Efficacy and Dosage of Melatonin for Sleep
Exogenous melatonin (N-acetyl-5-methoxytryptamine) is one of the most widely consumed sleep therapeutics globally, utilized for conditions ranging from transient insomnia and circadian phase disruption to neurodegenerative sleep pathologies. Despite its ubiquity, clinical data reveals a profound disconnect between commonly available consumer dosages and the hormone's physiological mechanisms of action. While substantial evidence supports melatonin's efficacy as a chronobiotic agent for advancing sleep timing, its utility as a general hypnotic for sleep maintenance is limited. Pharmacokinetic data indicate that the supraphysiological doses standard in many commercial markets actively saturate target receptors, potentially triggering receptor desensitization and altering sleep architecture without conferring proportional therapeutic benefits 11.
Physiology of Endogenous Melatonin Synthesis and Secretion
Melatonin is an indoleamine hormone synthesized primarily in the pineal gland, though extra-pineal synthesis occurs in the gastrointestinal tract, retina, lymphocytes, and macrophages 2. The physiological production of melatonin is inextricably linked to the mammalian circadian system. The suprachiasmatic nucleus (SCN) of the hypothalamus acts as the central pacemaker, regulating pineal secretion in response to environmental light-dark cycles transmitted via intrinsically photosensitive retinal ganglion cells (ipRGCs) 34.
Circadian Variations in Systemic Concentration
In healthy adults, systemic melatonin levels exhibit a pronounced circadian rhythm. During daylight hours, plasma concentrations typically drop below 5 picograms per milliliter (pg/mL) 2. Secretion generally initiates between 21:00 and 22:00, leading to a phenomenon termed Dim Light Melatonin Onset (DLMO), which serves as a highly reliable phase marker for the circadian rhythm 24. Endogenous plasma concentrations reach their nocturnal peak - averaging between 50 and 100 pg/mL, though occasionally up to 134 pg/mL in males and 197 pg/mL in females - between 02:00 and 04:00 before sharply declining 256.
Systemic plasma levels do not fully reflect tissue or central nervous system concentrations. Due to direct release into the pineal recess of the third ventricle, melatonin concentrations in the cerebrospinal fluid (CSF) are substantially higher than in peripheral blood 27. Animal models, such as studies in sheep, have recorded nocturnal CSF melatonin concentrations as high as 19,934 pg/mL, establishing a significant concentration gradient as the fluid flows through the ventricular system 7. In humans, CSF measurements demonstrate acute sensitivity to sleep homeostasis; for example, young healthy volunteers exhibit elevated morning CSF melatonin levels following sleep deprivation (7.7 pg/mL) compared to baseline (3.2 pg/mL) 2.
Age-Related Secretion Decline
Endogenous melatonin synthesis exhibits a strong inverse correlation with chronological age. The most substantial decline occurs prior to puberty, but a secondary, significant reduction is observed between the ages of 20 and 30, and further in post-menopausal populations 29. This attenuation is largely attributed to the progressive calcification of the pineal gland, which results in the loss of functional pinealocytes, as well as age-related degenerative changes within the neurons of the SCN 2. The resulting "low-melatonin syndrome" is frequently implicated in the fragmented sleep architecture and reduced sleep efficiency common among elderly demographics 1011.
Receptor Subtypes and Intracellular Signaling
Melatonin exerts its physiological effects primarily by binding to high-affinity, seven-transmembrane G protein-coupled receptors (GPCRs). To date, two primary membrane-bound melatonin receptors have been identified in humans: MT1 (formerly Mel1a) and MT2 (formerly Mel1b) 89. An additional binding site, sometimes referred to as MT3 or Mel1C, exists in amphibians, birds, and some mammals like hamsters, but has not been conclusively identified as a distinct receptor in humans 39.
| Receptor Subtype | Chromosomal Locus | Primary Anatomical Expression | Primary Functional Roles |
|---|---|---|---|
| MT1 (Mel1a) | Chromosome 4 (4q35.1) | SCN, pars tuberalis, retina, pituitary, hippocampus 35. | Acute suppression of SCN neuronal firing (sleep onset), REM sleep promotion, vasoconstriction 5910. |
| MT2 (Mel1b) | Chromosome 11 (11q21-q22) | SCN, retina, osteoblasts, blood vessels 35. | Circadian phase shifting, NREM sleep promotion, dopamine inhibition in retina, vasodilation 5910. |
| MT3 (Mel1C) | N/A (Humans) | Kidneys, liver, adipose tissue (in non-human mammals) 9. | Intracellular detoxification, non-GPCR mediated pathways (nanomolar affinity) 9. |
Molecular Pharmacology of MT1 and MT2
Both MT1 and MT2 receptors couple to inhibitory Gi proteins. Activation of MT1 leads to the direct inhibition of adenylate cyclase, resulting in decreased intracellular cyclic AMP (cAMP) and reduced Protein Kinase A (PKA) activity 3. MT2 activation shares this cAMP inhibitory function but additionally suppresses cGMP production and couples to Gq proteins to modulate phospholipases C and A2, as well as potassium and calcium channels 389.
In vitro pharmacological assays demonstrate that melatonin binds to these receptors with exceptional affinity. Saturation binding studies utilizing [3H]-melatonin establish pKD values of 9.89 to 10.23 for the human MT1 receptor and 9.56 to 9.87 for the human MT2 receptor, indicating binding at picomolar to low nanomolar concentrations 1112. Both receptors exhibit the capacity to form homodimers and heterodimers, which may further diversify their pharmacological properties and downstream signaling cascades, though the exact physiological implications of this dimerization remain under investigation 89.
Pharmacokinetics of Exogenous Supplementation
The clinical application of melatonin requires an understanding of its pharmacokinetic profile, which deviates significantly from its endogenous secretion patterns. Exogenous melatonin acts systemically, freely crossing cellular and nuclear membranes due to its amphipathic (both lipophilic and hydrophilic) chemical structure 5.
Absorption, Bioavailability, and Clearance
Following oral administration, melatonin is rapidly absorbed, adhering to first-order kinetics. Time to maximal concentration (Tmax) generally occurs within 50 to 60 minutes for immediate-release (IR) formulations 1314. The oral bioavailability is notoriously variable, averaging approximately 15% to 33%, but ranging from 2.5% to 56% across individuals 131415. This massive interindividual variability is driven by an extensive first-pass hepatic metabolism, mediated almost exclusively by the cytochrome P450 enzyme CYP1A2 1415. Consequently, exogenous factors that influence CYP1A2 activity - such as caffeine consumption, cigarette smoking, and the use of medications like fluvoxamine or oral contraceptives - can dramatically alter melatonin clearance rates 13.
Elimination of melatonin is rapid. The elimination half-life (T1/2) for oral immediate-release formulations is generally between 20 and 60 minutes, while prolonged-release (PR) formulations extend the half-life to approximately 3.5 to 4.0 hours 15. More than 90% of circulating melatonin is cleared in a single passage through the liver, where it is hydroxylated into 6-hydroxymelatonin and subsequently excreted via the kidneys; only 2% to 5% of the hormone is excreted in the urine entirely unchanged 1415.
Dose-Dependent Systemic Exposure
The most critical variable in melatonin pharmacokinetics is the administered dose. In controlled studies evaluating older adults, researchers compared low-dose (0.4 mg) and high-dose (4.0 mg) surge-sustained melatonin preparations. The results indicated linear pharmacokinetic behavior: apparent total clearance (379 L/hr for 0.4 mg vs. 478 L/hr for 4.0 mg) and apparent volume of distribution were statistically similar 1.
However, because the high dose introduces a total molecular payload ten times larger than the low dose, the absolute systemic exposure (Area Under the Curve, or AUC) scales accordingly. In the 4.0 mg cohort, melatonin serum levels remained significantly elevated for an average of 10 hours - extending well beyond the standard 8-hour sleep period and persisting into the biological daytime 114. This pharmacological hangover directly contributes to adverse clinical outcomes, including next-day grogginess, somnolence, and transient impairments in postural balance and body temperature regulation 11416.
| Pharmacokinetic Parameter | Immediate Release (IR) | Prolonged Release (PR) / Controlled |
|---|---|---|
| Time to Peak Concentration (Tmax) | 20 - 60 minutes 1315 | 1.5 - 3.0 hours 114 |
| Elimination Half-Life (T1/2) | 20 - 60 minutes 15 | 3.5 - 4.0 hours 15 |
| Bioavailability | 9% - 33% (mean ~15%) 1315 | Varies significantly by excipient delivery matrix 1 |
| Hepatic Metabolism | CYP1A2 (hydroxylation) 1415 | CYP1A2 (hydroxylation) 1415 |
Receptor Saturation and the Supraphysiological Dose Dilemma
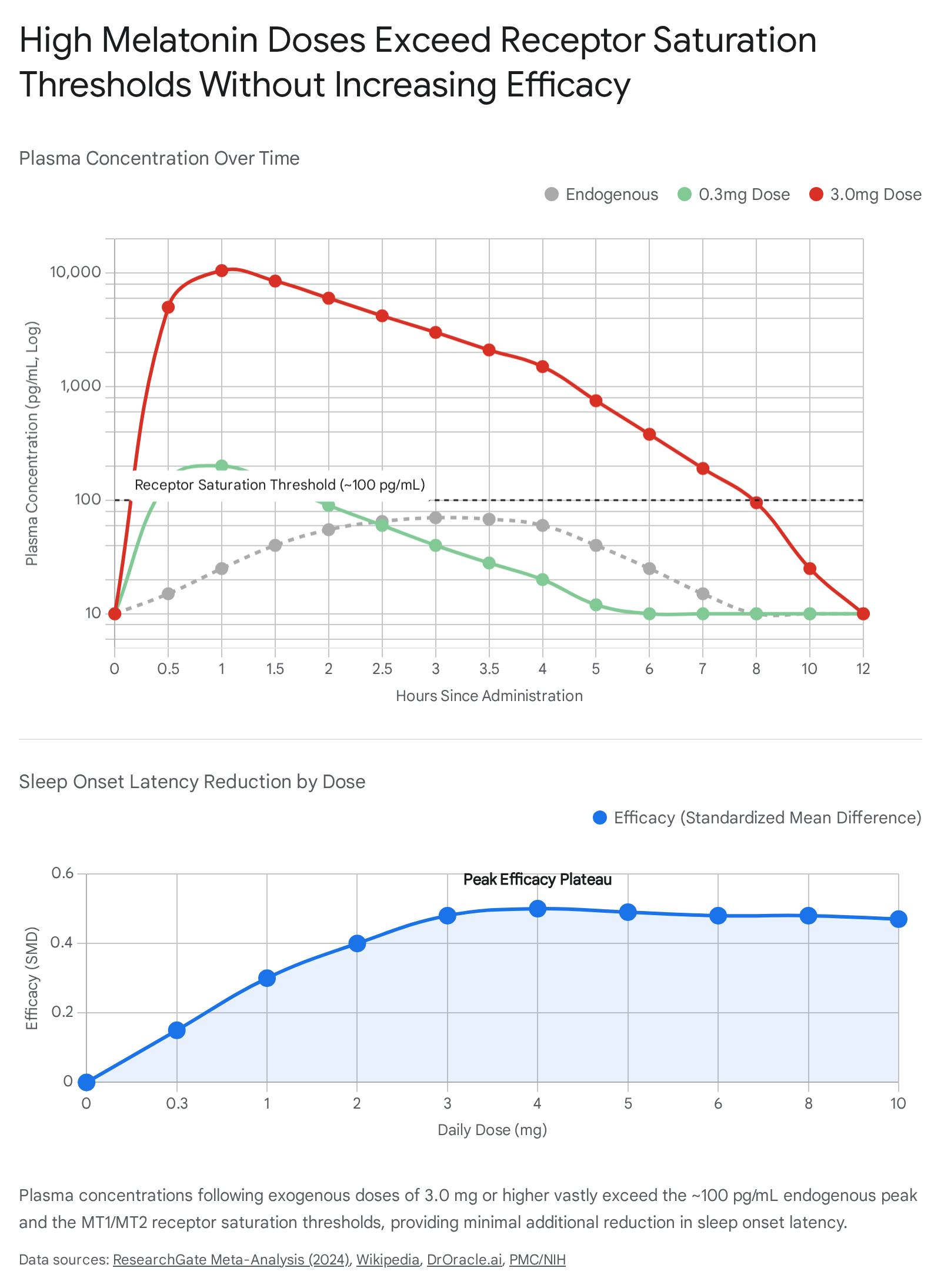
The prevailing trend in consumer supplement markets is the utilization of doses ranging from 3 mg to 10 mg, and occasionally higher. These doses are pharmacologically misaligned with the hormone's mechanism of action. A 0.3 mg oral dose reliably generates circulating melatonin concentrations that closely mirror endogenous peak nocturnal levels 815. Conversely, doses between 1 mg and 10 mg produce systemic concentrations 10 to 100 times higher than physiological baselines, frequently generating Cmax values exceeding 10,000 pg/mL 15.
The Uncoupling Phenomenon
The MT1 and MT2 receptors exhibit specific, finite binding affinities. Once systemic melatonin concentrations exceed physiological nocturnal levels (approximately 400 pM), these receptors achieve full saturation 1. In vitro research demonstrates that MT1 and MT2 receptors spontaneously exist in two states: G-protein coupled and uncoupled 12. Prolonged exposure to supraphysiological concentrations (e.g., 100 nM or higher) forces the receptors to desensitize. Rather than amplifying the therapeutic signal, excess melatonin decreases the binding affinity of the MT1 receptor and induces functional uncoupling from its associated G-proteins 18.
As a result, high-dose melatonin transitions the body's response from a receptor-mediated chronobiotic effect to a non-receptor-mediated profile. At these massive concentrations, melatonin begins to function strictly via its amphipathic properties as an intracellular free-radical scavenger and systemic antioxidant 15. While this antioxidant capability has profound implications for oncology and critical care, it provides zero additional benefit for sleep promotion.
Efficacy Limits in Primary Insomnia
The clinical translation of this receptor saturation is a stark plateau in efficacy. Meta-analyses encompassing thousands of patients reveal that while melatonin successfully decreases sleep onset latency (the time taken to fall asleep) by approximately 7 minutes and increases total sleep time by 8 to 11 minutes, titrating the dose upward does not yield proportional improvements 2117. Furthermore, melatonin demonstrates minimal efficacy in treating sleep maintenance insomnia (Wake After Sleep Onset, or WASO) 23.
Due to this limited hypnotic profile, organizations such as the American Academy of Sleep Medicine (AASM) advise against the routine use of melatonin for primary sleep onset or sleep maintenance insomnia in otherwise healthy adults, emphasizing that its primary utility remains strictly chronobiotic - shifting the circadian phase rather than acting as a traditional sedative 1.
Impact on Sleep Architecture and Dream Intensity
The neurobiological influence of melatonin extends beyond sleep initiation, deeply affecting the ultradian rhythm - the cyclical alternation between Rapid Eye Movement (REM) and non-REM (NREM) sleep 18. The relationship between exogenous melatonin and the frequently reported phenomenon of intensely vivid or bizarre dreams is rooted directly in the drug's interaction with REM architecture.
Comparative REM Modulation
To understand melatonin's effect on dreams, it must be contextualized against other classes of neuro-active medications. The majority of traditional sedative-hypnotics and psychiatric medications inherently suppress REM sleep: * GABA-A Agonists (Z-drugs and Benzodiazepines): Medications such as zolpidem and clonazepam aggressively inhibit REM sleep in favor of lighter NREM stages. Upon cessation, patients frequently experience a "REM rebound," leading to intense nightmares as the brain compensates for the period of suppression 2526. * Antidepressants (TCAs, SSRIs, SNRIs): Tricyclic antidepressants, Selective Serotonin Reuptake Inhibitors, and Serotonin-Norepinephrine Reuptake Inhibitors act on the midbrain raphe nuclei, increasing serotonin and noradrenaline outflow which directly inhibits REM-producing neurons. These agents prolong REM latency and drastically reduce total REM duration 419.
Melatonin behaves distinctly differently. Through the specific activation of the MT1 receptor within the SCN, melatonin actively preserves, and in certain dosages, enhances REM sleep duration 1020. Because REM is the neurological state most heavily associated with vivid, narrative-driven dreaming, any pharmacological agent that prolongs REM stages will proportionally increase dream volume and recall 262921.
The Vasotocin Hypothesis and Dream Bizarreness
The structural nature of "melatonin dreams" is hypothesized to be linked to the release of vasotocin. During melatonin-enhanced REM sleep, the pineal gland increases the secretion of vasotocin, a neuropeptide involved in the regulation of memory consolidation and the selective erasure of irrelevant memory traces during the dream state 2131. Elevated melatonin significantly boosts vasotocin activity, potentially leading to longer periods of memory-processing sleep that are subsequently recalled as highly intense, vivid, or bizarre narratives upon waking 31.
Empirical studies support these anecdotal claims. A placebo-controlled trial utilizing a 6 mg dose of melatonin in college students found statistically significant increases in validated measures of "dream bizarreness" - specifically regarding the structural transformation of objects and narrative events within the dream state 22. Notably, these effects demonstrated marked sex differences, indicating complex individual variability in neurochemical responses to the hormone 22.
For patients who find these vivid dreams disturbing, sleep medicine protocols dictate titrating the dose downward. Reducing exogenous melatonin to the physiological 0.3 mg to 1.0 mg range routinely alleviates intense dreaming by preventing the artificial hyper-extension of the REM cycle, further validating the dose-dependent nature of MT1 receptor modulation 29.
Clinical Applications of High-Dose Melatonin
While high-dose melatonin (3 mg to 10+ mg) is counterproductive for standard insomnia due to receptor saturation and next-day side effects, these exact supraphysiological concentrations represent highly targeted therapies for severe neurological and systemic pathologies.
Management of REM Sleep Behavior Disorder (RBD)
REM Sleep Behavior Disorder (RBD) is a severe parasomnia characterized by the pathological loss of normal muscle paralysis (atonia) during REM sleep. Patients physically enact their dreams, which frequently results in violent vocalizations, flailing, and trauma to themselves or bed partners 23. RBD is widely recognized as a prodromal marker for α-synucleinopathy neurodegenerative diseases, particularly Parkinson's disease and Lewy body dementia 2436.
Pathophysiologically, neurodegenerative progression in RBD patients includes a marked reduction in MT1 receptor expression in the striatum and MT2 receptor expression in the substantia nigra 20. High-dose exogenous melatonin has emerged as a cornerstone therapeutic for restoring physiological muscle atonia.
In clinical polysomnography studies, untreated RBD patients often exhibit abnormal muscle tone during up to 39% of their total REM sleep duration 2324. Following the nightly administration of 3 mg to 6 mg of melatonin, the proportion of REM sleep without atonia (RSWA) drops significantly, often to below 20%, correlating with a near-total cessation of violent nighttime behaviors 2337.
Crucially, high-dose melatonin provides a safer alternative to the traditional first-line RBD treatment, clonazepam. As a benzodiazepine, clonazepam carries profound risks for elderly populations with incipient neurodegeneration, including exacerbation of cognitive decline, respiratory suppression, and severe fall risks 2520. Comparative studies indicate that melatonin 6 mg yields similar reductions in clinical RBD severity scores while preserving natural sleep architecture and drastically reducing adverse events 37.
Pediatric Neurodevelopmental Insomnia
Pediatric populations presenting with severe neurodevelopmental disorders (NDDs) - such as Autism Spectrum Disorder (ASD), Attention Deficit Hyperactivity Disorder (ADHD), and neurogenetic anomalies like Smith-Magenis syndrome - frequently experience intractable insomnia resistant to standard behavioral interventions 141538. These populations often display inherent dysregulation of endogenous melatonin secretion, rendering them highly responsive to exogenous supplementation 1439.
In Europe and Australia, pharmaceutical-grade prolonged-release melatonin (marketed as Slenyto in 1 mg and 5 mg doses) has achieved formal regulatory approval specifically for pediatric insomnia associated with ASD and Smith-Magenis syndrome 1525. Long-term (52-week) randomized controlled trials demonstrate that daily administration of 2 mg to 10 mg of prolonged-release melatonin significantly reduces sleep latency and improves total sleep time without causing severe long-term adverse events, though minor issues such as daytime fatigue and mood swings occurred in roughly 3% to 5% of cohorts 14.
Oncology and Critical Care
Beyond the central nervous system, the non-receptor-mediated antioxidant properties of high-dose melatonin are being actively investigated in oncology and intensive care settings. Due to its ability to scavenge free radicals and mitigate oxidative stress, clinical trials have utilized massive systemic doses safely. For instance, chronic enteral doses of 300 mg per day over two years were well-tolerated in patients with Amyotrophic Lateral Sclerosis (ALS), normalizing markers of oxidative stress 42.
In oncology, doses ranging from 10 mg to 40 mg daily, administered in conjunction with interleukin-2 (IL-2) immunotherapy or standard chemotherapy, have demonstrated improved clinical outcomes and prolonged survival times in patients with metastatic non-small-cell lung cancer 42. Furthermore, acute intravenous administration of 20 mg of melatonin to neonates suffering from severe sepsis drastically improved clinical outcomes and prevented mortality by mitigating systemic ischemia-reperfusion injury 42.
| Clinical Indication | Typical Effective Dose | Mechanism / Rationale |
|---|---|---|
| Circadian Phase Shift (Jet Lag) | 0.3 mg - 1.0 mg 843 | MT2 receptor activation; avoids receptor saturation 1. |
| REM Sleep Behavior Disorder (RBD) | 3.0 mg - 12.0 mg 37 | Offsets receptor downregulation in substantia nigra; restores REM atonia 2037. |
| Pediatric NDD Insomnia (ASD/ADHD) | 1.0 mg - 5.0+ mg (Prolonged) 15 | Corrects inherent synthesis deficits; improves sleep consolidation 1439. |
| Oncology / Sepsis Adjunct | 10.0 mg - 300.0 mg 42 | Non-receptor-mediated intracellular free radical scavenging 142. |
Global Regulatory Frameworks and Quality Control
The stark division between the clinical reality of melatonin and consumer habits is largely a product of heterogeneous international regulatory frameworks. Governments approach the molecule either as a benign dietary supplement or as a potent, restricted neurohormone.
The United States: Dietary Supplement Classification
In the United States, the passage of the Dietary Supplement Health and Education Act (DSHEA) of 1994 legally grandfathered melatonin into the category of a dietary supplement 44. Consequently, the Food and Drug Administration (FDA) is prohibited from requiring rigorous pre-market safety, efficacy, or purity trials for melatonin products 45. It is widely available over-the-counter (OTC) in doses up to and exceeding 10 mg 46.
This lack of oversight has generated a systemic quality control crisis. Independent chemical analyses of commercially available melatonin supplements in the U.S., particularly within the highly popular "gummy" sector, reveal dangerous inaccuracies. A 2023 study published in JAMA documented that actual melatonin content ranged from 83% below the labeled amount to a staggering 478% above the declared concentration 1447. Furthermore, 26% of the tested products were contaminated with biologically active serotonin - a tightly controlled neurotransmitter that can precipitate severe cardiovascular and neurological events if ingested inadvertently 1444.
The European Union and Rest of World: Medical Precaution
In stark contrast, the European Union, the United Kingdom, Australia, and Japan classify melatonin utilizing the precautionary principle, viewing it as an active hormone requiring strict medical oversight 44.
Within the EU, prolonged-release melatonin formulations (such as Circadin) are universally categorized as prescription-only medicines, approved specifically for short-term use in adults over 55 1526. The availability of immediate-release melatonin as an OTC food supplement is highly fragmented and tightly controlled at the national level. France permits the highest OTC threshold in the bloc at a maximum of 2 mg per daily dose 4326. Italy and Poland cap OTC availability at a strict 1 mg limit 4349. In Germany and the Netherlands, OTC limits are set extremely low (below 1 mg, and often below 0.3 mg), effectively rendering standard therapeutic doses prescription-only 4349.
Globally, Australia's Therapeutic Goods Administration (TGA) regulates melatonin as a Schedule 4 prescription medicine, though it recently down-scheduled 2 mg prolonged-release formulations to Schedule 3 (Pharmacist Only) exclusively for patients aged 55 and older 45. Japan's Pharmaceuticals and Medical Devices Agency (PMDA) maintains perhaps the strictest stance, strictly prohibiting the manufacture or sale of hormone supplements and classifying melatonin solely as a tightly monitored prescription pharmaceutical 45.
Conclusion
The clinical profile of exogenous melatonin is defined by a paradox: the most commonly consumed doses are vastly unsuited for their most common intended use. For the general population seeking relief from transient insomnia or circadian misalignment, physiological micro-doses (0.3 mg to 1.0 mg) represent the optimal therapeutic window. These doses successfully trigger sleep-promoting MT1 and MT2 receptors without causing saturation, and they clear the hepatic system rapidly enough to prevent next-day cognitive impairment.
Conversely, the 3 mg to 10 mg dosages that saturate the North American OTC market fundamentally alter the drug's pharmacodynamics. At these levels, melatonin forces SCN receptors into uncoupled, desensitized states, flatlining any further reductions in sleep latency while drastically elongating the drug's systemic half-life. The consequence of this pharmacokinetic overload is the hyper-extension of REM sleep, vasotocin-induced vivid nightmares, and persistent daytime somnolence. High-dose administration is clinically justified only when explicitly targeting severe pathologies - such as restoring muscle atonia in REM Sleep Behavior Disorder, managing pediatric neurogenetic insomnia, or leveraging the molecule's non-receptor antioxidant properties in oncology and critical care. Ultimately, treating melatonin as a benign, dose-independent supplement ignores its potent identity as a structural neurohormone.