiness) 4348. In an AI-mediated search environment, content that lacks institutional backing or transparent medical authorship is theoretically suppressed in favor of established medical consensus, shifting the battleground from social virality to engineered authority 4348.
When using AI for health information, consumers must adapt their behavior. AI outputs must be treated strictly as a starting point for vocabulary and concept mapping, never as diagnostic or clinical truth 35. The most vital skill in the AI era is the manual verification of AI-generated claims. If an AI provides a source or a statistic, the user must independently search PubMed, Google Scholar, or a verified institutional database to ensure the study actually exists and that its conclusions precisely match the AI's summary 23549.
How Do Global Public Health Standards Combat Misinformation?
To systematically counteract the relentless deluge of sensationalized journalism, financially motivated influencer marketing, and AI-generated hallucinations, global public health institutions, academic networks, and international journalism watchdogs have developed rigorous frameworks designed to enforce standards in medical communication 373839.
One of the most successful and widely emulated international models is the "Behind the Headlines" initiative pioneered by the United Kingdom's National Health Service (NHS) 244041. This framework operates as a rapid-response critical appraisal service for the public. When a sensational health story hits the mainstream press - such as a claim that a vegetarian diet causes infertility or that afternoon heart surgery is safer - clinical analysts at the NHS trace the story back to its original peer-reviewed source 24424358. They apply a strict methodological checklist, asking foundational questions: Did the study use valid methods? Are the results clinically important, or just statistically significant? Are the results applicable to the general population? 24 They assess the study design, evaluate the sample size, analyze whether the researchers adequately controlled for confounding variables, and check if the absolute risk was reported alongside the sensational relative risk 244358. The NHS then publishes a plain-language summary that strips away the media hype, explaining exactly what the science actually says, what it doesn't say, and whether the headline is justified 4143.
Similarly, the Media Doctor initiative, originating in Australia and subsequently adapted globally in countries like Canada and the USA (as HealthNewsReview.org), established a rigorous 10-point rating instrument to grade the quality of mainstream health journalism 294445. The instrument evaluates whether news articles accurately report the novelty of an intervention, explicitly quantify the absolute benefits, describe potential biological harms, disclose the financial costs, and consult independent medical experts who were not involved in the original study (to avoid the blind regurgitation of biased university press releases) 72930. Historical data compiled from Media Doctor reviews revealed that news outlets frequently failed these basic criteria; while print media performed slightly better than online media, overall reporting was poor, particularly in its consistent failure to discuss the potential harms and costs of new treatments 1730. To address this, researchers have developed multicomponent training interventions for journalists, specifically focusing on educating them about diagnostic tests, the dangers of overdiagnosis, and the interpretation of medical statistics 4647.
Regionally focused efforts are also expanding globally. In Central and Eastern Europe, the SCIENCE+ platform was launched to create a cross-border coalition of medical experts, science editors, and independent media outlets to ensure trustworthy reporting on public health, recognizing that diseases and misinformation do not respect national borders 39. In the Asia-Pacific region, organizations like the Lymphoma Coalition and the Association of Southeast Asian Nations (ASEAN) are integrating media and information literacy directly into educational curricula, equipping students and educators with toolkits to critically assess digital information and counter disinformation 63.
The World Health Organization (WHO) has elevated this concept to a systemic, global level, framing health literacy not merely as an isolated individual responsibility, but as a critical socio-ecological imperative inextricably linked to the United Nations Sustainable Development Goals (SDGs) 101448. The WHO argues that combating misinformation requires the active regulation of the information environment itself 1011. This involves a multi-sectoral approach: training journalists to understand biostatistics 46, enforcing Culturally and Linguistically Appropriate Services (CLAS) standards in the US so diverse populations can access accurate data 3865, and building public-private partnerships to ensure that search engines elevate high E-E-A-T sources above viral, low-quality content 4348. The WHO recognizes that improving health literacy can reduce poverty, enhance educational outcomes, and decrease global health inequities 1048. Organizations like the European Food Information Council (EUFIC) further support this global mandate by producing evidence-based, visually accessible infographics that clearly differentiate between complex concepts like correlation and causation, and absolute versus relative risk, thereby directly attacking the root causes of public confusion in an easily digestible format 2849.
The "BS-Detector" Checklist: Instant Application
Given the highly complex web of cognitive biases, algorithmic manipulation, and frequently poor reporting standards, modern news consumers must internalize a systematic method for evaluating health claims. Below is a practical, instant-application "BS-Detector" checklist designed to be applied immediately to any news article, TikTok video, or AI-generated output.
| Analytical Phase | Specific Questions to Ask | The Scientific Rationale |
|---|---|---|
| 1. Trace the Provenance | Is the primary source cited and hyperlinked? Who funded the research? Is the source E-E-A-T compliant? |
If a publisher or influencer provides no link to the peer-reviewed journal, the claim cannot be verified and must be dismissed 1628. Funding sources (e.g., a pharmaceutical company funding a drug trial) introduce massive conflicts of interest 258. Look for institutional authority (.gov, .edu) rather than lifestyle influencers 223248. |
| 2. Audit the Methodology | Was the study conducted on a human or a mouse? Was it an observational study or an RCT? How large was the sample size? |
Animal studies do not predict human outcomes; they are preliminary 2028. Observational studies show correlation, not causation, and are vulnerable to confounding variables 272958. A study of 12 people is an anecdote; a study of 12,000 is robust data 229. |
| 3. Interrogate the Mathematics | Does the headline only report relative risk (e.g., "Doubles the risk")? What is the absolute baseline risk? Are the visual graphs manipulated? |
Never accept a relative risk without demanding the absolute baseline. A 100% relative increase on a 0.001% absolute chance is still only a 0.002% risk 2634. Ensure Y-axes on graphs start at zero and are not truncated to exaggerate minor changes 28. |
| 4. Assess the Narrative Framing | Is the language highly emotional or sensationalized? Does it claim to overturn all established consensus overnight? |
Genuine scientific writing is dry, measured, and heavily caveated. Words like "Miracle" or "Toxic" are massive red flags for marketing manipulation 1517. Science moves by aggregate consensus, not single outlier studies 12. |
| 5. Verify the Artificial Intelligence | Did I manually verify the citation? Is the AI offering a diagnosis? |
AI models suffer from "hallucinations" and will confidently invent fake studies and authors 3435. Always copy the provided citation and verify it exists in Google Scholar or PubMed 3549. Never use AI to alter a prescribed medical treatment 35. |
Bottom Line
Health whiplash is an artificial construct generated by a digital media ecosystem that fundamentally prioritizes engagement, velocity, and emotion over clinical nuance and accuracy. The scientific method is not failing when health advice updates; it is working exactly as intended by correcting itself through iteration. By firmly grounding your understanding in the hierarchy of evidence, aggressively seeking absolute risk metrics over relative fear-mongering, and applying critical friction to the claims made by social media influencers and generative AI, you can successfully inoculate yourself against medical misinformation. The ultimate defense against bad science is not memorizing every biological fact, but mastering the rules of evidence.