How mRNA Flu Vaccines Compare to Traditional Shots
Messenger RNA (mRNA) flu vaccines utilize a temporary set of genetic instructions to teach human cells how to build a harmless influenza protein, which safely trains the immune system to fight off the actual virus. In contrast, traditional flu shots inject weakened or killed viruses - or pieces of their proteins - directly into the body to trigger that same immune defense. Because mRNA vaccines skip the arduous process of growing live viruses in laboratories, they can be manufactured in a fraction of the time, offering a much more accurate match to circulating flu strains and significantly stronger protection, albeit with a higher likelihood of temporary side effects like a sore arm or fever.
The Enduring Challenge of Seasonal Influenza
Seasonal influenza remains one of the most formidable public health challenges of the modern era. Every year, particularly in the Northern Hemisphere between October and May, the flu virus causes tens of millions of illnesses. According to data tracking the 2025 - 2026 winter season, the United States alone experienced between 31 million and 54 million flu illnesses, resulting in up to 24 million medical visits, 780,000 hospitalizations, and 78,000 deaths 1. While annual vaccination is universally recommended as the best defense against severe flu-related complications, the clinical effectiveness of the traditional flu shot varies wildly from year to year. Over the past fifteen years, the overall effectiveness of the seasonal flu vaccine has fluctuated dramatically, ranging anywhere from a meager 19% to a high of 60% 1.
This massive variance in protection is primarily driven by a biological phenomenon known as antigenic drift. Influenza viruses are infamous for their ability to evolve quickly and without warning 1. As the virus replicates and spreads from person to person, its genetic code accumulates minor mutations, gradually altering the shape of the proteins on its surface. If the virus mutates significantly after scientists have chosen the specific strains for the annual vaccine formulation, the resulting shot will offer diminished protection by the time winter arrives 2. For decades, researchers, epidemiologists, and immunologists have been searching for a methodological breakthrough to improve both the speed of manufacturing and the accuracy of flu vaccine strain matching.
The unprecedented success of messenger RNA technology during the global response to the COVID-19 pandemic triggered a revolution in vaccinology. Major pharmaceutical companies immediately pivoted this validated technology toward seasonal influenza. By thoroughly examining how traditional flu shots have been manufactured for generations and contrasting that process with the novel mechanics of mRNA alternatives, the public health community can clearly articulate why this platform could fundamentally disrupt how we prevent respiratory illness 13.
The Mechanics of Traditional Flu Shot Manufacturing
To fully grasp the disruptive nature of mRNA technology, one must first understand the historical standard of care it aims to replace. Traditional vaccines primarily function by introducing the immune system to a harmless version of the target pathogen. Immunologists often compare this to giving the body's cellular security system a physical "mugshot" of an intruder 5. Once the immune system recognizes the structural shape of the viral mugshot, it begins producing antibodies. These specialized defense proteins are engineered to recognize, bind to, and neutralize the actual virus if it ever attempts to infect the host in the future.
Currently, the global pharmaceutical industry relies on three distinct methodologies to manufacture traditional seasonal influenza vaccines.
The Legacy of Egg-Based Cultivation
First utilized in the 1940s, egg-based manufacturing remains the most common method for producing influenza vaccines worldwide 14. The process begins when global health authorities select the candidate vaccine viruses (CVVs) for the upcoming season. Scientists then inject these specific flu viruses into millions of embryonated (fertilized) chicken eggs. The eggs serve as natural bioreactors, incubating the virus for several days to allow it to replicate and multiply 458. Once sufficient viral mass is achieved, the virus-laden fluid is harvested from the eggs. The virus is subsequently purified and chemically inactivated, or killed, ensuring that it cannot cause illness when injected into a human patient 45.
While egg-based vaccines have an extensive safety record spanning more than seventy years and are generally considered safe even for individuals with severe egg allergies, the methodology suffers from two profound biological and logistical flaws 14. The most glaring issue is the sheer duration of the production cycle. The entire logistical chain - from selecting the viral strains, securing millions of specialized eggs, cultivating the virus, purifying the antigen, and packaging the final vials - requires approximately six to eight months 18. Because of this immense lag time, the World Health Organization and the United States Food and Drug Administration are forced to finalize their strain recommendations for the Northern Hemisphere's winter flu season in February or March 126. This timeline leaves a massive half-year window during which the circulating wild virus can genetically drift away from the chosen vaccine strains.
The second major flaw is a phenomenon known as egg-adapted antigenic mismatch. Human influenza viruses are not naturally optimized to infect and replicate within avian cells. When human flu viruses are forced to grow inside chicken eggs, the viruses naturally acquire rapid adaptive mutations to survive and reproduce more efficiently in the avian environment 35. These egg-adapted mutations structurally alter the virus's primary surface antigen, the hemagglutinin (HA) protein. Consequently, the final vaccine may contain an antigen that structurally diverges from the wild-type strain circulating in the human population, directly reducing the vaccine's clinical efficacy even if the original strain prediction was perfectly accurate 135.
Modernizing with Cell-Based and Recombinant Technologies
To circumvent the limitations of egg adaptation, the pharmaceutical industry developed cell-based vaccine manufacturing. Instead of utilizing chicken eggs, the candidate flu viruses are inoculated into mammalian cell cultures, most commonly Madin-Darby Canine Kidney (MDCK) cells, housed within large industrial bioreactors 458. Because the virus is growing in mammalian cells rather than avian environments, it is far less likely to undergo the adaptive mutations that alter the hemagglutinin protein 57. Cell-based vaccines, such as Flucelvax, generally offer a moderately better match to circulating strains and have shown slight efficacy advantages over egg-based counterparts, particularly during seasons dominated by the highly mutable H3N2 influenza strain 17.
A third methodology, recombinant vaccine manufacturing, completely removes the need to cultivate a live influenza virus. In this highly synthetic process, scientists isolate the exact genetic code responsible for the influenza virus's hemagglutinin protein. They insert this genetic sequence into a baculovirus - a distinct type of virus that exclusively infects invertebrates and is entirely harmless to humans. This genetically modified baculovirus is then introduced into a culture of insect cells, instructing the insect cells to express mass quantities of the pure influenza HA protein 488. The protein is harvested, purified, and formulated into a vaccine, such as Flublok. Recombinant vaccines entirely eliminate egg-adaptive mutations and generally induce a stronger immune response due to a higher concentration of pure antigen 18.
Despite these advancements, cell-based and recombinant platforms still require extensive physical culturing of organic cells in massive bioreactors. While they solve the biological problem of egg adaptation, they only offer modest improvements to the overall manufacturing timeline, still requiring several months to scale up production ahead of the autumn vaccination window 287.
The Science of Messenger RNA Technology
Messenger RNA vaccines represent a fundamental paradigm shift in vaccinology. Instead of relying on the traditional method of injecting a physical piece of the actual pathogen to trigger immunity, mRNA acts as a biological instruction manual 9.
To understand how this works, one must look at fundamental cellular biology. Within every human cell, DNA serves as the permanent genetic blueprint, securely locked inside the cell nucleus. However, the cellular machinery that actually builds the proteins required for life resides outside the nucleus, in the cytoplasm. To bridge this gap, the cell creates a temporary, single-stranded copy of the specific DNA instructions needed at any given moment. This messenger molecule is called mRNA. It travels from the nucleus to the cytoplasm, where cellular structures called ribosomes read its code and assemble the corresponding protein. Once the protein is built, the fragile mRNA strand is rapidly degraded and discarded 1011.
An mRNA vaccine simply harnesses this natural, elegant machinery. Scientists chemically synthesize a strand of mRNA in a laboratory that carries the specific genetic code for the influenza virus's hemagglutinin (HA) protein. It is crucial to note that this is merely the blueprint for a single, isolated structural component of the virus; it is entirely harmless and lacks the genetic information required to assemble a functional, infectious virus 31213.
Overcoming Biological Hurdles
While the concept of mRNA therapeutics dates back to foundational experiments on mice in 1990, the technology faced decades of immense biological hurdles 1714. Naked mRNA is highly unstable and extremely labile; if injected directly into the human bloodstream, it is immediately recognized as foreign debris and rapidly destroyed by the body's natural ribonuclease enzymes before it can ever reach a cell 10. Furthermore, synthetic RNA can trigger a massive, unwanted inflammatory response from the innate immune system.
The breakthrough that enabled modern mRNA vaccines involved two critical innovations. First, researchers discovered that by slightly modifying the nucleoside building blocks of the RNA - specifically substituting uridine for a naturally occurring variant called pseudouridine or N1-methylpseudouridine - they could successfully evade the body's immediate inflammatory alarms and greatly enhance the molecule's stability 1015. Second, to physically protect the fragile mRNA and facilitate its delivery into human cells, scientists encapsulated the genetic instructions inside a microscopic, protective bubble of fat known as a lipid nanoparticle (LNP) 101621.
The Mechanism of Action Inside the Body
When a patient receives an intramuscular injection of an mRNA flu vaccine, a rapid and highly orchestrated biological sequence unfolds. The lipid nanoparticles carry the mRNA payload safely through the extracellular environment and fuse with the outer membranes of muscle cells and local immune cells in the arm 1112.
Once the lipid nanoparticle deposits the mRNA into the cell's cytoplasm, the human cell's own ribosomes read the synthetic genetic instructions and begin assembling the viral hemagglutinin protein 1214.
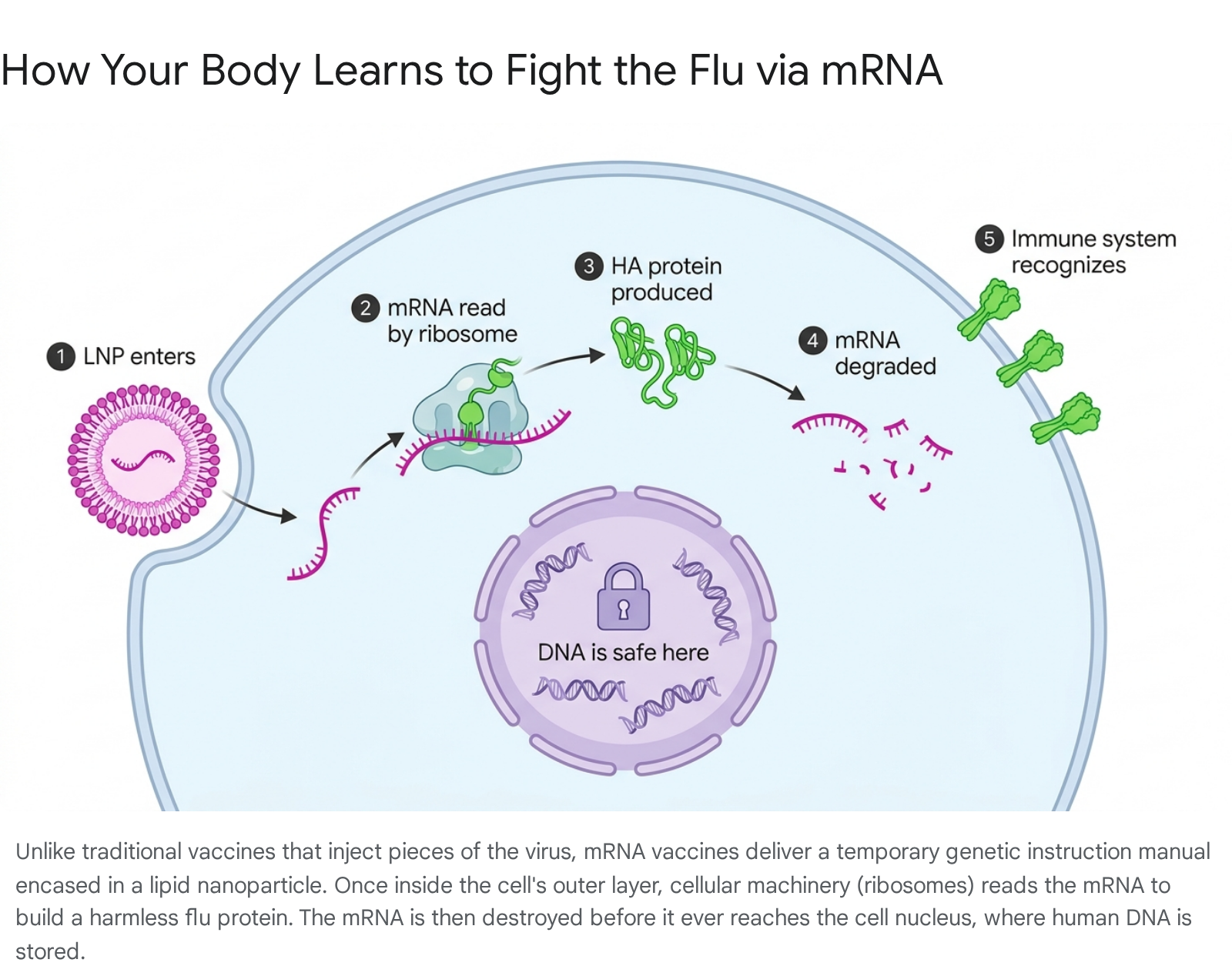
The host cell then transports these newly built, harmless viral proteins and displays them on its outer surface 1217.
The body's circulating immune cells immediately detect these protruding hemagglutinin proteins. Recognizing that the proteins are distinctly foreign and do not belong in the human body, the immune system initiates a robust defensive response 121718. B-cells begin producing highly specific neutralizing antibodies designed to latch onto the HA protein. Simultaneously, the vaccine triggers a profound cellular immune response. Studies demonstrate that mRNA vaccines prompt the activation of polyfunctional CD4+ T-helper cells and CD8+ cytotoxic T-cells 818. While antibodies prevent a virus from initially entering a cell, CD8+ T-cells act as specialized infantry, actively seeking out and destroying cells that have already been infected. This dual-layered response - both humoral and cellular - can lead to broader and significantly longer-lasting protection against severe clinical disease 81819.
After the cellular machinery has read the mRNA instruction manual, the synthetic genetic material is rapidly dismantled by normal cellular enzymes. It is completely discarded by the body within a matter of days and leaves no permanent trace 101217. If the vaccinated individual is exposed to an actual circulating influenza virus weeks or months later, their immune system instantly recognizes the hemagglutinin protein on the viral envelope, deploying an immediate and overwhelming antibody and T-cell response to neutralize the infection before it can cause severe illness 512.
How mRNA Vaccine Production Solves the Timeline Crisis
The most critical operational advantage of the mRNA platform over traditional methods is its sequence-independent, purely synthetic manufacturing process 12. Traditional vaccines require researchers to physically cultivate biological viruses. Whenever global health agencies recommend a new strain, manufacturers must determine how to coax that specific virus to grow efficiently in eggs or cell cultures, which frequently leads to unexpectedly low yields, biological contamination risks, and massive production delays 812.
With mRNA, scientists do not need to grow a virus at all. The manufacturing process relies entirely on in vitro (test tube) chemical synthesis 212526. The production cycle begins with the computational design of a plasmid DNA template that contains the targeted RNA sequence. This plasmid is amplified using a bacterial expression system, typically E. coli, within relatively small 5- to 50-liter fermentors 2125. The harvested DNA template is purified and subjected to a biochemical process called in vitro transcription (IVT). During IVT, specialized enzymes, such as T7 or Sp6 RNA polymerase, read the DNA template and synthesize massive quantities of the corresponding mRNA molecules in a cell-free environment 2125. Finally, the pure mRNA is capped to prevent degradation and mixed with lipids in specialized microfluidic chambers to form the final lipid nanoparticles 1121.
This highly controlled, biochemical process requires vastly smaller facility footprints compared to the sprawling agricultural supply chains needed for embryonated chicken eggs 25. More importantly, it dramatically compresses the strain-to-dose manufacturing timeline. While traditional egg-based vaccines require roughly sixteen to twenty-four weeks (four to six months) from strain selection to finished product, the mRNA production cycle can be executed in roughly seven to eight weeks 23.

By shrinking this production window by months, public health agencies could theoretically delay their annual strain selection until much closer to the start of the autumn flu season 120. This ensures the chosen vaccine formulation is a tighter genetic match to the virus that is actually beginning to circulate in the population, effectively eliminating the risk of egg-adaptive mutations and minimizing the impact of natural viral drift 23.
Direct Comparison: mRNA vs. Traditional Platforms
To summarize the sweeping differences between the established standard of care and the emerging mRNA technology, a side-by-side analysis of key metrics highlights the operational and clinical distinctions.
| Feature | Traditional Flu Shots (Egg/Cell-Based) | mRNA Flu Vaccines |
|---|---|---|
| Mechanism of Action | Injects chemically weakened/dead viruses or isolated viral proteins directly into the body 521. | Injects temporary genetic instructions (mRNA) that direct human cells to build the antigen 51214. |
| Manufacturing Timeline | Approximately 16 to 24 weeks (up to 6 months) from strain selection to final dosage 23. | Approximately 7 to 8 weeks, allowing for late-season strain matching 3. |
| Live Virus Risk | Nasal sprays contain live attenuated virus; standard shots contain inactivated (dead) virus 521. | Contains zero whole microbes, live virus, or dead virus particles 51617. |
| Relative Clinical Efficacy | Serves as the established baseline standard for seasonal protection 2230. | Demonstrated 26.6% to 34.5% higher relative efficacy compared to standard traditional shots in late-stage trials 53023. |
| Common Reactogenicity | Mild injection-site pain and fatigue, occurring in roughly 30% to 43% of patients 1. | Moderate injection-site pain, headache, and fatigue, occurring in roughly 65% to 70% of patients 11624. |
| Allergy Considerations | Egg-based shots contain trace amounts of egg protein (though widely deemed safe by health agencies) 4. | Completely egg-free, cell-independent, and manufactured purely synthetically 312. |
Efficacy Analysis: Do mRNA Flu Vaccines Work Better?
The theoretical advantages of mRNA technology - speed, purity, and robust cellular immune activation - must ultimately translate into clinical superiority to justify disrupting a seventy-year-old global manufacturing infrastructure. Recent data from massive, multinational late-stage clinical trials indicate that mRNA flu vaccines consistently outperform standard-dose traditional vaccines in preventing symptomatic illness.
During the 2022 - 2023 flu season, Pfizer conducted a massive Phase 3 clinical trial testing its experimental mRNA flu candidate against a traditional egg-based quadrivalent vaccine. The study spanned the United States, South Africa, and the Philippines, enrolling over 18,000 healthy adults 151325. The final data revealed that the mRNA vaccine resulted in 34.5% fewer laboratory-confirmed, flu-like illnesses compared to the traditional standard-of-care shot 5162526. The vaccine proved highly capable of neutralizing the dominant circulating strains of that season, predominantly influenza A strains H3N2 and H1N1, while also protecting against the B strains Victoria and Yamagata 2526.
Moderna's pursuit of an mRNA flu vaccine yielded similarly striking results. In a massive Phase 3 clinical trial dubbed "Fluent," researchers evaluated Moderna's mRNA-1010 seasonal flu vaccine against standard-dose traditional vaccines (such as Fluarix) 242736. The trial enrolled more than 40,000 adults aged 50 and older across 301 sites in 11 countries during the 2024 - 2025 Northern Hemisphere influenza season 242728. Published in The New England Journal of Medicine in May 2026, the primary efficacy endpoint was determined by reverse-transcriptase-polymerase-chain-reaction (RT-PCR) confirmed influenza cases 242930.
The Fluent trial results demonstrated that just 2.0% of the participants who received the mRNA-1010 vaccine contracted the flu, compared to 2.8% of those receiving the standard-dose comparator 27282931. This absolute risk reduction translated to a highly significant relative vaccine efficacy (rVE) of 26.6% in favor of the mRNA platform 242729. Furthermore, the protection remained remarkably consistent across the specific circulating flu strains, achieving an rVE of 29.6% against influenza A/H1N1, 22.2% against A/H3N2, and 29.1% against B/Victoria 2327283242. Crucially, the vaccine maintained its superior performance in vulnerable demographics; among the 19,260 trial participants aged 65 years and older, the mRNA vaccine exhibited a 27.4% relative vaccine efficacy 23273242. The trial also documented a meaningful reduction in disease burden, noting a 33.7% relative reduction in patients seeking professional healthcare visits for flu-related symptoms compared to the standard vaccine group 27.
It is important to contextualize that these superiority trials measured mRNA candidates against standard-dose traditional vaccines. While the results are unequivocally positive, independent experts note that further studies will eventually be required to compare mRNA vaccines head-to-head against enhanced flu shots - such as high-dose, adjuvanted, or recombinant formulations - which are currently the preferential recommendation for older adults facing severe flu complications 22242731.
The Reactogenicity Trade-Off
The primary clinical downside to current mRNA flu vaccines is a noticeably higher rate of short-term side effects. In the medical community, this phenomenon is referred to as "reactogenicity" - the physical manifestations of the body's immune system actively responding to the vaccine 101618.
Because mRNA vaccines encapsulated in lipid nanoparticles are incredibly efficient at stimulating immune responses, they frequently cause the recipient to experience temporary, flu-like symptoms as the body furiously builds its defenses 1022. In Moderna's Phase 3 Fluent trial, local injection-site pain was reported by 65.8% of participants who received the mRNA vaccine, compared to just 29.8% of those who received the traditional comparator shot 24273631. Systemic symptoms followed a similar pattern; fatigue was reported in 45.1% of mRNA recipients versus 20.3% in the control group, headache in 37.8% versus 18.0%, and muscle aches (myalgia) in 35.4% versus 11.6% 3631.
While these figures suggest a much more physically demanding patient experience in the day following vaccination, medical experts emphasize that these reactions are almost entirely mild to moderate in severity and heavily transient, typically resolving completely within one to two days 183024263631.
Most importantly, higher reactogenicity does not equate to diminished safety. The rates of serious adverse events (SAEs) were virtually identical between the two trial groups, occurring in 2.2% of mRNA-1010 recipients and 1.9% of standard-dose recipients 302427362931. Extensive monitoring during the trials identified no cases of myocarditis or pericarditis associated with the mRNA flu vaccine within the predefined high-risk observation windows 124. Furthermore, large-scale real-world data tracking adverse events following immunization (AEFI) via VigiBase systems showed that while mRNA vaccines predictably cause more systemic chills, myalgia, and fatigue, they actually demonstrated a lower risk of serious neurological complications - such as Guillain-Barre syndrome and neuralgia - compared to traditional influenza vaccines 33.
For patients and healthcare providers, the impending arrival of mRNA flu vaccines will require counseling on a fundamental trade-off: accepting twenty-four hours of feeling temporarily unwell in exchange for a significantly heightened level of seasonal protection against actual influenza infection 52231.
Debunking Common mRNA Vaccine Misconceptions
Because mRNA technology was deployed at an unprecedented global scale to combat the COVID-19 pandemic, it rapidly became the subject of widespread public confusion, suspicion, and misinformation 15. Despite the perceived suddenness of its arrival, fundamental research and development into mRNA vaccines had been steadily progressing in academic and corporate laboratories for more than three decades 17141720. To ensure high vaccination compliance, infectious disease experts continually work to debunk lingering myths surrounding the technology.
A prominent fear is the misconception that mRNA vaccines have the capability to alter a patient's DNA. This is scientifically impossible 91734. Human DNA is securely housed within the nucleus of the cell. The synthetic genetic material delivered by an mRNA vaccine operates entirely in the cell's cytoplasm and lacks the required biological machinery to penetrate the nuclear membrane 91217. Because the mRNA and the host's DNA never share the same physical space, they cannot interact, meaning the vaccine cannot change, alter, or integrate into a person's genetic code 9121734.
Another widespread myth suggests that receiving an mRNA vaccine can infect a patient with the disease it is designed to prevent. However, mRNA vaccines contain absolutely zero whole microbes, live viruses, or inactivated dead viruses 51617. They merely contain a sequence of code representing a single, isolated protein 14. Without the complete viral genome, it is biologically impossible for the vaccine to assemble into a functional virus and cause an infection 59.
Similarly, fears of "vaccine shedding" - where a vaccinated individual allegedly exhales or excretes vaccine components that infect others - are baseless regarding mRNA platforms. Viral shedding can only occur when a patient is inoculated with a vaccine containing a live, weakened virus, such as certain traditional nasal spray flu vaccines 1721. Because mRNA vaccines utilize no viruses whatsoever, they cannot shed or release infectious material into the environment 17.
Finally, claims asserting that mRNA vaccines cause female infertility or pregnancy complications lack any grounding in scientific evidence. The mRNA blueprint and the resulting flu protein bear no structural or biological resemblance to the reproductive proteins required for placental attachment or fertility, and extensive monitoring has demonstrated no adverse effects on human reproduction 9.
The Future of Flu Prevention: 2026 and Beyond
The global regulatory landscape for mRNA influenza vaccines is evolving rapidly. Following the publication of their successful Phase 3 clinical trials, manufacturers are actively seeking marketing authorizations from leading global health agencies.
In the United States, the trajectory of mRNA approval faced a brief period of uncertainty. Early in 2026, the FDA unexpectedly declined to review Moderna's application for mRNA-1010, citing concerns that the trial utilized standard-dose comparators rather than high-dose vaccines for the over-65 demographic 20302731. However, following intense discussions regarding differing regulatory pathways based on age demographics, the agency reversed course. The FDA officially accepted the application and established a Prescription Drug User Fee Act (PDUFA) target action date of August 5, 2026, to complete its review 3027363145. If the FDA grants approval, mRNA-1010 could be available to the American public in time for the 2026 - 2027 influenza season 203045. Internationally, the vaccine has already been accepted into the formal approval pipelines of the European Union, Canada, and Australia 31.
This impending technological shift perfectly coincides with a global update in seasonal flu prevention strategies. For years, standard flu shots were "quadrivalent," designed to protect against two strains of influenza A (H1N1 and H3N2) and two strains of influenza B (Victoria and Yamagata) 4. However, comprehensive surveillance indicates that the B/Yamagata lineage has not been detected anywhere in the world since March 2020 and is presumed to have been naturally eradicated 35. Consequently, global health authorities, including the WHO and the FDA, mandated a shift back to "trivalent" (three-strain) vaccines for the 2025 - 2026 and 2026 - 2027 seasons, omitting the unnecessary Yamagata strain 6353637. The new mRNA flu vaccines currently under regulatory review have already been engineered to match this updated, streamlined trivalent standard 2224273031.
Furthermore, the incredible speed of mRNA manufacturing will likely prove vital against rapidly emerging sub-variants. During the 2025 - 2026 season, health officials identified the sudden spread of an influenza A(H3N2) virus subclade J.2.4.1 (colloquially known as "subclade K") 353637. Because this subclade emerged rapidly over the summer, traditional egg-based manufacturers - locked into the strains they began cultivating in February - were helpless to update their vaccines. In the future, a fully established mRNA infrastructure, requiring only weeks to execute a strain update, could pivot during the summer to accurately match late-emerging threats like subclade K 132036.
The Ultimate Goal: Combination Respiratory Vaccines
Perhaps the most highly anticipated commercial development in the mRNA pipeline is the combination respiratory vaccine. By taking advantage of the modular and highly customizable nature of lipid nanoparticles, scientists can seamlessly insert the genetic instructions for multiple entirely different viruses inside the exact same delivery vehicle 49.
Moderna has aggressively pursued this frontier, reporting highly positive Phase 3 trial results for an investigational vaccine called mRNA-1083, which combines the seasonal influenza components of mRNA-1010 with a next-generation COVID-19 booster 4950. The trial demonstrated that a single injection of the combination shot elicited immune responses that were non-inferior - and in many metrics, statistically superior - to administering separate, currently licensed flu and COVID-19 vaccines simultaneously 50. In early 2026, the European Medicines Agency (EMA) became the first major regulatory body to issue a positive recommendation for this combination shot, designated mCombriax, for adults aged 50 and older 51.
For the general public, the availability of a highly effective, single-dose combined respiratory vaccine would dramatically reduce the logistical friction of scheduling multiple pharmacy visits each autumn. Public health officials anticipate this convenience will drastically improve seasonal vaccination compliance, ultimately reducing the crippling annual burden of co-circulating winter viruses on global healthcare systems 4950.
Bottom line
An mRNA flu vaccine represents a profound technological upgrade to global influenza prevention, swapping out the traditional method of injecting physical viral fragments in favor of delivering temporary genetic instructions that teach the human body to build its own highly targeted immune defenses. By completely bypassing the archaic and dangerously slow egg-based manufacturing process, mRNA vaccines can be produced in a matter of weeks rather than months, effectively eliminating the risk of egg-adaptive mutations and ensuring a much tighter genetic match to circulating flu strains. While patients should be counseled to anticipate a higher likelihood of transient, mild-to-moderate side effects like fatigue or a sore arm, exhaustive late-stage clinical trials demonstrate that the underlying technology is overwhelmingly safe, cannot alter human DNA, and provides statistically superior protection against seasonal illness compared to standard flu shots.