Cortisol research and social media health claims
The intersection of clinical endocrinology and digital wellness culture has generated unprecedented public interest in cortisol, an essential glucocorticoid hormone synthesized by the adrenal glands. Across global social media platforms, an extensive narrative has emerged characterizing cortisol as a universal antagonist to human health. This discourse systematically links the hormone to weight gain, chronic fatigue, metabolic dysfunction, and facial edema. Consequently, this narrative has catalyzed a multi-trillion-dollar consumer market prioritizing cortisol-lowering supplements, specialized functional beverages, and highly specific exercise regimens. However, clinical endocrinology presents a vastly different biological paradigm. In physiological reality, cortisol is a critical survival hormone that regulates basal metabolism, modulates systemic immune responses, and manages cardiovascular homeostasis. The profound discrepancy between the biological necessity of cortisol and its vilification in digital wellness spaces highlights a broader phenomenon of digital medical misinformation, the systemic oversimplification of the hypothalamic-pituitary-adrenal axis, and the complex psychological impacts of algorithmic health content on the modern consumer.
Endocrinology of the Hypothalamic-Pituitary-Adrenal Axis
To comprehend the divergence between clinical science and digital wellness trends, it is necessary to establish the biochemical and physiological realities of cortisol. Cortisol is the primary glucocorticoid hormone secreted by the cortex of the adrenal gland 1. Biochemically, cortisol is a steroid hormone derived from cholesterol. Its chemical structure features a basic pregnenolone hydrocarbon ring wherein three carbon atoms are replaced by hydroxyl groups at the 11, 17, and 21 positions. The hydroxyl group at the C-11 atom resides in the beta position, while the C-17 hydroxyl group is in the alpha position, accompanied by two ketone groups at the C-3 and C-20 atoms 1. This specific structural configuration allows cortisol to bind effectively to glucocorticoid receptors present in almost every tissue in the human body.
The Neuroendocrine Feedback Loop
Cortisol secretion is strictly governed by the hypothalamic-pituitary-adrenal (HPA) axis, a highly sensitive neuroendocrine feedback loop. The hypothalamus, an almond-sized region located at the base of the brain, acts as the central monitoring station. When the hypothalamus detects homeostatic deviations - whether induced by physical exertion, psychological stress, inflammatory markers, or the natural circadian rhythm - it secretes corticotropin-releasing hormone (CRH) 234.
CRH travels via the hypophyseal portal system to the anterior pituitary gland, which serves as the metabolic accelerator. The pituitary responds by synthesizing and releasing adrenocorticotropic hormone (ACTH) into the systemic circulation. ACTH ultimately reaches the adrenal cortex, prompting the immediate synthesis and secretion of cortisol 35.
Once circulating in the bloodstream, cortisol executes numerous critical physiological processes necessary for survival. In the liver, cortisol facilitates gluconeogenesis, ensuring a continuous and steady supply of glucose to the brain and peripheral tissues 6. Within the immune system, it acts as a potent anti-inflammatory agent, keeping immune responses in check to prevent autoimmune hyperactivity and systemic tissue damage 67. Cortisol also plays a regulatory role in maintaining blood pressure, modulating lipid and protein metabolism, and synchronizing the sleep-wake cycle 678. The biological imperative of cortisol is so absolute that conditions characterized by extreme hypocortisolism, such as Addison's disease, present a risk of fatal adrenal crisis requiring immediate and lifelong glucocorticoid replacement therapy 91011.
Circadian Rhythms and Diurnal Cortisol Secretion
Cortisol is not secreted at a static rate; rather, its production is characterized by a highly predictable diurnal rhythm dictated by the body's central circadian pacemaker 112. Understanding this rhythm is critical for interpreting physiological health, as deviations from the standard curve frequently indicate underlying metabolic or psychological disruptions.
The Cortisol Awakening Response
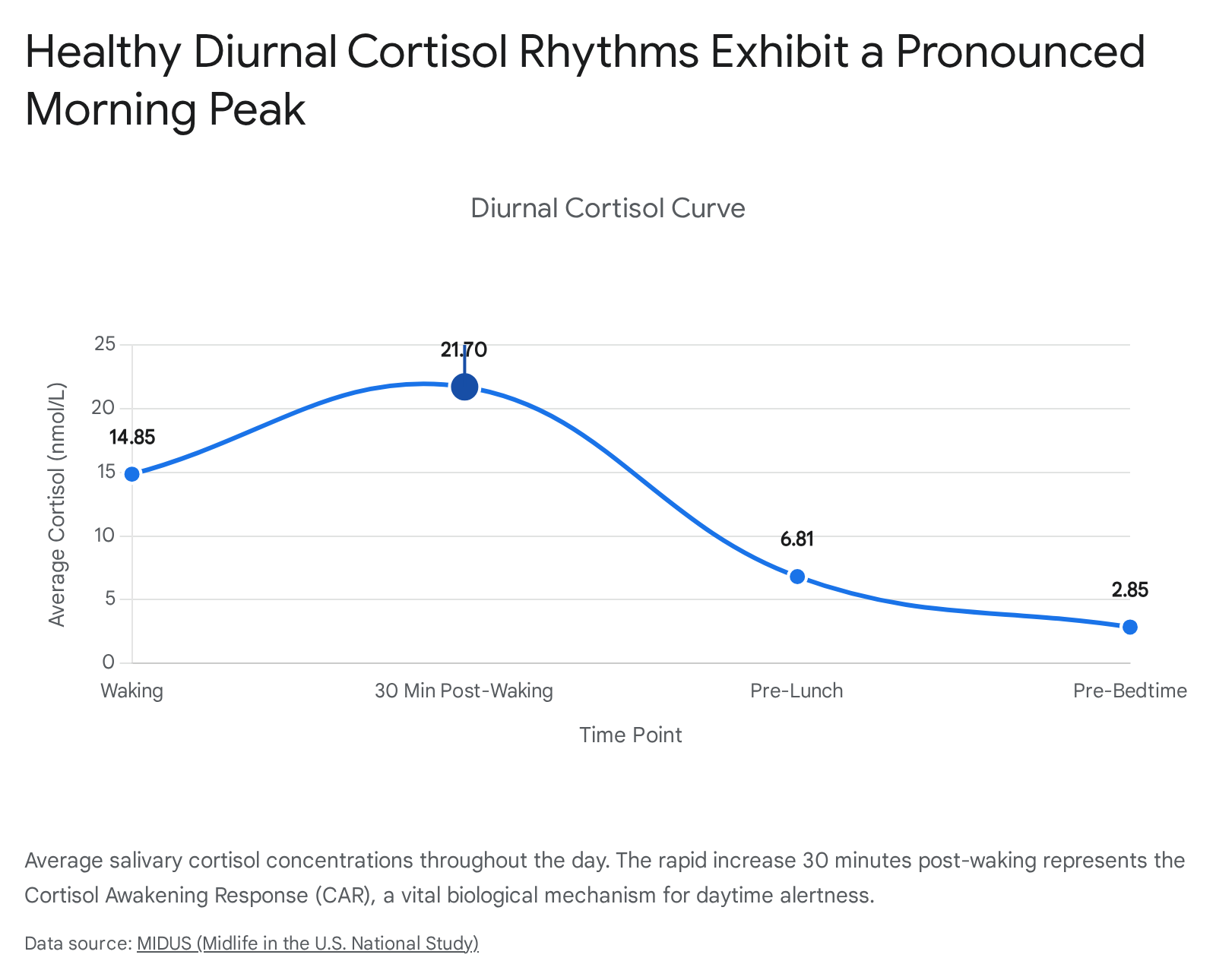
In healthy populations, cortisol concentrations reach their absolute nadir near midnight, a biological necessity that permits the secretion of melatonin and the initiation of restorative sleep phases 12. During the final hours of the nocturnal sleep cycle, the HPA axis begins to upregulate cortisol production. This culmination results in the Cortisol Awakening Response (CAR), a sharp and rapid increase in cortisol secretion that peaks approximately 30 to 45 minutes after awakening 1213.
The CAR is not a symptom of morning stress, but rather an evolutionary adaptation designed to elevate blood pressure, mobilize blood glucose, and stimulate the central nervous system to safely transition the human body from a dormant state to active wakefulness 614. Researchers observing adults across multi-day trials have identified that a robust CAR - characterized by a steep upward slope immediately upon waking followed by a rapid, steady decline - is the hallmark of a healthy, normative endocrine profile. Conversely, a flattened diurnal slope with a blunted CAR is highly correlated with older age, chronic health conditions, male sex, and the use of confounding medications 13.
Following the morning peak, cortisol concentrations engage in a slow, steady clearance throughout the diurnal period. The lowest physiological levels are consistently observed prior to bedtime 1516. Health professionals evaluate these rhythms utilizing a diurnal cortisol curve, frequently mapped through four distinct salivary samples taken at waking, midday, evening, and night 1215.
The analytical distinction between serum and salivary cortisol levels is highly relevant to clinical diagnostics. Serum cortisol represents the total circulating hormone, which is predominantly bound to carrier proteins and heavily concentrated, whereas salivary cortisol represents the free, biologically active fraction 112. Salivary assessment is favored for diurnal tracking due to its non-invasive nature, mitigating the risk of venipuncture-induced stress artifacts.
| Collection Period | Average Serum Concentration (nmol/L) | Average Salivary Concentration (nmol/L) | Physiological State |
|---|---|---|---|
| Morning (8:00 - 9:00 a.m.) | 459.6 ± 235.2 | 21.2 ± 16.2 | Post-awakening metabolic surge; maximal HPA axis output 117. |
| Afternoon (4:00 - 5:00 p.m.) | 340.5 ± 207.5 | 12.7 ± 8.1 | Gradual hepatic clearance; declining sympathetic tone 1. |
| Midnight (11:00 p.m. - 12:00 a.m.) | Data Sparse | < 3.5 | Baseline nadir; suppression of ACTH allowing melatonin dominance 1218. |
(Clinical diagnostic parameters indicate that morning serum cortisol is approximately twenty times higher than corresponding salivary concentrations, underscoring the vast proportion of protein-bound hormone in the bloodstream 1.)
Photic Regulation of the HPA Axis
The diurnal cortisol rhythm is fundamentally anchored to environmental cues, primarily light exposure. The suprachiasmatic nucleus (SCN) of the hypothalamus serves as the body's master chronobiological clock, processing photic information received directly from the retina 19.
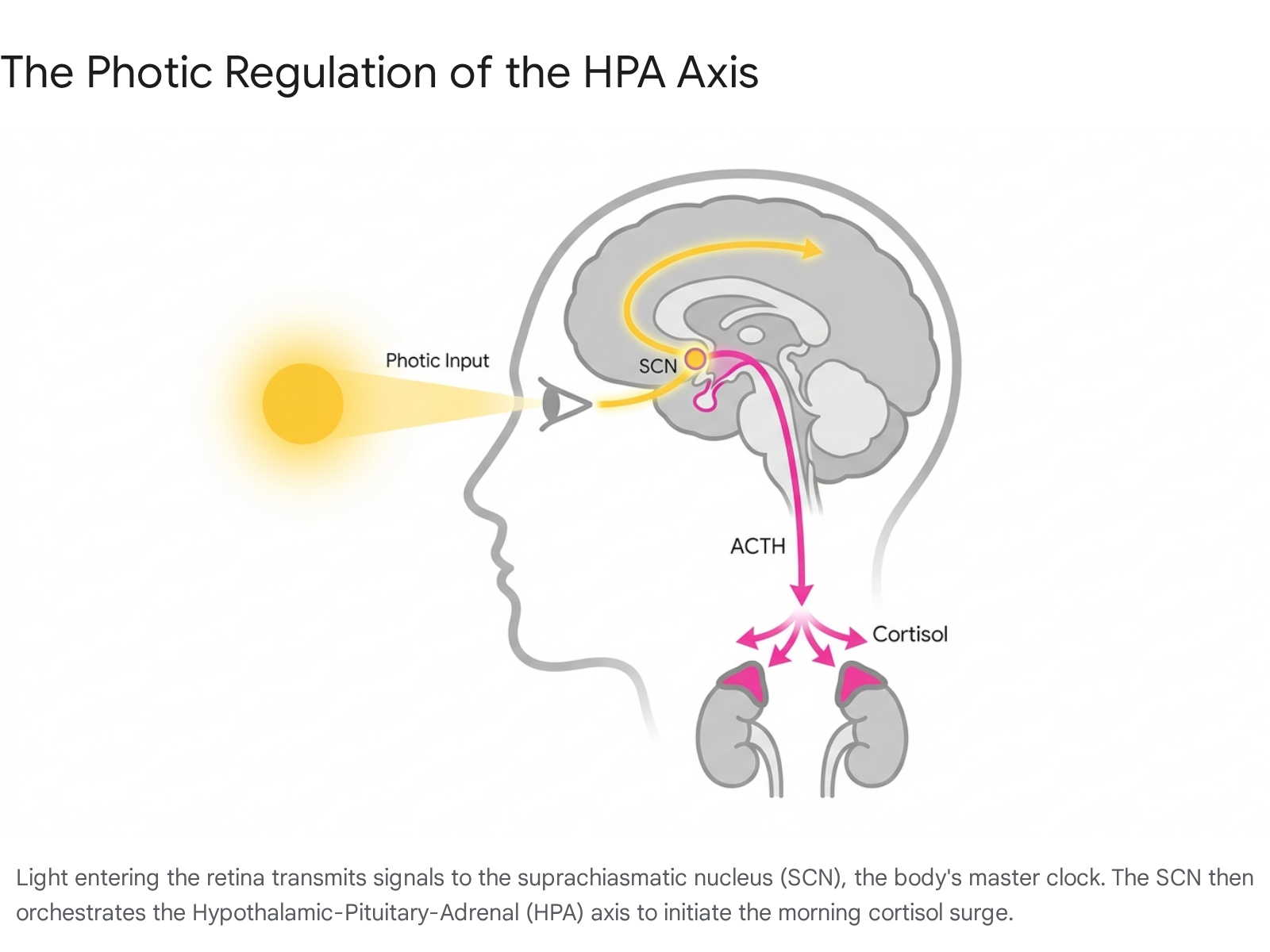
The timing, spectrum, and intensity of light exposure exert profound modulatory effects on adrenal function.
Clinical research utilizing controlled laboratory environments demonstrates that early morning exposure to bright light (ranging between 2,500 and 10,000 lux) significantly amplifies the Cortisol Awakening Response 1920. Specifically, individuals exposed to bright, white or short-wavelength blue light (470-nm) within the first two to three hours of waking experience a 20% to 50% greater peak in salivary cortisol compared to subjects remaining in dim lighting (less than 150 lux) 202122.
In the context of the wellness paradigm, which frequently treats any cortisol elevation as pathological, chronobiologists view this photic enhancement as highly therapeutic. A robust CAR driven by morning light optimizes daily stress hormone patterns, improves daytime vigilance, and supports psychological resilience against daily stressors 20. The acute suppressive effects of bright light on cortisol are primarily observed during the biological night; exposure to 10,000 lux during descending cortisol phases rapidly diminishes plasma concentrations, underscoring the SCN's ability to acutely override the adrenal glands 19. Furthermore, early wake times combined with light exposure naturally restrict the nocturnal suppression of melatonin, liberating cortisol to rise sequentially during the sleep-wake transition 6.
Pathological Hypercortisolism Versus Lifestyle Edema
The most highly visible manifestation of cortisol misinformation on social media relates to physical appearance, specifically the viral phenomenon dubbed "cortisol face." Digital content creators routinely attribute round, puffy, or bloated facial appearances to chronic occupational or emotional stress, advocating for behavioral interventions to achieve a slimmer jawline 2324.
Clinical Moon Facies
In medical taxonomy, a distinctly round and swollen face is classified as "moon facies," a strictly clinical symptom associated with profound, chronic hypercortisolism 2325. Moon facies is driven by extreme, systemic cortisol overload that fundamentally alters lipid metabolism, causing adipose tissue to aggressively redistribute from the extremities to the face, the suboccipital region (creating a "buffalo hump"), and the visceral abdomen 2526.
This degree of hypercortisolism is nearly impossible to induce through psychosocial stress alone. Instead, clinical moon facies is predominantly caused by two explicit medical conditions: 1. Exogenous Corticosteroid Administration: The long-term prescription of potent synthetic glucocorticoids (such as prednisone or dexamethasone) for the management of asthma, rheumatoid arthritis, or other severe autoimmune disorders 232527. 2. Cushing's Syndrome/Disease: A rare endogenous endocrine disorder with an incidence rate of 10 to 15 cases per million people annually 26. This condition is universally driven by cortisol-secreting adrenal tumors or ACTH-secreting pituitary adenomas 2329.
The diagnostic pathway for suspected Cushing's syndrome is rigorous, relying on midnight salivary cortisol assays (where levels exceeding 4.0 nmol/L suggest pathology), 24-hour urinary free cortisol testing, dexamethasone suppression tests, and advanced MRI imaging 1226. Furthermore, true hypercortisolism presents alongside severe systemic symptoms including profound muscle wasting in the limbs, cutaneous striae (dark stretch marks), treatment-resistant hypertension, and severe metabolic syndrome 2326.
Drivers of Non-Endocrine Facial Puffiness
For the general population experiencing episodic facial fullness, the underlying etiology is rarely endocrine failure. Everyday emotional stress is insufficient to drive the structural fat redistribution seen in true moon facies 2327. Consequently, "cortisol face" is not a recognized medical diagnosis but rather a social media colloquialism that conflates transient fluid retention with complex endocrine pathology 2324.
Facial edema observed in the general public is predominantly driven by lifestyle and dietary factors that may correlate with periods of stress, but operate via entirely independent physiological mechanisms: * Dietary Sodium Exertion: Psychological stress frequently precipitates cravings for highly palatable, sodium-dense foods. Elevated sodium intake directly induces systemic cellular water retention, which preferentially manifests in the facial tissues due to localized vascular dynamics 232427. * Sleep Deprivation and Lymphatic Stasis: Inadequate sleep disrupts fluid homeostasis and impairs overnight lymphatic drainage. Sleeping position, particularly prone or lateral resting, exacerbates fluid pooling in the face upon waking 830. * Allergens and Histamine Responses: Unrecognized seasonal allergies or low-grade sinus infections trigger histamine releases, leading to localized inflammation, vasodilation, and under-eye puffiness 824. * Alternative Endocrine Disruptions: Chronic, pervasive facial puffiness is frequently a symptom of untreated hypothyroidism (resulting in facial myxedema) or Polycystic Ovary Syndrome (PCOS), neither of which are primarily driven by cortisol overproduction 232531.
Endocrinologists maintain that advising patients to arbitrarily "lower cortisol" based on facial appearance is medically unsound. Diagnostic clarity demands distinguishing between idiopathic lifestyle edema and true endocrine disruption 1126.
Evolution of Clinical Terminology in Wellness Spaces
A significant mechanism perpetuating digital health misinformation is the co-optation of clinical terminology by the alternative wellness sector. For decades, holistic practitioners utilized the term "adrenal fatigue" to describe an exhaustion syndrome theorized to arise from the adrenal glands' inability to synthesize cortisol following prolonged psychosocial stress 239.
The Diagnostic Invalidation of Adrenal Fatigue
Rigorous scientific review has universally failed to substantiate the existence of adrenal fatigue. The adrenal glands do not succumb to functional exhaustion or deplete their biosynthetic capacity simply due to modern lifestyle stressors 31128. Except in autoimmune contexts resulting in Addison's disease - where the adrenal cortex is physically destroyed - the glands remain highly capable of synthesizing glucocorticoids indefinitely 911.
Patients presenting with profound fatigue and identifying with the adrenal fatigue label frequently exhibit normal or even elevated total cortisol production when measured via comprehensive 24-hour urinary breakdown products, despite occasional low free salivary cortisol at specific time points 3. Consequently, treating these patients with exogenous cortisol supplements based on unvalidated symptom questionnaires has led to iatrogenic (medication-induced) Cushing's syndrome and permanent, life-threatening suppression of the endogenous adrenal glands 11.
The Shift to HPA Axis Dysregulation
In response to the scientific invalidation of adrenal fatigue, evidence-based integrative medicine has adopted the precise terminology of "Hypothalamic-Pituitary-Adrenal (HPA) Axis Dysregulation" or "Maladaptation" 3929.
This updated framework correctly identifies the central nervous system - specifically the hypothalamus - as the locus of dysfunction 29. Chronic exposure to inflammation, emotional trauma, environmental toxins, and disrupted circadian rhythms initiates a protective cascade in the brain 229. To shield peripheral tissues from the catabolic damage of relentless cortisol exposure, the hypothalamus actively down-regulates its signaling, reducing the secretion of CRH and ACTH 29. The resultant low cortisol levels observed in conditions such as Chronic Fatigue Syndrome, fibromyalgia, and severe burnout are a secondary consequence of central brain down-regulation, not primary adrenal failure 29.
Despite this critical distinction in medical pathology, social media platforms continue to heavily monetize the concept of "healing the adrenals," demonstrating a significant lag between scientific consensus and public health discourse 111428.
Nutritional Interventions and Supplement Efficacy
The belief in epidemic-level hypercortisolism has birthed an expansive market for consumer interventions, most notably in the form of specific beverage formulations and botanical adaptogens. Evaluating the biochemical validity of these trends reveals a spectrum ranging from beneficial baseline nutrition to highly exaggerated physiological claims.
The Cortisol Cocktail Phenomenon
A predominant trend across platforms like TikTok is the "cortisol cocktail" or "adrenal mocktail." While formulations vary slightly, the standard recipe combines orange or lemon juice (providing Vitamin C and fast-acting glucose), coconut water (providing potassium), sea salt (for sodium replenishment), and magnesium powder 73031. Promoters of the beverage claim that this exact combination rapidly lowers stress hormones, resets the adrenal glands, and directly treats burnout 303132.
Biochemically, the individual components of the mocktail do support general cellular function. The adrenal glands possess one of the highest concentrations of Vitamin C in the human body, utilizing it rapidly during the synthesis of both catecholamines and glucocorticoids 33. Magnesium acts as a crucial cofactor in hundreds of enzymatic reactions, modulating central nervous system excitability; furthermore, chronic stress accelerates the renal excretion of magnesium stores 33. Potassium is vital for maintaining intracellular fluid balance, while dietary sodium can temporarily alleviate the lightheadedness often associated with prolonged sympathetic activation 3132.
However, the assertion that combining these nutrients yields an acute, significant reduction in circulating cortisol levels lacks any empirical scientific foundation 303233. Clinical dietitians note that these micronutrients are easily obtained in sufficient quantities through a standard, diverse diet 32. More importantly, the frequent consumption of the cortisol cocktail presents distinct metabolic risks. The rapid influx of simple sugars from concentrated citrus juice exacerbates blood glucose volatility, placing undue stress on pancreatic insulin response in metabolically vulnerable populations 3034. Additionally, the deliberate administration of sodium poses cardiovascular risks for individuals managing essential hypertension 3034. The subjective improvements in energy reported by consumers are largely attributed to simple hydration and glycemic elevation rather than definitive HPA axis modulation 3135.
The Clinical Efficacy of Botanical Adaptogens
Beyond beverage formulations, the market for adaptogenic supplements - botanicals historically utilized in traditional medicine to enhance stress resilience - has surged. The most prominent compounds targeted for cortisol reduction include Ashwagandha (Withania somnifera), Rhodiola (Rhodiola rosea), and L-theanine (derived from green tea) 363738. While often marketed interchangeably, clinical data reveals distinct mechanisms and varying degrees of efficacy among these substances.
| Botanical Compound | Active Mechanism / Physiological Target | Empirical Cortisol Reduction Data | Clinical Considerations |
|---|---|---|---|
| Ashwagandha | Neuromodulation of the HPA axis; suppression of pro-inflammatory cytokines 3739. | High Efficacy: Systematic reviews pool trials demonstrating 11% to 33% reductions in baseline cortisol over 30 - 112 days at doses of 240 - 600 mg/day 39. | Unestablished long-term safety data; potential interactions with autoimmune and endocrine medications 3940. |
| Rhodiola rosea | Central nervous system stimulation; modulation of neuro-motoric and cognitive fatigue pathways 3741. | Mixed Efficacy: Highly effective at reducing subjective fatigue and burnout scores, but primary trial endpoints frequently show inconclusive direct effects on quantitative salivary cortisol suppression 3941. | Approved by the European Medicines Agency for temporary relief of stress symptoms; highly tolerated, but acts primarily on cognitive resilience rather than cortisol suppression 3741. |
| L-Theanine | Promotion of alpha brain-wave activity; antagonism of excitatory neurotransmitters 3638. | Moderate/Acute Efficacy: Measurable suppression of salivary cortisol observed 3 hours post-ingestion during acute stress tasks; limited data on chronic basal reduction 38. | Operates synergistically with other compounds; effectively mitigates the physiological spike associated with immediate stressors rather than systemic hypercortisolism 3638. |
Despite the promising data surrounding Ashwagandha, indiscriminate supplementation is physiologically hazardous. Individuals suffering from late-stage HPA axis dysregulation - characterized by a flattened diurnal curve and "cortisol flatlining" - already exhibit abnormally low cortisol levels 40. Administering a potent cortisol-lowering botanical in this state further suppresses the necessary morning CAR, directly exacerbating systemic fatigue and lethargy 40.
Exercise Modalities and Adrenal Responses
Exercise physiology represents another domain heavily influenced by cortisol-related wellness narratives. A prevailing trend on social media cautions against High-Intensity Interval Training (HIIT) and sustained distance running, claiming these activities chronically elevate cortisol, resulting in intractable abdominal adiposity ("cortisol belly") 642. As a result, many consumers have shifted exclusively toward Low-Intensity Steady State (LISS) cardio, such as incline walking or Pilates 4247.
The Hormonal Dynamics of High-Intensity Interval Training
The assertion that HIIT causes pathological hypercortisolism fundamentally misinterprets the nature of exercise endocrinology. Physical exertion serves as an acute, essential physiological stressor. During high-intensity training (operating at 85% to 95% of maximum heart rate), the hypothalamus rapidly activates the sympathetic nervous system and the HPA axis. This triggers an immediate, pronounced spike in cortisol, alongside parallel surges in anabolic hormones such as testosterone and human growth hormone (GH) 4843.
This cortisol spike is biologically necessary; it catalyzes glycogenolysis and lipolysis, rapidly mobilizing stored glucose and fatty acids to meet the extreme energetic demands of the muscle tissues 4243. Unlike psychological stress, exercise-induced cortisol elevation is transient. Research demonstrates that upon cessation of intense exercise, a robust negative feedback loop initiates, generally returning serum cortisol to baseline resting levels within 90 minutes 42.
Furthermore, the metabolic superiority of HIIT in specific contexts relies on this intense hormonal disruption. The severe homeostatic challenge induces Excess Post-exercise Oxygen Consumption (EPOC). Clinical trials monitoring energy expenditure reveal that while a moderate 30-minute jog burns approximately 288 kcal, equivalent sprint intervals burn up to 562 kcal. Crucially, the afterburn effect of HIIT keeps the basal metabolic rate elevated for up to 24 hours as the body synthesizes proteins and replenishes glycogen 48.
The Utility of Low-Intensity Steady State Cardio
While the acute cortisol spike of HIIT is physiologically healthy, its frequent application without adequate recovery can lead to systemic overtraining. If high-intensity regimens are layered atop pre-existing chronic occupational stress and sleep deprivation, the continuous activation of the HPA axis can contribute to chronic basal elevation and subsequent reproductive hormone suppression 47.
In contrast, LISS cardio (operating at 50% to 65% of maximum heart rate) provides cardiovascular benefits without crossing the physiological threshold required to significantly activate the adrenal glands 4248. Activities like steady cycling or walking maintain steady blood glucose levels without the delayed spikes associated with hepatic glucose dumping in HIIT 44. For individuals currently presenting with profound HPA axis dysregulation or those seeking active recovery between intense training sessions, LISS offers a highly effective mechanism to engage the parasympathetic nervous system, lowering overall allostatic load while still achieving meaningful fat oxidation 4744. Ultimately, both modalities are essential components of physical health, and the vilification of high-intensity exercise based on transient cortisol spikes is scientifically unfounded 642.
Fasting Protocols and Circadian Hormone Shifts
The physiological impact of dietary timing on the HPA axis has garnered significant attention, particularly concerning intermittent fasting, Time-Restricted Eating (TRE), and religious fasting protocols like Ramadan. Fasting serves as a profound metabolic stressor, directly influencing the amplitude and chronobiology of cortisol secretion.
Clinical trials monitoring salivary and serum cortisol during sustained fasting reveal complex circadian shifts. In strict multi-day fasting scenarios, plasma cortisol levels elevate dramatically, shifting the circadian peak from the morning to the early afternoon 45. Even short-term interventions, such as an early 8:00 AM to 2:00 PM feeding window, reliably increase fasting morning serum cortisol levels 45.
Research assessing continuous 64-hour salivary sampling during acute fasting protocols underscores distinct gender-based chronobiological responses. In female cohorts, acute one-day fasting results in a 12% to 13% increase in cortisol amplitude and shifts the acrophase (the timing of the peak concentration) significantly earlier by approximately 48 to 66 minutes 4.
| Fasting Protocol | Impact on Diurnal Cortisol Parameters | Clinical and Metabolic Implications |
|---|---|---|
| Prolonged Fasting (2.5 - 6 Days) | Dramatic elevation of basal plasma cortisol; peak shifts from morning to afternoon 45. | Sustained HPA axis activation; potential for muscle catabolism alongside deep lipolysis 45. |
| Dinner-Skipping (Early TRE) | Reduced evening cortisol concentrations; potential elevation of morning peak 4647. | Aligns with natural circadian clearance; generally supports improved nocturnal metabolic markers 47. |
| Breakfast-Skipping (Late TRE) | Significant reduction or blunting of the morning Cortisol Awakening Response 47. | Potential indicator of HPA axis dysregulation; associated with unfavorable cardio-metabolic outcomes 47. |
| Ramadan Fasting | Abolition of standard circadian rhythmicity; lower morning cortisol coupled with elevated evening concentrations 4647. | Circadian disruption heavily influenced by inverted sleep schedules, nocturnal light exposure, and altered feeding times 47. |
These findings highlight that fasting is not a hormonally neutral intervention. While intermittent fasting yields undeniable improvements in insulin sensitivity, lipid profiles, and cardiovascular metrics, its inherent activation of the stress response suggests that extreme fasting protocols should be carefully calibrated for individuals already exhibiting signs of cortisol dysregulation 445.
Digital Technology Use and HPA Axis Activation
While nutritional and botanical interventions dominate wellness discussions, cyberpsychology research indicates that modern behavioral patterns - specifically digital technology utilization - are profound drivers of systemic cortisol elevation. The integration of smartphones into sleep and waking routines acts as an omnipresent psychosocial stressor.
Neurological Wake States and Smartphone Disruption
The human brain transitions through distinct electrical states during the waking process. It moves from restorative delta waves (deep sleep) into theta waves (dreaming/light sleep), progresses through alpha waves (relaxed, non-processing wakefulness), and finally achieves beta waves (high-frequency alertness) 48.
When individuals immediately engage with smartphones upon waking, they circumvent the vital alpha state, thrusting the brain violently from delta or theta states directly into high-stimulus beta processing 48. This abrupt cognitive loading initiates an immediate stress response. Clinical studies measuring salivary cortisol in subjects using smartphones immediately upon waking reveal a pathologically augmented Cortisol Awakening Response 4849. Furthermore, exposure to the blue-light spectrum (460-nm) emitted by screens, specifically when lacking blue-light filters, actively suppresses the remnants of nocturnal melatonin, artificially spiking the morning cortisol curve but resulting in a subsequent collapse of midday drive, manifesting as fatigue and anxiety 4850.
Continuous Technological Stress and Multitasking
The physiological toll of digital media extends beyond the waking hour. Studies utilizing the Trier Social Stress Test (TSST) and dual-task paradigms assess the biological cost of uninterrupted technology usage. In cohorts of adults and adolescents, the total duration of unrestricted smartphone use directly correlates with measurable increases in salivary cortisol during task execution 51. Furthermore, excessive smartphone usage is linked to elevated levels of Interleukin-6 (IL-6), a primary pro-inflammatory cytokine, indicating a deep biological link between digital hyper-connectivity and systemic immune stress 52.
Interestingly, some research points to a "digital pacifier" effect, where moderate phone checking provides temporary psychological relief in stressful environments. However, when digital engagement replaces physical social interaction or becomes a chronic compulsion, it universally drives up baseline allostatic load, sustaining cortisol secretion long past the point of functional utility 5153.
Cyberpsychology and Social Media-Driven Self-Diagnosis
The explosion of cortisol-related wellness content is inextricably linked to the mechanics of social media algorithms and their impact on public health psychology. Platforms such as TikTok and Instagram deploy highly sophisticated engagement algorithms that curate individualized "For You" feeds 54. These systems excel at identifying a user's latent anxieties or physical complaints - such as fatigue, bloating, or difficulty concentrating - and inundating them with content attributing these universal experiences to specific pathologies 54.
The Rise of Cyberchondria
This algorithmic amplification has birthed a culture of rampant self-diagnosis. Individuals with no medical training routinely utilize short-form video content to intrinsically establish themselves as suffering from complex conditions like ADHD, autism, or severe HPA axis dysregulation 5455. Surveys tracking adolescent behavior reveal that up to 25% of young people have self-diagnosed a mental health or endocrine issue strictly based on social media consumption, with 30% of that demographic relying exclusively on TikTok 56.
While these platforms provide essential community support and destigmatize chronic illness, they simultaneously fuel "cyberchondria" - a clinical state characterized by heightened, persistent health anxiety driven by endless online medical research 5457. The dissemination of inaccurate or highly biased information (with researchers noting that over 30% of mental health videos on TikTok contain explicit misinformation) frequently leads users to adopt incorrect labels, delaying actual professional intervention 5758.
The Paradox of Wellness-Induced Anxiety
The psychological data regarding digital consumption is stark. Massive longitudinal studies, including research conducted by UNC-Chapel Hill following college students over 18 months during the pandemic, demonstrate that a mere one-hour daily increase in social media usage results in significant, measurable spikes in clinical depression and anxiety 59. Global psychiatric data confirms that excessive social media consumption (exceeding three hours daily) increases the baseline risk of depression by 33% in young adults 53.
The deep irony of the current cortisol trend is that the relentless pursuit of "optimizing" the hormone has become a primary driver of its elevation. Continuously monitoring wearable data for stress spikes, obsessively curating diets to avoid "cortisol belly," and agonizing over perceived facial puffiness initiates a chronic psychological stress response 635. The physiological manifestations of anxiety - including elevated heart rate, galvanic skin response, and increased blood pressure - mirror the exact stress markers consumers are desperately attempting to suppress 60. The obsession with fixing cortisol, therefore, guarantees that cortisol remains perpetually elevated.
Global Variations in the Digital Wellness Market
The fixation on cortisol and biological tracking is not uniformly distributed but represents a broader global shift in the $1.8 trillion wellness economy. Industry analysts and global wellness summits note a stark bifurcation in the modern market, splitting into two distinct ideologies: "hardcare" and "softcare" 68.
"Hardcare" encompasses the hyper-medicalized, tech-driven pursuit of longevity and absolute biological optimization, characterized by continuous glucose monitors, intensive biomarker tracking, and anti-aging regimens 68. Conversely, "softcare" represents a rejection of relentless optimization, focusing instead on low-pressure, community-driven emotional wellbeing, restorative sleep, and psychological grace 68.
Data extracted from global wearable technologies, encompassing millions of users, provides context to these trends. Nations prioritizing active transit and community health exhibit vastly superior physiological metrics compared to highly stressed, tech-centric populations.
| Global Region | Notable Wearable Health Metric (2025 Aggregated Data) | Societal and Wellness Implications |
|---|---|---|
| Scandinavia (Sweden, Norway, Denmark) | Lowest average Cardiovascular Age (CVA) globally (e.g., Sweden at -2.8 years) 61. | High integration of active commuting, strong social safety nets, and robust outdoor culture 61. |
| Oceania (New Zealand, Australia) | Highest global sleep scores (80.0 and 79.4, respectively) 61. | Cultural emphasis on work-life separation and outdoor environmental access 61. |
| Western Europe (Ireland, Spain, Italy) | Highest daily step counts (Ireland averaging 8,924 steps/day) 61. | Walkable urban infrastructure reducing reliance on sedentary transport, supporting baseline parasympathetic tone 61. |
| United States | Highest daily "Stressed Minutes" recorded (121.2 minutes/day) 61. | Fast-paced, hyper-connected work culture; extreme economic pressure driving systemic chronic HPA axis activation 61. |
These variations have sparked an emerging counter-trend termed "analog wellness." Consumers, particularly older Gen Z and Millennials, are increasingly seeking digital detoxes, returning to pre-digital hobbies, and demanding offline experiences to combat the physiological toll of continuous connectivity 6271. This analog movement intuitively addresses the root causes of HPA axis dysregulation by enforcing boundaries that allow the nervous system to transition securely into parasympathetic recovery.
Conclusion
The contemporary discourse surrounding cortisol serves as a profound case study in the translation - and frequent distortion - of clinical science into digital wellness trends. The social media narrative that characterizes cortisol as a toxic element responsible for facial puffiness, fatigue, and weight gain actively ignores the hormone's indispensable role in survival, metabolic regulation, and immune homeostasis. The terms "adrenal fatigue" and "cortisol face" are medically invalid, representing social media constructs that conflate transient lifestyle edema and central nervous system down-regulation with severe endocrine pathology.
While nutritional interventions and adaptogenic botanicals like Ashwagandha possess defined biochemical utilities, they are not universal antidotes for modern exhaustion. True regulation of the hypothalamic-pituitary-adrenal axis cannot be purchased in a supplement container; it is intrinsically tied to behavioral and environmental modification. Establishing rigid boundaries around digital technology use, managing photic exposure to preserve the Cortisol Awakening Response, and prioritizing low-grade, consistent physical movement are the scientifically validated methodologies for restoring endocrine balance. Ultimately, cortisol is not a biological error to be suppressed, but an elegant, vital messenger reflecting the exact demands placed upon the human body.