What the Flu Decision Means for the Future of mRNA
The U.S. Food and Drug Administration's upcoming decision on the first messenger RNA seasonal flu vaccine marks a pivotal moment for public health, offering next-generation shots that are up to 35 percent more effective but come with noticeably more frequent mild side effects like fatigue and arm pain. Beyond influenza, this regulatory milestone serves as a crucial stress test for a booming biotechnology pipeline that aims to use mRNA to tackle personalized cancer treatments, latent viruses, and global pandemic preparedness. Ultimately, the maturation of these vaccines will dictate how we manufacture, distribute, and experience genetic medicine over the next decade.
The Broken Paradigm of Seasonal Flu Vaccination
For more than eighty years, the global supply of influenza vaccines has relied on a slow, fragile, and mathematically perilous manufacturing process. Each year, public health agencies must predict which influenza strains will dominate the winter season globally. They make these predictions in February to allow manufacturers roughly six months to produce the vaccines for the fall. Historically, the vast majority of these vaccines have been manufactured by injecting circulating influenza viruses into millions of fertilized chicken eggs, where the virus is allowed to replicate before being harvested, inactivated, and purified.
This decades-old method carries a profound biological flaw known as egg-adapted antigenic mismatch. When human influenza viruses are forced to grow inside avian eggs, they often mutate to adapt to their temporary host environment. These adaptive mutations frequently occur on the hemagglutinin protein - the primary viral surface protein that the human immune system uses to recognize and attack the flu. If the virus mutates while incubating in the egg, the resulting vaccine will train the human immune system to fight a version of the virus that no longer matches the wild strain circulating in the population. Consequently, the real-world effectiveness of seasonal flu vaccines over the past fifteen years has fluctuated wildly, ranging from a moderately successful 60 percent to a dismal 19 percent.
The rapid, unprecedented success of messenger RNA technology during the COVID-19 pandemic offered a tantalizing, high-tech solution to this historical bottleneck. Because mRNA vaccines rely on synthetic genetic instructions rather than live biological cultures, they can be designed and manufactured in a matter of weeks rather than months. By avoiding the use of eggs, mRNA technology completely eliminates the risk of egg-adapted mutations. Furthermore, the accelerated production timeline theoretically allows public health officials to delay their strain selection until much closer to the start of the flu season, drastically improving the accuracy of the viral match. Yet, the transition from managing a novel pandemic emergency to disrupting the routine seasonal flu market has proven to be a complex scientific and regulatory challenge.
The Clinical Reality: Weighing Efficacy Against Reactogenicity
The fundamental question for health authorities, clinicians, and patients is whether mRNA flu vaccines actually outperform the traditional shots we have relied on for decades. Based on rigorous Phase 3 clinical trials published in the New England Journal of Medicine, the answer is a definitive yes - but with notable clinical trade-offs that could impact patient behavior.
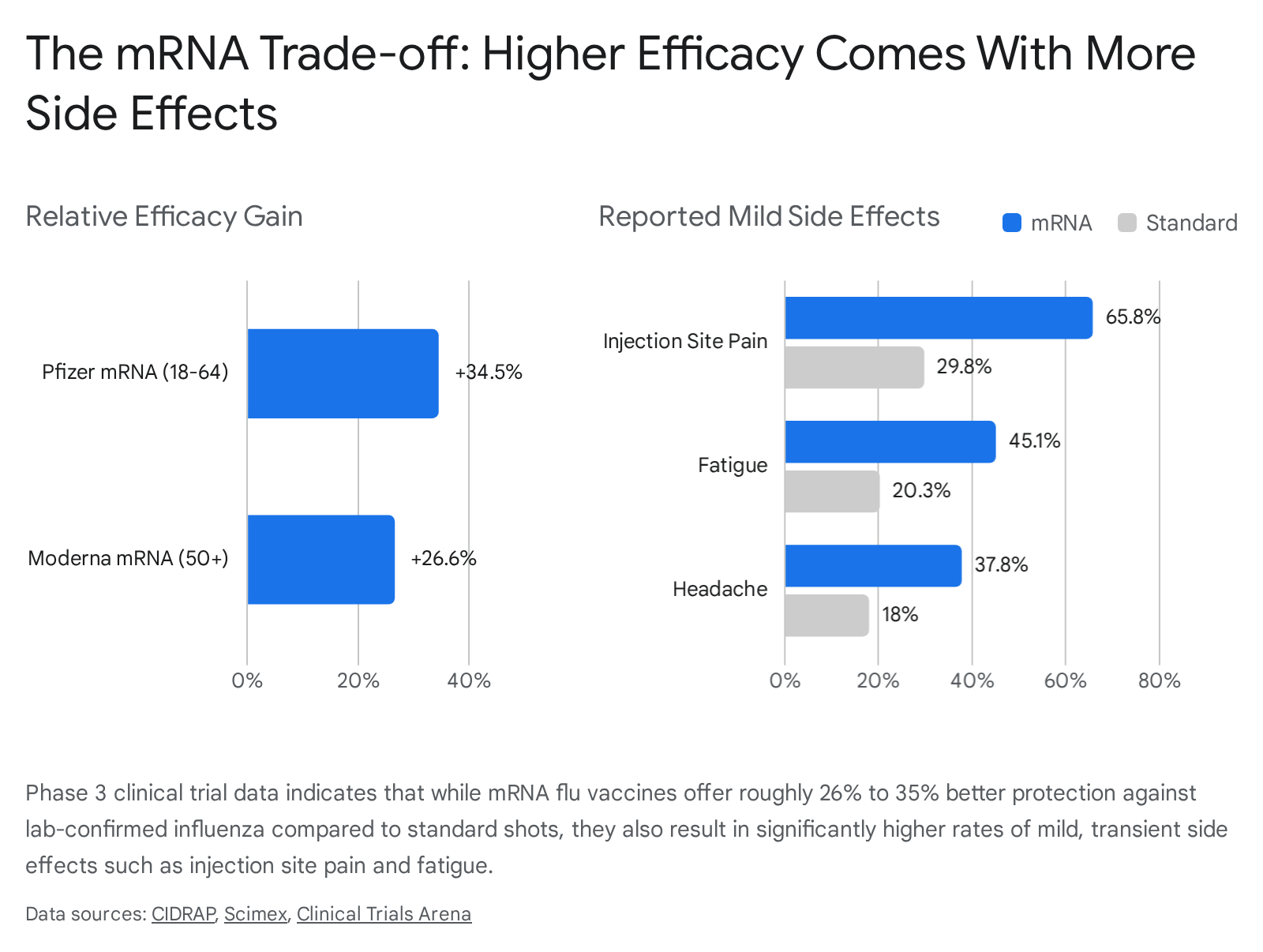
Two major pharmaceutical developers, Pfizer and Moderna, have provided the clearest picture of mRNA's potential in the seasonal influenza space. A global Phase 3 trial funded by Pfizer tested its experimental mRNA flu vaccine in over 18,000 healthy adults aged 18 to 64 during the 2022 - 2023 flu season. The results were highly encouraging: the mRNA vaccine had a relative vaccine efficacy of 34.5 percent compared to a standard, widely used egg-based shot known as Fluzone. In clinical terms, this means that the participants who received the mRNA vaccine experienced roughly 35 percent fewer lab-confirmed flu-like illnesses than those who received the traditional vaccine.
Moderna's Phase 3 trial for its investigational vaccine, mRNA-1010, painted a remarkably similar picture in an older, more vulnerable demographic. The trial enrolled over 40,000 adults aged 50 and older. Influenza-like illness was observed in just 2.0 percent of the mRNA-1010 recipients compared to 2.8 percent of those receiving the standard-dose comparator. This translates to a relative vaccine efficacy of 26.6 percent. In the world of respiratory virus vaccination, a 26 to 35 percent relative improvement over an existing, functional vaccine is considered a massive leap that could theoretically prevent hundreds of thousands of medical visits and tens of thousands of hospitalizations globally.

The biological cost of this robust immune response is known as reactogenicity - the expected, short-term physical side effects that occur when the innate immune system is aggressively activated. While mRNA vaccines excel at triggering both profound antibody production and deep cellular T-cell responses, they are notoriously reactogenic.
In the Moderna trial, nearly 66 percent of mRNA recipients reported localized injection-site pain, compared to just 30 percent of those receiving the standard conventional shot. Systemic symptoms followed a similar pattern. Fatigue was reported by 45 percent of the mRNA group versus 20 percent of the standard group, while headaches affected 38 percent compared to 18 percent. The Pfizer trial echoed these findings, noting that 5.6 percent of mRNA volunteers developed a fever, which was more than three times the rate observed in the conventional vaccine cohort.
While researchers emphasize that these symptoms are overwhelmingly mild to moderate and generally fade within one to two days, they present a genuine behavioral obstacle.
Public health officials are acutely aware of vaccine fatigue. Clinicians express concern that patients who previously experienced intense, flu-like side effects from mRNA COVID-19 boosters may choose to skip their annual flu shots entirely if they anticipate feeling run-down for a weekend. It is vital to note, however, that rigorous safety monitoring during these trials found absolutely no increase in serious adverse events. Rates of severe medical complications were nearly identical between the mRNA and standard vaccine groups, hovering around 2 percent for older adults, and there were zero reported cases of myocarditis or pericarditis (heart inflammation), effectively distancing the new seasonal shots from the rare cardiac signals occasionally associated with early pandemic vaccines.
The B-Strain Achilles Heel
While mRNA technology has proven highly adept at neutralizing Influenza A strains - such as H1N1 and H3N2, which traditionally cause the most severe seasonal outbreaks and hospitalizations - it has encountered an unexpected biological hurdle. First-generation mRNA flu vaccines have consistently struggled to generate strong, durable antibody responses against Influenza B strains.
Historically, seasonal flu shots have been quadrivalent, designed to protect against two strains of Influenza A and two lineages of Influenza B (Victoria and Yamagata). In clinical trials, the immunological non-inferiority criteria against B lineages were frequently not met by the mRNA candidates, a phenomenon that appears to be a class-wide effect across different mRNA platforms rather than a failure of one specific company.
Fortunately for mRNA developers, the global viral landscape has recently shifted in their favor. The Influenza B/Yamagata lineage has not been detected in global circulation since March 2020, likely driven to extinction by the unprecedented global masking and social distancing measures enacted during the COVID-19 pandemic. Recognizing that this extinct lineage no longer poses a threat to public health, the European Medicines Agency and the U.S. Food and Drug Administration have both strongly recommended transitioning away from quadrivalent vaccines. For the 2025 - 2026 and 2026 - 2027 seasons, regulatory agencies are endorsing trivalent formulations that omit the Yamagata strain. This naturally reduces the burden on mRNA vaccines to cover a strain they historically struggled with, allowing manufacturers to optimize their lipid nanoparticle formulations for the remaining viral threats.
Comparing the Influenza Vaccine Arsenal
As messenger RNA technology prepares to enter the commercial market, it will not operate in a vacuum. It must compete against several established, highly refined manufacturing platforms that currently dominate the seasonal influenza landscape. Understanding how mRNA measures up against these incumbent technologies is essential for evaluating its future market share.
| Vaccine Technology | Mechanism of Production | Production Speed | Efficacy and Mutation Risk | Reactogenicity |
|---|---|---|---|---|
| Egg-Based Inactivated (e.g., standard Fluzone) | Viruses are grown inside fertilized chicken eggs, inactivated with chemicals, and purified. | Slow. Requires 6 to 9 months and massive agricultural logistics. | Moderate. High risk of egg-adapted antigenic mismatch reducing real-world effectiveness. | Low. Generally causes minimal systemic side effects. |
| Cell-Based Inactivated (e.g., Flucelvax) | Viruses are grown in cultured mammalian cells (MDCK cells) rather than eggs. | Moderate. Faster scaling than eggs but still relies on biological growth. | Good. Mammalian cells prevent egg-adapted mutations, offering up to 20% better protection than standard egg shots in some seasons. | Low. Very well tolerated with minimal side effects. |
| Recombinant Protein (e.g., Flublok) | Viral proteins are synthesized genetically inside insect cells; entirely egg-free. | Fast. Takes 3 to 4 months once the genetic sequence is identified. | Excellent. Delivers three times the antigen dose of standard vaccines, highly effective for older adults. | Low to Moderate. Slightly higher local site pain than standard shots. |
| Messenger RNA (mRNA) (e.g., Moderna mRNA-1010) | Synthetic mRNA is encapsulated in lipid nanoparticles; cells read the RNA to build viral proteins. | Very Fast. Can be engineered and mass-produced in weeks to months. | Superior relative efficacy (26% to 35% higher than standard). Exact genetic sequence prevents mutation mismatch. | High. Frequent but mild, transient systemic symptoms like fatigue, headache, and fever. |
The Regulatory Rollercoaster: Moderna and the FDA
The path to securing approval for mRNA flu vaccines has been fraught with regulatory turbulence, highlighting the intense scrutiny applied to next-generation biologics in a post-pandemic world. In early February 2026, the FDA stunned the biotechnology sector by issuing a rare "refusal-to-file" letter regarding Moderna's biologics license application for its mRNA-1010 flu vaccine.
The initial rejection was deeply technical. Regulators expressed concern that Moderna's pivotal Phase 3 study had compared its novel mRNA vaccine against standard-dose flu vaccines in older adults. The FDA argued that this trial design did not accurately reflect the highest standard of care in the United States, as older adults are typically advised to receive high-dose or adjuvanted vaccines that offer superior protection against severe outcomes. Moderna swiftly countered that the original study design had been explicitly discussed and agreed upon during prior consultations with the agency, and that absolutely no safety or efficacy concerns had been raised regarding the data itself.
Following a high-priority emergency meeting, the FDA abruptly reversed course just one week later, agreeing to formally review the application. The agency established a Prescription Drug User Fee Act (PDUFA) target action date of August 5, 2026. Under the revised regulatory framework, Moderna is seeking full traditional approval for adults aged 50 to 64. For the more vulnerable population aged 65 and older, the company is pursuing an accelerated approval pathway, heavily contingent upon post-marketing commitments to conduct ongoing real-world studies assessing the vaccine's efficacy and safety in seniors.
If the FDA grants approval by the August deadline, it would allow Moderna to launch the vaccine in the United States just in time for the 2026 - 2027 respiratory virus season. Meanwhile, international regulators have advanced even faster. The European Medicines Agency recently issued a positive recommendation for mCombriax - Moderna's ambitious, first-of-its-kind combination vaccine targeting both influenza and COVID-19 in a single shot - for European adults aged 50 and older.
The Corporate Divide: Why Sanofi Walked Away
While Moderna and Pfizer double down on bringing seasonal mRNA flu vaccines to the public, other pharmaceutical titans have assessed the landscape and fundamentally altered their strategies. In late January 2026, French pharmaceutical giant Sanofi quietly announced in its full-year earnings documents that it had entirely deprioritized its mRNA-based seasonal flu vaccine program, effectively terminating a Phase 1 clinical trial for a hexavalent candidate.
This decision sent shockwaves through the industry, particularly given that Sanofi had acquired the mRNA-focused biotechnology firm Translate Bio in 2021 for a staggering $3.2 billion. However, from a corporate and clinical perspective, the pivot made logical sense. Sanofi executives acknowledged the persistent class-wide struggles that mRNA platforms face in generating robust immune responses against Influenza B strains. More importantly, Sanofi already commands a dominant and highly lucrative share of the premium influenza market. The company manufactures Fluzone High-Dose (an enhanced egg-based shot) and Flublok (an advanced recombinant protein vaccine). Both of these existing products are explicitly approved by the FDA and have consistently demonstrated exceptional protection against severe flu complications in older adults.
Rather than spend billions of dollars navigating regulatory hurdles to launch a highly reactogenic mRNA product that would merely cannibalize the sales of its own highly successful premium vaccines, Sanofi decided to preserve its mRNA resources for a much larger threat. The company is continuing active Phase 1 and Phase 2 trials for an mRNA-based vaccine targeting the H5 avian influenza strain. Sanofi is placing a calculated bet that the true, unparalleled value of messenger RNA lies not in the crowded, incremental market of seasonal sniffles, but in the rapid-response demands of pandemic preparedness, where the ability to manufacture hundreds of millions of doses in a matter of weeks is a matter of global survival.
Expanding the Pipeline: Cancer, RSV, and Latent Viruses
The intense focus on seasonal influenza is ultimately a stepping stone. If regulatory bodies like the FDA and EMA formalize the approval pathways for routine, non-emergency mRNA vaccines, they will unlock a massive biotechnology pipeline designed to treat some of the most complex diseases in human history.
Oncology and Personalized Cancer Vaccines
The most highly anticipated and financially significant application of messenger RNA over the next decade lies in the field of oncology. Because mRNA technology simply provides instructions for human cells to build specific proteins, it can be entirely customized to fight cancer.

By taking a biopsy of a patient's tumor and genetically sequencing it, scientists can identify the unique mutations - known as neoantigens - that are specific to that individual's cancer. Those sequences can then be coded into a bespoke mRNA vaccine and injected back into the patient. The goal is to train the patient's own immune system to recognize those specific tumor markers, hunting down micro-metastases and preventing the cancer from returning after surgery.
This is no longer theoretical science fiction. Major players like BioNTech anticipate the potential approval and commercial launch of their first mRNA-based therapeutic cancer vaccines between 2026 and 2030. Moderna, working in a lucrative partnership with Merck, has aggressively advanced its individualized neoantigen therapy (mRNA-4157) into late-stage Phase 3 clinical trials for adjuvant melanoma and non-small cell lung cancer. The same customized therapy is currently undergoing Phase 2 trials for renal cell carcinoma and various forms of bladder cancer.
Tackling Latent Viruses and Bacterial Pathogens
Beyond oncology, the mRNA platform is being forcefully directed at complex, latent viruses that hide within the human body and have evaded traditional vaccine development for decades. Traditional inactivated or live-attenuated vaccines have repeatedly failed to conquer pathogens like Cytomegalovirus (CMV) and Epstein-Barr virus (EBV), which causes infectious mononucleosis and is linked to multiple sclerosis. Today, Moderna has multiple mRNA candidates for both CMV and EBV advancing through Phase 2 clinical trials.
In the realm of HIV research, where an effective prophylactic vaccine has remained agonizingly out of reach despite billions of dollars in funding, the mRNA platform is allowing immunologists to iterate and test new ideas at breakneck speed. While no HIV candidate has yet advanced to Phase 3 efficacy trials, Phase 1 studies are actively using mRNA to attempt to stimulate the production of broadly neutralizing antibodies. A new clinical trial slated for late 2026, known as IAVI G004, will test specialized mRNA boosters designed to refine and strengthen this exact immune response. Furthermore, the platform is expanding beyond viruses entirely, making surprising inroads against bacterial threats; clinical candidates for Lyme disease and enteric viruses like Norovirus are currently progressing through Phase 2 and Phase 3 trials.
Democratizing Manufacturing: The WHO Phase 2.0 Initiative
While the types of diseases mRNA can treat are expanding rapidly, an equally important revolution is happening regarding where these life-saving therapeutics are actually manufactured. During the height of the COVID-19 pandemic, the centralization of mRNA technology and intellectual property in the Global North led to profound, devastating vaccine inequity, leaving the Global South waiting months for access to basic prophylactic care.
To ensure this catastrophic failure is never repeated, the World Health Organization (WHO) and the Medicines Patent Pool (MPP) launched a radical initiative known as the mRNA Technology Transfer Programme. The primary goal was to bypass the traditional pharmaceutical monopolies by freely sharing the knowledge, technology, and training required to build synthetic vaccines from scratch. Announced initially in 2021 with a central hub located at Afrigen Biologics in Cape Town, South Africa, the program quickly proved that developing nations could successfully reverse-engineer and produce clinical-grade mRNA vaccines without prior foundational infrastructure.
In October 2025, over a hundred global health leaders gathered in Brussels to officially launch Phase 2.0 of this massive initiative, which will run from 2026 through 2030. The program has expanded from a solitary proof-of-concept into a sprawling, collaborative network of fifteen manufacturing partners located across ten low- and middle-income countries spanning four continents. Phase 2.0 marks the critical transition from basic capacity building to achieving sustainable, commercial-scale production utilizing Good Manufacturing Practices.
By December 2026, all manufacturing partners in the network are expected to have demonstrated full technological integration at their respective sites. Together, this decentralized, Global South-led network has established the collective ambition to deliver up to 1.9 billion pandemic-ready doses autonomously in the event of a future global health emergency. Crucially, these state-of-the-art facilities cannot simply sit idle waiting for the next pandemic. To remain economically viable and maintain a highly skilled workforce, these regional hubs are establishing robust research consortia to utilize their newly acquired mRNA platforms against localized, neglected diseases. By pivoting their focus toward regional priorities such as tuberculosis, dengue fever, malaria, and leishmaniasis, the program ensures that the infrastructure is actively utilized, continuously improved, and ready to pivot instantly when a novel global threat emerges.
Dispelling Myths and Addressing Costs
As mRNA technology permeates routine healthcare, it is imperative to address the persistent misconceptions and economic realities that continue to shadow its deployment. The rapid proliferation of these vaccines has fueled a belief in some circles that mRNA will soon render all other forms of vaccination obsolete. Experts universally caution that this "mRNA or nothing" perspective is not based in scientific reality.
Traditional vaccine manufacturing platforms - such as the recombinant protein technology utilized in Flublok, or advanced cell-based systems - remain highly effective, exceptionally well-tolerated, and benefit from deeply entrenched global distribution networks. Furthermore, early preclinical studies of mRNA vaccines conducted prior to the pandemic against various infectious diseases sometimes yielded less impressive immunological results than traditional methods, serving as a reminder that synthetic RNA is not a universal skeleton key capable of instantly neutralizing all pathogens.
Public perception also remains a formidable hurdle. Despite billions of doses being safely administered globally, profound misunderstandings regarding the biology of mRNA persist. Medical professionals continually emphasize that mRNA vaccines do not - and biologically cannot - alter human DNA. The messenger RNA acts merely as a temporary, instructional "post-it note" that provides the cellular ribosomes with the blueprint to synthesize a target protein. Because the mRNA is highly unstable, it never enters the cell's nucleus where human chromosomes reside, and it is quickly degraded by cellular enzymes within a matter of days. Furthermore, the technology contains no live or inactivated viruses, no fetal cells, and no heavy metal preservatives, utilizing simple, biodegradable lipid nanoparticles (essentially microscopic fat bubbles) to protect the fragile genetic code during delivery into the cytoplasm.

Finally, the widespread adoption of seasonal mRNA vaccines will heavily depend on healthcare economics. Developing and manufacturing synthetic genetics remains an expensive endeavor. Currently, premium influenza vaccines tailored for older adults, such as Fluzone High-Dose, have a list price of roughly $78 per shot. While these costs are typically fully covered or heavily subsidized by government programs like Medicare Part B in the United States, public health budgets are finite. As mRNA flu vaccines enter the commercial market, their pricing strategies, evaluated against their higher reactogenicity profiles, will ultimately dictate whether they become the default public health recommendation or remain a premium, niche alternative for specific patient demographics.
Bottom line
The FDA's decision to advance the review of Moderna's mRNA seasonal flu vaccine signals a massive regulatory vote of confidence in the future of synthetic genetic medicine. While late-stage clinical data clearly proves these next-generation vaccines can deliver superior efficacy against certain influenza strains, the biological trade-off of higher rates of temporary side effects - coupled with ongoing struggles regarding B-strain coverage - means traditional, egg-free alternative vaccines will remain vital to public health. Ultimately, the maturation of these seasonal mRNA shots is paving the essential regulatory and manufacturing pathways necessary for the next true leaps in the platform: personalized oncology treatments, the eradication of latent viruses, and decentralized pandemic preparedness in the Global South.