How Is Neurodiversity Different From a Clinical Diagnosis
Neurodiversity is the biological reality that human brain function naturally varies across the population, framing these cognitive differences as valuable variations rather than inherent defects. A clinical diagnosis, conversely, is a formalized medical classification given only when a person's neurological traits cause significant functional impairment in their daily life. While a clinical diagnosis remains the primary legal gateway for medical treatments and educational accommodations, the neurodiversity paradigm advocates for supporting cognitive differences without strictly pathologizing them.
The Operating Systems of the Human Mind
To understand the core distinction between neurodiversity and clinical psychiatry, it helps to conceptualize the human brain through the lens of computing. If an individual operates on a macOS device, their computer processes information, executes commands, and organizes data differently than a machine running a Windows operating system. Neither operating system is inherently diseased or broken; they simply possess different underlying architectures. However, if an end-user attempts to run Windows-native software on a macOS device without an appropriate emulator, the system will struggle, crash, or fail to complete the task entirely.
For the better part of the twentieth century, the fields of psychology, psychiatry, and special education viewed the human mind through a singular, monolithic lens. The scientific consensus held that there was only one "typical" operating system for human cognition, and any significant deviation from that dominant societal norm was categorized as a malfunction, deficit, or disorder that required a cure 12.
The concept of neurodiversity actively dismantles this assumption. The term was originally coined in the late 1990s by Australian sociologist Judy Singer, who drew direct inspiration from the environmental and biological concept of biodiversity 34. Ecological science dictates that a healthy, resilient ecosystem requires a vast array of flora and fauna to survive environmental shifts. Singer and other early advocates proposed that human society operates on the same principle: cultural and systemic stability requires a repository of different cognitive types 345.
Some human brains are naturally optimized for intense hyper-focus and complex pattern recognition, while others excel at rapid context-switching, profound creative leaps, or heightened sensory awareness 67.
Navigating the Terminology
Because the terminology surrounding this topic evolved in grassroots advocacy spaces rather than formal clinical laboratories, definitions are frequently misunderstood. A critical point of clarification is that neurodiversity encompasses the entirety of the human race. Because no two nervous systems on the planet are exactly identical, humanity as a whole is neurodiverse 38. It is grammatically and scientifically incorrect to refer to a single individual as "neurodiverse" 3.
When referring to specific individuals whose brain function diverges significantly from the dominant societal norms, the correct nomenclature is neurodivergent 89. This term was introduced in the year 2000 by activist Kassiane Asasumasu to serve as a broad, inclusive umbrella 9. The neurodivergent spectrum includes a wide array of cognitive profiles, incorporating autism, attention-deficit/hyperactivity disorder (ADHD), dyslexia, dyspraxia, dyscalculia, Tourette's syndrome, and various sensory processing and mental health conditions 910. Conversely, individuals whose cognitive functioning aligns with expected societal baselines are referred to as neurotypical 911.
The origins of the movement are not without contemporary controversy. While Judy Singer is widely credited as the "mother of neurodiversity," recent letters published in the journal Autism by early activists, including Martijn Dekker, have contested her sole ownership of the concept. These academics argue that the paradigm was collectively forged in the mid-1990s on early internet forums like Independent Living on the Autistic Spectrum (InLv), and have distanced the movement from Singer following her recent controversial statements regarding the transgender community 1011. Despite these ideological fractures, the core premise of the movement - shifting away from pure pathology - remains intact.
The Three Lenses of Disability and Difference
To fully comprehend how a clinical diagnosis operates in opposition to the neurodiversity movement, it is necessary to examine the three distinct paradigms used by researchers, clinicians, and sociologists to understand human disability 12814.
The Medical Model
The traditional medical model, also referred to as the pathology paradigm, asserts that disability is a defect located entirely inside the individual's biology 81412. Under this framework, there is a distinct, healthy way for a human mind to function, and any significant deviation indicates an illness or disorder 1. The ultimate goal of the medical model is clinical intervention: to cure, treat, or minimize symptoms so the individual can assimilate seamlessly into society 1412. The language used by this model is inherently deficit-based, utilizing terms like impairment, dysfunction, and abnormality 216.
The Social Model of Disability
Emerging from the disability rights activism of the 1960s and 1970s, the social model radically relocates the source of disability 89. This framework argues that individuals are not disabled by their physical or cognitive differences, but rather by an environment that is exclusively designed for the majority 141613. For example, a person who uses a wheelchair is not disabled by their paralysis; they are disabled by a society that constructs buildings entirely out of stairs 816. The solution, therefore, is not to medically "fix" the person, but to fundamentally alter societal expectations and physical infrastructure to remove barriers 14.
The Neurodiversity Paradigm
Championed by scholars such as Dr. Nick Walker, the neurodiversity paradigm functions as an evolution of the social model 112. It accepts that neurological variations are a natural, neutral reality. It aligns heavily with the social model by arguing that systemic barriers, rigid educational standards, and a lack of workplace accommodations cause massive disablement for neurodivergent people 112. However, unlike a strict interpretation of the social model, the neurodiversity paradigm acknowledges the complex reality that certain neurodivergent traits can be inherently disabling regardless of societal structure, and that medical treatments can still be highly beneficial for improving a person's quality of life 1413.
| Feature | The Medical (Pathology) Model | The Social Model | The Neurodiversity Paradigm |
|---|---|---|---|
| Location of the "Problem" | Inside the individual's brain, biology, or genetics. | In the environment, societal attitudes, and systemic barriers. | In the mismatch between the individual's natural needs and the environment. |
| Core Assumption | There is a "normal" baseline; deviation is a malfunction. | Disability is entirely a social construct created by lack of access. | Brain variation is a natural, valuable part of human biodiversity. |
| Primary Goal | To cure, treat, medicate, or mask symptoms to achieve normalcy. | To change society, eliminate barriers, and provide equality. | To support, accommodate, and respect the individual's operating system. |
| Diagnostic Terminology | Disorder, Deficit, Impairment, Symptom, Treatment. | Barrier, Accessibility, Accommodation, Exclusion. | Neurodivergent, Neurotypical, Neuro-affirming, Natural variation. |
Table 1: A comparative analysis of the three primary frameworks utilized to define and address cognitive differences and disability 1281413.
The Mechanics of a Clinical Diagnosis
While "neurodivergent" serves as a community-based identity and an analytical framework, a clinical diagnosis remains a highly specific, standardized medical classification 714.
In the medical and psychiatric communities, diagnoses for conditions like autism or ADHD are strictly governed by diagnostic manuals, most notably the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) and the World Health Organization's International Classification of Diseases (ICD-11) 151617. The DSM-5-TR, updated as recently as 2022, dictates precise criteria that must be met for a clinician to issue a formal medical label 17.
The defining characteristic that separates natural neurodivergence from a clinical disorder is the threshold of significant functional impairment 1517.
An individual may possess a nervous system that processes sensory input intensely, or they may possess executive functioning traits characteristic of ADHD. However, under the strict guidelines of the DSM-5-TR and ICD-11, if that individual has developed sufficient coping mechanisms to maintain employment, navigate social relationships, and avoid severe psychological distress, a clinician will determine that their traits do not cause enough impairment to warrant a medical diagnosis 1517.
This creates a fascinating clinical paradox. Two individuals can share nearly identical neurocognitive profiles and genetic predispositions. If one is situated in a highly supportive, neuro-affirming environment that capitalizes on their strengths, they may never cross the clinical threshold for a diagnosis 15. Conversely, if the other individual is subjected to chronic stress, trauma, or an unaccommodating environment, their coping mechanisms will eventually fail, triggering the functional impairment required to be diagnosed with a "disorder" 1315.
The Utility and Limitations of Medical Labels
Despite the inherent limitations and deficit-based language of the medical model, obtaining a formal clinical diagnosis remains a crucial milestone for many.
First and foremost, a medical diagnosis is almost universally required by global healthcare systems and insurance providers to access targeted therapies, specialized occupational support, or vital pharmaceutical interventions 1819. Beyond the bureaucratic utility, a formal diagnosis often provides profound psychological relief. It offers an individual a scientific framework to contextualize a lifetime of perceived failures, validating their experiences and enabling them to connect with established communities 18.
However, leading psychiatric research in 2024 and 2025 has begun exposing the limitations of rigid clinical categorizations. Researchers, including international groups led by experts like Dr. Giorgia Michelini, are increasingly pushing for "transdiagnostic frameworks" 16. This approach acknowledges that approximately 15% of the global population is neurodivergent, and these individuals frequently exhibit traits from multiple DSM-5 categories simultaneously 16. Autism, ADHD, dyslexia, and co-occurring mental health conditions like depression and anxiety share significant biological and behavioral overlap. Categorizing them into entirely distinct, siloed "labels" overlooks their shared characteristics and the complex interplay of human cognition 16.
The Self-Identification Debate and Epistemic Injustice
As public awareness of neurodiversity has expanded, one of the most fiercely debated topics within the psychiatric community is the rapid rise of self-identification (often colloquially referred to as self-diagnosis) 2021. Increasingly, adults are researching neurocognitive profiles, recognizing their lived experiences in the clinical criteria, and adopting labels like "autistic" or "ADHD" without ever consulting a physician 20.
From a traditional psychiatric standpoint, this trend presents serious concerns. Critics within the medical establishment argue that self-identification risks diluting formal diagnoses and lacks the rigorous differential testing that a trained medical professional provides 2021. Diagnosticians are trained to rule out overlapping conditions - such as distinguishing whether an inability to focus is caused by ADHD, clinical burnout, or an undiagnosed mood disorder 2122.
Conversely, advocates argue that self-identification is not a fleeting trend, but a necessary survival strategy in the face of fundamentally broken healthcare systems 2021. The clinical diagnostic pathway is currently obstructed by severe bottlenecks, including multi-year waiting lists for adult assessments 23. In nations without universal healthcare, comprehensive psychological evaluations can cost thousands of dollars, rendering formal diagnoses inaccessible to lower-income demographics 2324.
Furthermore, historical diagnostic criteria were largely derived from observations of young, white males. Consequently, women, people of color, and high-masking individuals - those who consciously or subconsciously suppress their natural behaviors to blend into neurotypical society - are routinely misdiagnosed with personality or mood disorders due to clinician bias and outdated stereotypes 20.
Within this context, the dismissal of self-identification is analyzed by sociologists as a form of epistemic injustice 202526. Drawing on the philosophical framework established by Miranda Fricker, epistemic injustice occurs when an individual is wronged in their capacity as a knower 26. When the medical establishment dismisses a neurodivergent person's intimate knowledge of their own internal brain function simply because they lack formal medical credentials, it invalidates their lived reality 2526. This dynamic is further exacerbated by the "double empathy problem," a theory positing that communication breakdowns occur not because neurodivergent people lack empathy, but because neurotypical and neurodivergent individuals naturally utilize fundamentally different styles of socialization and communication 920.
The Dangers of Algorithmic Self-Diagnosis
While deep, thoroughly researched self-identification can be a valid emancipatory tool, the explosive growth of mental health content on platforms like TikTok, Instagram, and Reddit has introduced immense risks 222728.
The algorithms driving social media platforms are optimized to deliver highly relatable, frictionless content. A sixty-second video might present universal human experiences - such as "feeling overwhelmed by loud noises," "procrastinating on difficult tasks," or "having niche hobbies" - as definitive clinical symptoms of autism or ADHD 222728.
The consequences of algorithmic self-diagnosis are statistically alarming: * High Error Rates: Research conducted by the Harvard Petrie-Flom Center in 2025 demonstrated that individuals are between 5 and 11 times more likely to incorrectly self-diagnose their mental health condition via social media than they are to accurately identify it 22. * Clinical Inaccuracy: Peer-reviewed analyses have concluded that approximately 80% of mental health content circulated on TikTok is either highly misleading or entirely clinically inaccurate 22. * Treatment Delays: When users incorrectly self-diagnose based on superficial algorithms, they often cease pursuing professional evaluations. This delays accurate interventions for serious, sometimes life-threatening conditions that share overlapping symptoms but require vastly different clinical treatments 2228.
Educational Classifications: Why a Doctor's Note Isn't Enough
The disparity between medical reality and administrative categorization becomes painfully apparent when neurodivergent children enter the public education system 2934.
A widespread misconception among parents is that securing a formal clinical diagnosis of autism or ADHD from a neurologist will automatically guarantee their child special education services. Under United States federal law, specifically the Individuals with Disabilities Education Act (IDEA), this assumption is false 293430.
There is a stringent legal boundary between a medical diagnosis and an educational classification 1936.
To qualify for an Individualized Education Program (IEP), a student must fit into one of the 13 specific disability categories defined by IDEA 2931. The most common category is Specific Learning Disability (SLD), encompassing dyslexia and dyscalculia, followed closely by Speech or Language Impairments, Other Health Impairments (OHI, which typically covers ADHD), and Autism Spectrum Disorder 31.
However, possessing a medical diagnosis is merely one piece of the puzzle. The critical legal hurdle for IEP eligibility is the "adverse effect" clause 293431. The school's multidisciplinary team must definitively prove that the child's disability adversely affects their educational performance and that they specifically require specialized instruction to succeed 293430.
| Medical Diagnosis | Educational Classification (IEP Eligibility) | |
|---|---|---|
| Who conducts the assessment? | A licensed clinical professional (Psychiatrist, Neurologist, Clinical Psychologist) 1938. | A multidisciplinary school team (Special Educators, School Psychologists, Speech Therapists, Parents) 3832. |
| What criteria is utilized? | Standardized clinical manuals such as the DSM-5-TR or ICD-11 1932. | Federal legislation (IDEA) and specific state-level educational guidelines 3431. |
| What is the primary focus? | Identifying functional impairment and clinical presentation across all areas of daily life 1936. | Determining if the condition significantly impedes academic progress and functional performance specifically within the school environment 3036. |
| What services does it unlock? | Medical interventions, behavioral therapies, pharmaceutical prescriptions, and insurance coverage 1932. | Legally binding specialized instruction, classroom modifications, and occupational/speech therapy delivered during school hours 3432. |
Table 2: An analysis of the differing requirements and outcomes between acquiring a medical diagnosis versus securing an educational classification in the US public school system 1934303632.
If a child has a documented clinical diagnosis of autism but is earning proficient grades, reading at grade level, and navigating the social dynamics of the classroom without significant disruption, the educational team may legally determine that the autism does not adversely affect their schooling 2930. Consequently, the child will be denied an IEP. They may, however, still qualify for a 504 Plan under the Rehabilitation Act of 1973, which provides essential civil rights accommodations (such as extended testing time or permissible sensory breaks) but does not alter the curriculum or provide specialized instruction 33.
Conversely, public schools do not possess the medical authority to formally diagnose a child 1930. While a school psychologist can determine that a student meets the educational criteria for an autism classification to receive classroom services, this educational label cannot be used to bill health insurance for outside medical therapies 1930.
Workplace Rights and Accommodations in 2025
When neurodivergent individuals transition from the education system into the workforce, the tension between self-identification, clinical proof, and legal protections undergoes yet another transformation.
Under legislation such as the Americans with Disabilities Act (ADA) in the United States, or the Equality Act 2010 in the United Kingdom, employers are legally obligated to provide "reasonable accommodations" to qualified individuals to assist them in performing their essential job functions 344243. Historically, accessing these accommodations involved an invasive human resources protocol requiring extensive medical documentation to "prove" the severity of a clinical diagnosis 43.
However, recent legal precedents in 2025 have begun reshaping the corporate landscape. A landmark decision by the Second Circuit Court of Appeals (Tudor v. Whitehall Central School District) dramatically clarified how the ADA applies to high-functioning neurodivergent employees 424445. The court ruled that an employee does not need to prove that an accommodation is strictly necessary to perform their job duties; they only need to demonstrate that the request is reasonable 4244. The ruling recognized that the ADA protects employees who can perform their jobs "with or without" accommodation 4445. Therefore, if an autistic employee can technically execute their job without noise-canceling headphones - but doing so causes extreme sensory exhaustion and burnout - they are still legally entitled to the accommodation to enhance their general job performance 4445.
Simultaneously, the Fourth Circuit Court of Appeals (Tarquinio v. Johns Hopkins University) established clear boundaries regarding the "interactive process" 46. While employers must accommodate known disabilities, if a neurodivergent limitation is not patently obvious, the employer retains the right to request reasonable medical documentation 46. If the employee refuses to participate in this interactive process or declines to provide basic verification, they forfeit their ADA protections 46. Furthermore, modifications to other federal laws, such as the Pregnant Workers Fairness Act (PWFA), have demonstrated a shift toward accommodations for "known limitations" without requiring a threshold level of severe impairment, indicating a broader legal trend toward functional support over strict diagnostic pathology 47.
Despite these strengthening legal frameworks, the psychological reality for neurodivergent professionals remains fraught with anxiety and systemic barriers.
Data extracted from the 2025 "Neurodiversity at Work" survey, conducted by Understood.org and The Harris Poll, illuminates a severe disconnect between policy and culture 2435.
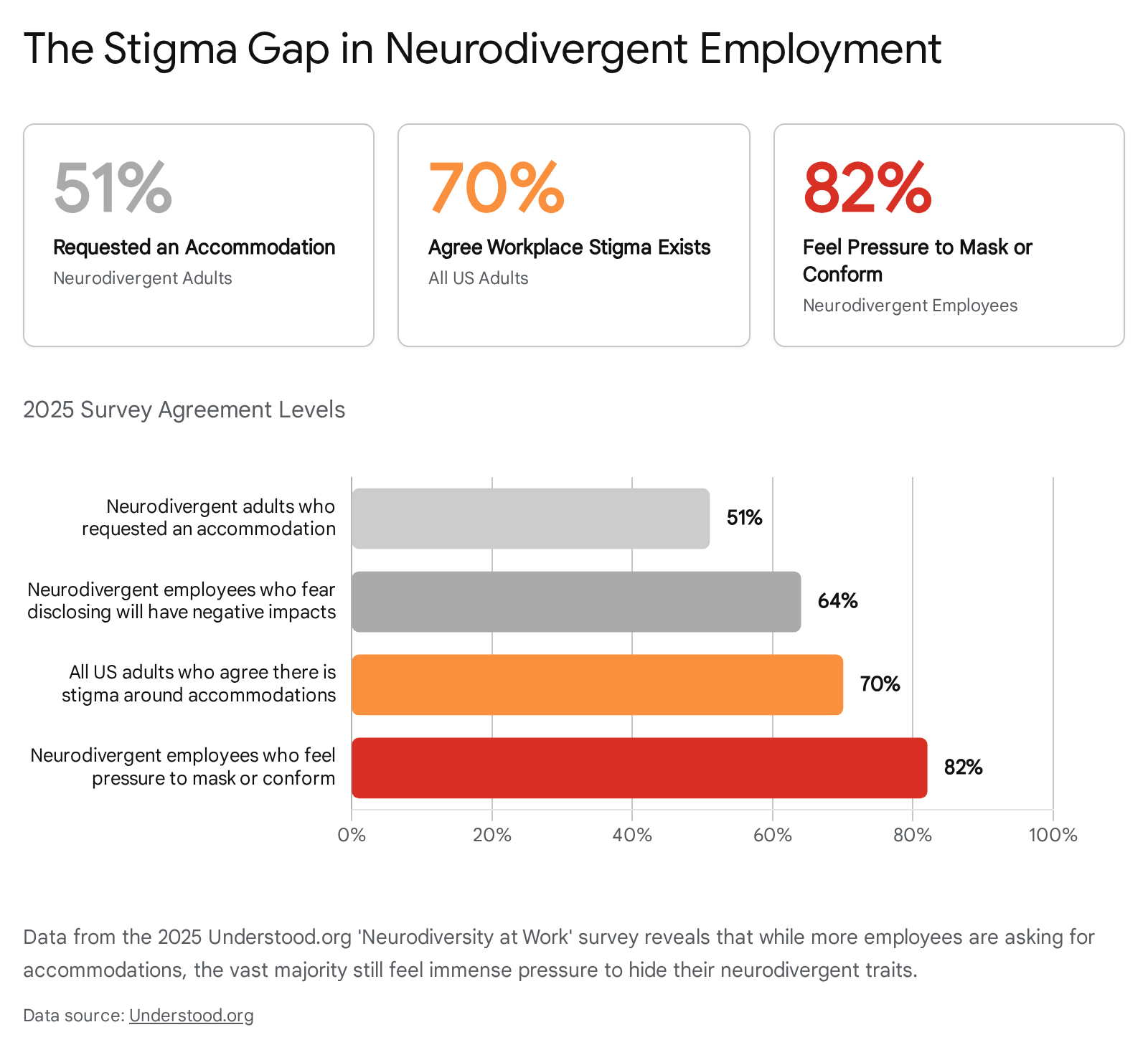
While advocacy is rising - with a record 51% of neurodivergent adults actively requesting workplace accommodations - an overwhelming 82% reported feeling intense pressure to "mask" their natural behaviors to conform to neurotypical expectations 35. Furthermore, 64% of neurodivergent employees admitted they were terrified that formally disclosing their condition to human resources would trigger negative professional repercussions, and 53% suspect that corporate neurodiversity programs are implemented purely for public relations optics 35.
In response to this persistent stigma, forward-thinking organizations are pioneering new methodologies. The UK's Advisory, Conciliation and Arbitration Service (ACAS) issued updated 2025 guidelines advocating for "trust-based" approaches to neuroinclusion 34. Rather than demanding complex clinical evidence to supply a modified keyboard, flexible scheduling, or noise-canceling headphones, managers are encouraged to provide these adjustments based purely on an employee's self-identified functional needs 34. This performance-focused approach bypasses the medical bottleneck, treating accommodations as standard productivity tools rather than remedial interventions for a disorder 34.
A Global Perspective: Neurodiversity Beyond the West
It is imperative to recognize that the tension between the neurodiversity paradigm and clinical diagnostics is deeply rooted in Western sociological frameworks. As these concepts export globally, they intersect with vastly different cultural, religious, and economic realities 363751.
In Brazil, the discourse around neurodiversity is currently undergoing a rapid transformation. Activist movements, significantly led by autistic self-advocates, have established initiatives like the Pacto pela Neurodiversidade to challenge the dominant biomedical perspective that pathologizes disability 52. Despite public support for inclusive education, the reality within the Brazilian public healthcare system (SUS) reveals deep systemic challenges. Referrals to neuropediatric facilities are frequently delayed, with many educators and clinicians lacking the training to recognize early developmental divergence, leading to an over-reliance on medicalized interventions rather than proactive academic support 3854.
Conversely, the Middle East is demonstrating how neuro-inclusive policies can be instituted via top-down government mandates. The United Arab Emirates (UAE) has embedded inclusion directly into national strategies, completely reimagining the terminology 5556. By officially designating individuals with disabilities as "People of Determination," the UAE actively seeks to strip away deficit-based stigma 5539. Policies like the Dubai Inclusive Education Policy Framework legally mandate that all private schools must admit and provide equitable environments for neurodivergent students, resulting in a staggering 116% increase in the enrollment of students with additional educational needs in Abu Dhabi between 2023 and 2024 555640. However, researchers note that across the broader Arab world, challenges remain regarding social isolation and the need for culturally sensitive mental health support for caregivers 4142.
In regions of Africa and Asia, the paradigm shift faces profound cultural hurdles. In Nigeria, clinical diagnostic services are exceptionally scarce, and neurodivergent traits - such as the hyperactivity seen in ADHD or the communication differences in autism - are frequently misattributed to poor parenting, moral failings, or spiritual interference 4362. This can result in families pursuing traditional deliverance rituals rather than evidence-based support 43. Yet, significant progress is underway; the inaugural 2026 National Inclusion Conference spearheaded by the International Forum of Inclusion Practitioners (IFIP) aims to dismantle these stigmas and train Nigerian educators in practical, neuro-affirming classroom strategies 44.
Similarly, in countries like India, China, and Japan, the concept of neurodiversity must navigate cultural systems that highly prioritize social harmony and conformity over individual uniqueness 5145. While collectivist cultures have historically fostered strong extended-family care structures for neurodivergent individuals, avoiding the institutionalization seen in the early 20th-century West, the stigma surrounding formal mental health diagnoses remains potent 3645. Progress is currently highly bifurcated; while multinational technology corporations in urban centers like Bangalore are launching specialized hiring initiatives to recruit neurodivergent data analysts, rural populations continue to lack access to basic developmental screening 51.
Bottom line
Neurodiversity is the biological reality that human brains naturally vary in how they process information, socialize, and learn, suggesting that these differences should be accommodated rather than cured. A clinical diagnosis is a specific, standardized medical tool used to identify when these natural variations cause significant functional impairment, remaining essential for unlocking vital therapies, pharmaceutical interventions, and legal protections. As the global neurodiversity movement gains momentum, society is slowly shifting from a rigid medical model toward a framework that supports individuals based on their functional needs and self-identified lived experiences. What remains an ongoing challenge is how quickly heavily regulated systems - from public education to corporate human resources - can adapt their legal and administrative structures to foster true inclusion without demanding pathology.