Who Qualifies for the $50 Medicare GLP-1 Bridge in 2026
The Medicare GLP-1 Bridge is a temporary federal pilot program running from July 1, 2026, through December 31, 2027, that caps out-of-pocket costs for specific FDA-approved weight-loss medications at $50 per month. To qualify, Medicare beneficiaries must be enrolled in a Part D prescription plan, meet strict Body Mass Index (BMI) and health criteria, and secure a prior authorization from a centralized processor rather than their standard insurance plan. The program covers the injectable medications Wegovy and Zepbound, alongside the newly approved once-daily pill, Foundayo.
What Is the Medicare GLP-1 Bridge?
Historically, the federal government has been strictly barred by a long-standing statute from covering medications prescribed solely for anorexia, weight loss, or weight gain under Medicare 12145. This statutory exclusion left millions of seniors and disabled beneficiaries paying entirely out of pocket for popular and highly effective glucagon-like peptide-1 (GLP-1) receptor agonists 1. Without insurance, these revolutionary treatments can cost anywhere from $149 to well over $1,000 per month, forcing many patients to ration doses or abandon treatment entirely 2628.
To bypass this statutory ban without waiting for complex Congressional legislation, the Centers for Medicare & Medicaid Services (CMS) invoked a Section 402 demonstration authority 123. Section 402 allows the government to test novel approaches to healthcare delivery, premium stabilization, and drug pricing without formally amending statutory coverage rules 12.
The resulting initiative is the Medicare GLP-1 Bridge 4. Beginning July 1, 2026, CMS will provide eligible Medicare Part D beneficiaries with early access to evidence-based weight-loss medications at a predictable $50 monthly copay 41112. Under this framework, CMS has directly negotiated a net price of $245 per monthly supply with participating drug manufacturers 1235. The patient pays $50 at the pharmacy counter, and the remaining costs are managed by a central processor 5146. This structure allows CMS to collect vital utilization data and provide immediate financial relief to patients without exposing standard Medicare Part D plan sponsors to the financial risk of these expensive therapies 5616.
The Policy Landscape: Why Is Coverage Changing Now?
The path to covering GLP-1s in Medicare has been politically fraught and economically complex. In late 2025, the proposed contract year 2026 Medicare Advantage and Part D rule included sweeping provisions that would have formally expanded coverage to weight loss medications for all Medicare and Medicaid beneficiaries dealing with obesity 124.
However, the Congressional Budget Office (CBO) published a report in October 2024 analyzing the massive economic impact of such a change, concluding that covering GLP-1 drugs for obesity would cost the Medicare program an estimated $35 billion between 2026 and 2034 4. Fearing premium spikes and budget destabilization, the final CY 2026 MA and Part D rule ultimately removed these broad coverage provisions 12.
To soften the blow of this reversal, the Trump administration announced an alternative strategy in November 2025. They unveiled agreements with the manufacturers of brand-name GLP-1 products to reduce consumer prices through a new direct-to-consumer platform known as TrumpRx, while simultaneously initiating the Medicare GLP-1 Bridge and the multi-year BALANCE Model demonstration projects 124. This policy pivot represents a significant departure from the government's historical stance, aiming to balance the undeniable clinical benefits of obesity treatment with the severe fiscal constraints of the Medicare program 124.
Which Weight Loss Medications Are Covered?
The GLP-1 Bridge program covers three specific FDA-approved GLP-1 medications when prescribed for chronic weight management. The program is exclusive to these branded therapies; it currently excludes older weight-loss drugs like phentermine-topiramate (Qsymia) or naltrexone-bupropion (Contrave) 31117.
1. Foundayo (orforglipron)
Approved by the FDA on April 1, 2026, Foundayo represents a major technological leap in obesity treatment 7891022. Manufactured by Eli Lilly, Foundayo is an oral glucagon-like peptide-1 (GLP-1) receptor agonist 710. However, unlike earlier pill-based treatments, its active ingredient, orforglipron, is a small-molecule, non-peptide compound 7891023.
Peptide-based drugs are highly unstable in the acidic environment of the human stomach and require strict fasting protocols to be absorbed properly 889. Foundayo's non-peptide structure solves this problem. It can be taken once a day at any time, with or without food, and without strict water limitations, offering unprecedented flexibility for patients 878911.
The FDA approval of Foundayo was heavily supported by the ATTAIN clinical trial program 1023. In the ATTAIN-1 trial, which evaluated adults with obesity but without diabetes, participants taking the highest dose of Foundayo (17.2 mg) and completing the trial lost an average of 12.4% of their baseline body weight (an average of 27.3 pounds) over 72 weeks, compared to just 0.9% in the placebo group 891012. When looking at all participants regardless of whether they completed the full trial, the average weight loss was 11.1% (25 pounds) 710.
Like other GLP-1s, Foundayo works by binding to receptors in the brain to reduce hunger, increase feelings of fullness, and slow gastric emptying 7810. It does carry standard class warnings, including a boxed warning for the potential risk of thyroid C-cell tumors, alongside monitoring requirements for gastrointestinal distress, acute kidney injury, and pancreatitis 71023. All dosage formulations of Foundayo (from 0.8 mg up to 17.2 mg) are fully covered under the Bridge program 3782226.
2. Wegovy (semaglutide)
Manufactured by Novo Nordisk, Wegovy is covered under the Bridge in both its traditional once-weekly injectable form and its daily oral tablet form 23115. Its active ingredient, semaglutide, has a long track record of safety and efficacy, and is identical to the ingredient used in the diabetes drug Ozempic 81782713.
In pivotal clinical trials (such as the STEP 1 trial), injectable Wegovy demonstrated an average body weight reduction of approximately 14.9% to 15% over 64 to 71 weeks 17927. The newer daily oral version of Wegovy, which was approved in late 2025, showed similar or slightly superior efficacy, with the OASIS clinical trial demonstrating up to 16.6% average weight loss 17927. In addition to weight reduction, Wegovy carries secondary FDA approvals for reducing the risk of major adverse cardiac events and treating non-cirrhotic metabolic dysfunction-associated steatohepatitis (MASH) 17.
Despite the convenience of a pill, the oral formulation of Wegovy is a modified protein (peptide) and remains notoriously difficult for the body to absorb 889. It requires strict morning fasting: it must be taken on an empty stomach with no more than four ounces of water, and the patient must wait at least 30 minutes before eating, drinking, or taking any other medications 8892713.
3. Zepbound (tirzepatide)
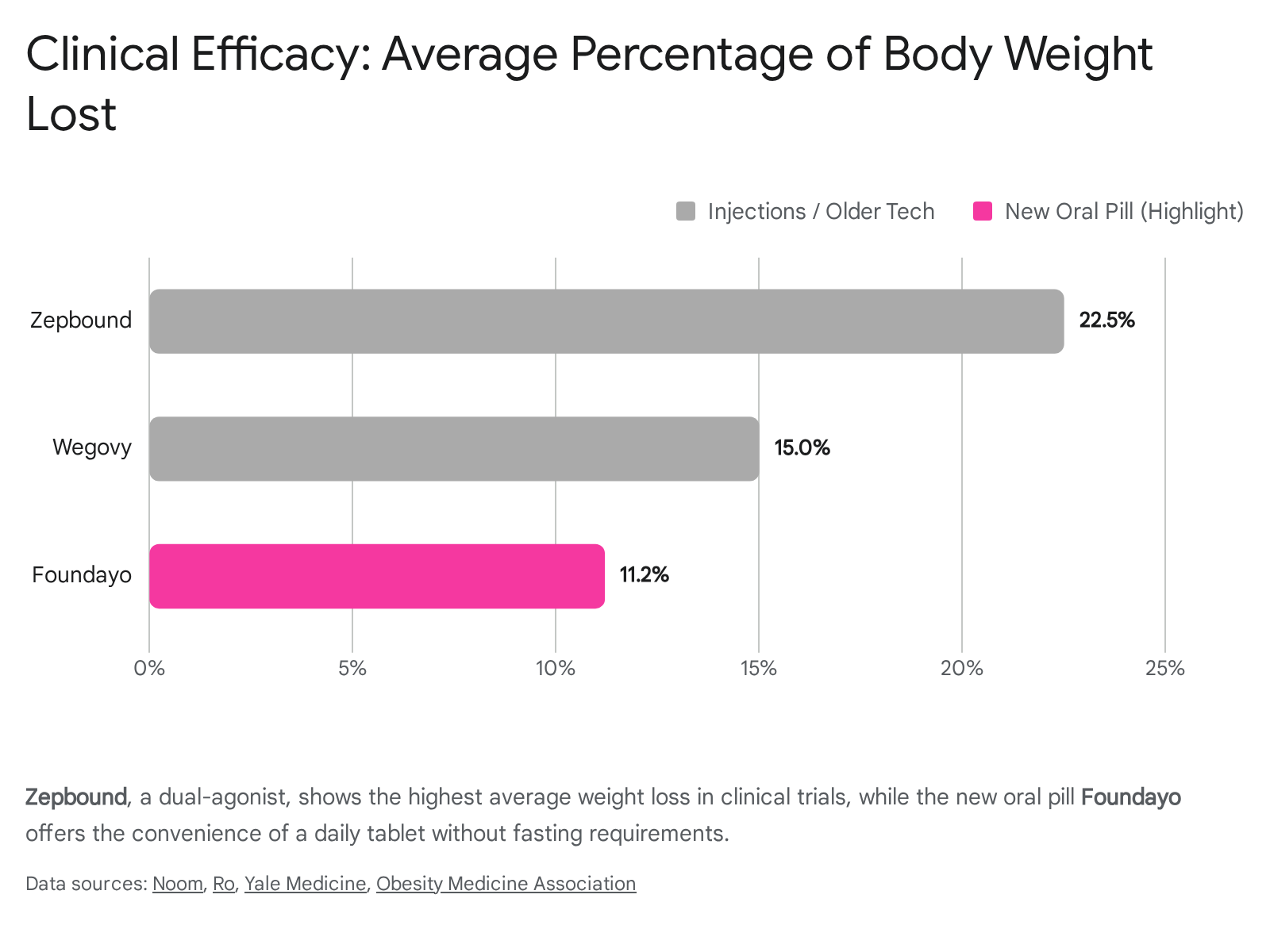
Eli Lilly's injectable Zepbound uses the active ingredient tirzepatide (the same compound used in the diabetes medication Mounjaro) 1781227. Zepbound is unique among the Bridge-covered drugs because it is a dual agonist; it mimics both GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) 17912. By targeting two distinct appetite-regulating hormone pathways simultaneously, Zepbound currently boasts the highest average weight loss among approved anti-obesity medications 1217912.
In the landmark SURMOUNT-1 clinical trial, adults with obesity taking tirzepatide achieved an average body weight reduction of between 15% and 22.5% over 72 weeks, depending on the dosage 1712.
Crucial restriction: Under the Medicare GLP-1 Bridge, only the KwikPen formulation of Zepbound is eligible for the $50 copay 32614. The single-dose vial and standard single-dose pen formulations of Zepbound are strictly excluded from the demonstration program 32614.
Medication Comparison Summary
The table below summarizes the key features, administration routes, and clinical trial efficacy benchmarks for the medications included in the Medicare GLP-1 Bridge.
| Feature | Foundayo | Wegovy | Zepbound |
|---|---|---|---|
| Active Ingredient | Orforglipron | Semaglutide | Tirzepatide |
| Manufacturer | Eli Lilly | Novo Nordisk | Eli Lilly |
| Formulation | Daily Oral Tablet | Weekly Injection & Daily Tablet | Weekly Injection (KwikPen only) |
| Mechanism | GLP-1 agonist | GLP-1 agonist | GLP-1/GIP dual agonist |
| Fasting Required? | No | Yes (for pill formulation) | No (injection) |
| Average Weight Loss | ~11.1% - 12.4% (at 72 weeks) | ~14% - 16.6% (at 64-71 weeks) | ~15% - 22.5% (at 72 weeks) |
| Bridge Eligibility | All tablet formulations | Injection and tablet formulations | KwikPen formulation only |
Note: Efficacy percentages are derived from varied clinical trials (ATTAIN, STEP/OASIS, and SURMOUNT programs) and are heavily dependent on dosage, patient adherence, and lifestyle modifications 831778910221227.
Who Qualifies for the $50 Copay?
Not every Medicare beneficiary can access the GLP-1 Bridge. The program operates with highly specific enrollment boundaries and clinical criteria that are notably more restrictive than general FDA prescribing labels 31230.
1. Medicare Plan Requirements
To qualify, a patient must be actively enrolled in a qualifying Medicare prescription drug plan for the 2026 calendar year 311530. Eligible plans include: * Standalone Medicare Part D Prescription Drug Plans (PDPs) 3115141430. * Medicare Advantage coordinated care plans that include prescription drug coverage (MA-PDs), such as HMOs and PPOs 3115141430. * Special Needs Plans (SNPs) and the Limited Income Newly Eligible Transition (LI NET) program 31151614. * Employer/union group waiver plans (EGWPs) 31114.
Certain specialized plan types are explicitly excluded. Beneficiaries enrolled in private fee-for-service plans, section 1876 cost contract plans, PACE organizations, or religious fraternal benefit plans cannot participate unless they simultaneously carry a standalone PDP 3. Furthermore, TRICARE For Life beneficiaries are only eligible if they are cross-enrolled in an eligible Medicare Part D plan and successfully meet all clinical prior authorization criteria 3.
2. Strict Clinical and BMI Criteria
You must be at least 18 years old, and your healthcare provider must attest that the medication is being prescribed specifically to reduce excess body weight and maintain weight reduction in combination with ongoing lifestyle modifications, such as structured nutrition and physical activity 3121414.
Furthermore, a physician must verify that the patient met one of three specific Body Mass Index (BMI) tiers.
| Eligibility Tier | BMI Requirement | Additional Health Condition Required |
|---|---|---|
| Tier 1 | BMI of 35 or higher | None required. |
| Tier 2 | BMI of 30 or higher | Must have a diagnosed history of: heart failure with preserved ejection fraction (HFpEF), uncontrolled hypertension, OR chronic kidney disease (stage 3a or above). |
| Tier 3 | BMI of 27 or higher | Must have a diagnosed history of: pre-diabetes, previous heart attack (myocardial infarction), previous stroke, OR symptomatic peripheral artery disease. |
Source: CMS Medicare GLP-1 Bridge Provider Guidelines 13125141415.
The "Lookback" Rule: A critical and highly beneficial feature of the program is that the BMI criteria apply to the moment the patient first initiated GLP-1 therapy, rather than their current weight 31414. For example, if a patient began taking Wegovy out-of-pocket in September 2024 with a starting BMI of 37, but their current BMI has dropped to 34 by the time of their July 2026 prior authorization request, they still fully qualify 314. The prescribing provider simply attests to the original BMI at the time therapy was initiated, ensuring that patients are not financially punished for successfully losing weight prior to the Bridge's launch 31414.
3. Excluded Diagnoses
The Medicare GLP-1 Bridge is exclusively designed to cover medications prescribed for weight management 31414. If a beneficiary requires a GLP-1 medication to treat Type 2 diabetes, obstructive sleep apnea, or noncirrhotic metabolic dysfunction-associated steatohepatitis (MASH), they cannot use the GLP-1 Bridge 1431214.
This is because standard Medicare Part D plans are already legally permitted - and routinely expected - to cover GLP-1s for these specific, FDA-approved non-weight-loss indications 14314. Patients with these conditions must obtain their prescriptions through their normal Part D benefit flow, paying whatever formulary copay or coinsurance their specific insurance plan dictates. Even if that standard Part D copay is higher than $50, the patient is locked out of the Bridge program 1314.
Financial Mechanics: How the $50 Copay Works (and the TrOOP Catch)
When a prior authorization is approved, the beneficiary's out-of-pocket cost is strictly capped at $50 for a 30-day supply of the medication 2634111416. Patients cannot stack additional manufacturer coupons, savings cards, or secondary discounts to lower this $50 copay any further 14.
However, the financial mechanics of this program come with a significant structural catch that beneficiaries must fully understand: The Medicare GLP-1 Bridge operates entirely outside of the standard Medicare Part D benefit structure 1562311562616.
Because the program is an experimental Section 402 demonstration, the financial claims bypass your private insurance company entirely 565146. Instead, CMS uses a single, centralized processor (contracted through Humana) to adjudicate the claims and pay the dispensing pharmacies directly 611514614. At the pharmacy counter, the patient pays the $50 copay, and the central processor reimburses the pharmacy for the remainder of the $245 negotiated wholesale acquisition cost (plus a standard dispensing fee) 123514.
Because this money never flows through your Part D plan's accounting systems, patients face three distinct financial consequences:
- No Deductible Assistance: The $50 you spend each month on Wegovy, Zepbound, or Foundayo will not count toward satisfying your annual Part D deductible 1311151633.
- No TrOOP Accumulation: Neither the $50 copay nor the $245 net cost of the drug counts toward your True Out-Of-Pocket (TrOOP) spending or your gross covered prescription drug costs (GCPDC) 1311516. In 2026, standard Part D plans feature a $2,100 annual out-of-pocket spending cap; money spent in the Bridge program will not help you reach that protective limit 1111533.
- No "Extra Help" Subsidies: If you are a low-income senior who qualifies for the Part D Low-Income Subsidy (LIS) program - commonly known as Extra Help - you cannot apply those federal subsidies to Bridge prescriptions 31116. You will still be required to pay the full, unsubsidized $50 copay 31116.
Despite these limitations, the flat $50 rate remains consistent regardless of which phase of the Part D benefit (such as the coverage gap or catastrophic phase) the beneficiary is currently traversing for their other medications 3.
The Prior Authorization Process for 2026
Beneficiaries cannot enroll themselves directly into the Bridge program; the application process relies entirely on active coordination by medical providers 1130.
1. Wait for the Launch Date: The program does not formally begin until July 1, 2026. Providers are instructed not to submit any paperwork early, as prior authorization requests will not be accepted, queued, or processed before that date 314.
2. Provider Submission: To initiate coverage, a medical provider must submit both a valid prescription and a specific prior authorization request directly to the CMS central processor 3514. Providers can submit this documentation electronically - which CMS strongly encourages to prevent backlogs - or via a standardized fax form that will be published in June 2026 314.
3. Minimal Provider Friction: CMS has intentionally removed barriers for physicians. A doctor does not need to be formally enrolled as a Medicare provider to write a Bridge prescription or submit a prior authorization request 1214. The only restriction is that the prescribing provider must not be listed on the federal Medicare Preclusion List 14.
4. Plan Independence: Because the central processor handles the claims, your specific Part D insurance sponsor does not need to "opt in" or assume any risk for you to gain access 621156. If a standard Part D plan inadvertently receives a prior authorization request for a weight-loss medication covered under the Bridge, CMS guidelines mandate that the plan immediately direct the provider to reroute the request to the central processor 5.
For patients who are currently rationing doses due to high cash-pay costs, healthcare advocates and clinic navigators strongly suggest consulting with doctors well before the July 1 launch 61130. Gathering baseline BMI records, confirming cardiovascular comorbidities, and preparing the necessary attestation paperwork early will be critical for avoiding administrative bottlenecks when the central processor portal opens 61130.
The BALANCE Model: What Happens in 2028?
The program is officially designated as a "Bridge" because it serves as a temporary, 18-month stopgap 16211514634.
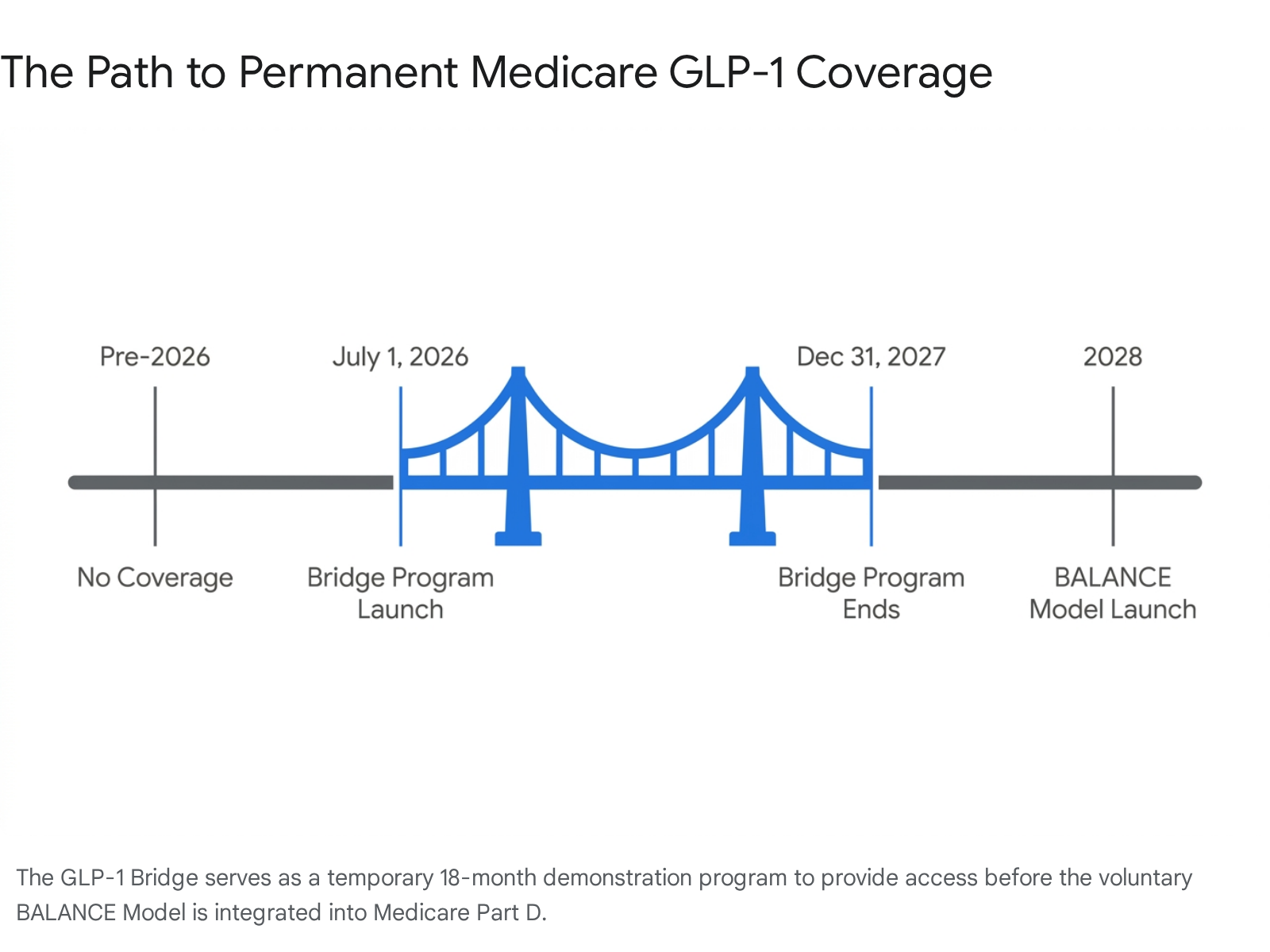
It is designed to provide immediate access and collect real-world utilization data while the government builds a much larger, permanent infrastructure known as the Better Approaches to Lifestyle and Nutrition for Comprehensive hEalth (BALANCE) Model 15611514616263417.
The BALANCE Model is a multi-year demonstration project that fundamentally shifts how Medicare handles weight-loss drugs 1517. Under BALANCE, CMS abandons the central processor approach and instead negotiates directly with drug manufacturers on behalf of participating Part D plan sponsors and state Medicaid agencies to permanently integrate affordable GLP-1 coverage into standard insurance benefits 52617.
Originally, BALANCE was scheduled to launch across both Medicare and Medicaid on January 1, 2027 162115146163417. The Medicaid portion is proceeding as planned, with states allowed to opt into the pricing model between May 2026 and January 2027 2526162617.
However, the Medicare Part D rollout encountered a massive roadblock. To launch BALANCE in Medicare, CMS required enough Part D insurance plans to voluntarily sign up to cover at least 80% of eligible beneficiaries 5. In April 2026, CMS announced that too few major insurers - including holdouts like UnitedHealth Group and CVS Health - were willing to participate and absorb the financial risk 5211. Consequently, CMS was forced to delay the Medicare implementation of BALANCE until at least 2028 5.
To prevent seniors from losing access in the interim, CMS officially extended the temporary GLP-1 Bridge through December 31, 2027 156211514162634173637.
This delay highlights a critical future risk for patients: when the BALANCE Model eventually launches in Medicare, participation will be voluntary for Part D insurers 1526. This means that beneficiaries utilizing the Bridge program in 2026 and 2027 will likely need to carefully evaluate and potentially switch their Part D plans during the 2027 open enrollment period, ensuring they select a plan that has formally opted into the BALANCE framework for 2028 111. Failing to switch to a participating plan could result in a sudden loss of coverage and a return to exorbitant out-of-pocket prices for life-saving obesity care 111.
Bottom line
Starting July 1, 2026, the Medicare GLP-1 Bridge will provide eligible Part D enrollees with unprecedented access to Wegovy, Zepbound (KwikPen), and the newly approved oral pill Foundayo for a predictable $50 monthly copay. Because the program operates entirely outside normal Medicare Part D benefits via a central processor, your $50 payments will not count toward your annual deductible or your $2,100 out-of-pocket maximum. While the Bridge secures affordable access through December 2027, the voluntary nature of the subsequent BALANCE Model means patients must remain vigilant during future open enrollment periods to ensure their coverage continues uninterrupted in 2028.