Caffeine pharmacokinetics, cognitive effects, and health evidence
Pharmacokinetics and Systemic Metabolism
Caffeine (1,3,7-trimethylxanthine) represents the most widely consumed psychoactive substance globally, functioning primarily as a non-selective antagonist of adenosine receptors in the central nervous system. Its widespread integration into cultural rituals, dietary habits, and athletic protocols necessitates a rigorous understanding of its pharmacological mechanisms, cognitive impacts, and long-term health implications. Caffeine operates by competitively binding to the A1 and A2A adenosine receptor subtypes, thereby preventing the normal inhibitory, sleep-inducing signaling of endogenous adenosine 12. This antagonism initiates secondary neurochemical cascades, including the release of catecholamines such as epinephrine and dopamine, which mediate the compound's characteristic alerting, ergogenic, and metabolic effects 34.
Following oral ingestion, caffeine is rapidly and almost entirely absorbed by the gastrointestinal tract. Pharmacokinetic profiling indicates that absorption is typically complete within 60 minutes, with 99% of the substance successfully entering the systemic circulation after approximately 45 minutes 4. Peak plasma concentrations are generally achieved between 15 and 120 minutes post-ingestion, depending on the delivery matrix (e.g., aqueous solution, botanical suspension, or capsule) and gastric emptying rates 4. However, the elimination half-life of caffeine is highly variable, spanning a broad range of 1.5 to 10 hours in healthy adults, driven fundamentally by individual genetic polymorphisms and specific environmental factors 4.
Genetic Determinants of Clearance
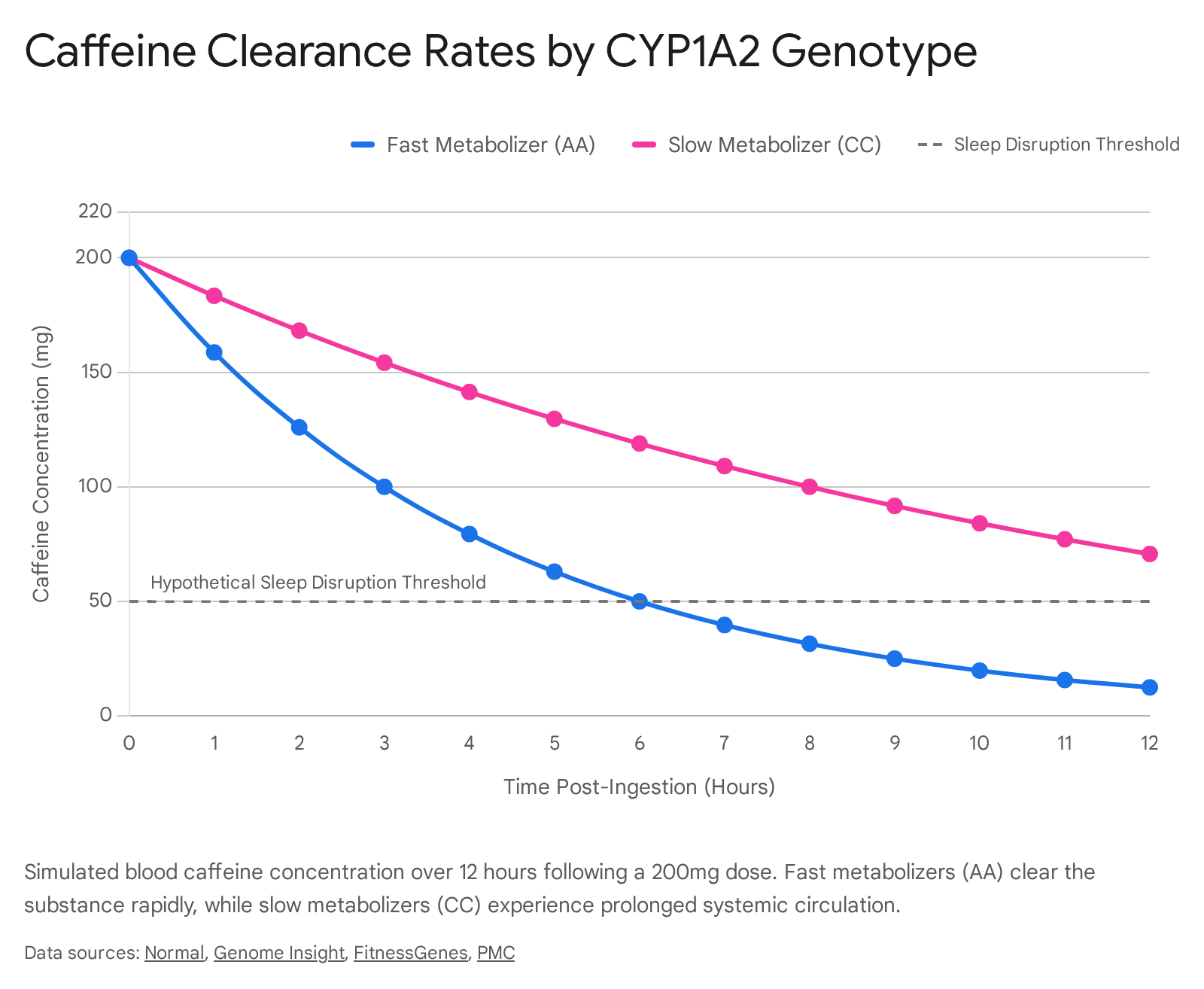
The metabolism of caffeine occurs predominantly in the liver, where over 95% of the compound undergoes demethylation into three primary active metabolites: paraxanthine, theobromine, and theophylline. This metabolic process is governed by the cytochrome P450 1A2 (CYP1A2) enzyme 675. The gene encoding this enzyme, CYP1A2 (located on chromosome 15q24.1), exhibits significant genetic polymorphism, which directly dictates the vast inter-individual variability observed in caffeine clearance and subsequent physiological responses 65.
The most clinically relevant single nucleotide polymorphism (SNP) in this gene is rs762551, characterized by a C-to-A transversion at position -163 in intron 1 675. This specific genetic variation alters enzyme inducibility and divides the population into distinct metabolic phenotypes.
| Genotype Profile | Metabolic Phenotype | Enzyme Activity Characteristics | Average Half-Life | Estimated Population Prevalence |
|---|---|---|---|---|
| AA (Homozygous) | Fast Metabolizer | High inducibility and rapid systemic clearance. | 2 - 4 hours | ~46 - 50% (European descent) |
| AC (Heterozygous) | Intermediate Metabolizer | Reduced enzyme activity and moderate clearance. | Variable | ~33 - 44% |
| CC (Homozygous) | Slow Metabolizer | Low enzyme activity; prolonged systemic circulation. | 6 - 10+ hours | ~10 - 15% |
In fast metabolizers carrying the homozygous AA genotype, caffeine is cleared rapidly, ensuring that its systemic physiological effects are transient and acute 910. Conversely, in slow metabolizers carrying the homozygous CC genotype, the CYP1A2 enzyme operates at a significantly reduced capacity. Consequently, caffeine and its active metabolites remain in the bloodstream for extended periods, continuously blocking adenosine receptors and maintaining elevated sympathetic nervous system activity for up to ten hours or more 910. This genetic dichotomy is critical for interpreting the highly individualized responses to caffeine, particularly regarding cardiovascular disease risk and the disruption of sleep architecture.
Beyond the CYP1A2 gene, the ADORA2A gene governs the sensitivity of the brain's adenosine receptors to blockade 10. Individuals exhibiting high receptor sensitivity combined with a slow metabolic clearance rate represent a phenotype that is particularly vulnerable to the anxiogenic and sleep-disrupting side effects of caffeine 10. Furthermore, environmental and physiological factors dynamically modulate CYP1A2 activity. Smoking heavily induces the enzyme, thereby accelerating metabolism and shortening the half-life 611. In contrast, the use of oral contraceptives and the physiological state of pregnancy significantly inhibit CYP1A2 activity, drastically prolonging the systemic circulation of caffeine and necessitating strict dosage reductions 410.
Therapeutic Doses and Cognitive Efficacy
Caffeine is widely utilized as a cognitive and ergogenic aid. Its efficacy, however, is heavily dose-dependent, and the relationship between intake and cognitive enhancement is not strictly linear. Clinical evaluations of caffeine on cognitive performance generally stratify doses into low (1 - 3 mg/kg of body weight), moderate (4 - 6 mg/kg), and high (>6 mg/kg) categories to measure differential outcomes 6137.
Dose-Response Relationships in Executive Function
Meta-analyses demonstrate that caffeine doses in the range of 100 to 600 mg effectively increase the speed of simple and choice reaction times 8. However, a recent comprehensive meta-analysis of 31 randomized, double-blind, placebo-controlled trials (encompassing 1,455 participants) revealed a nuanced dose-response dynamic regarding attention and precision. While reaction time exhibits a positive linear relationship with increasing caffeine doses (yielding a standardized mean difference, or Hedges' adjusted g, of 0.28), accuracy follows a distinct quadratic relationship 9. This indicates that accuracy improves up to a specific moderate dosage threshold, beyond which higher doses (≥ 200 mg) initiate a decline in precision, likely due to overstimulation, hyperarousal, and ensuing impulsivity 9.
In specific athletic populations, an acute dose of 6 mg/kg significantly improved both physical and motor reaction times (by approximately -0.04 seconds, P = 0.036 and P = 0.008 respectively) compared to a placebo, whereas a 3 mg/kg dose did not yield statistically significant improvements in these specific motor metrics 6. Conversely, for generalized attention and mood elevation in fatigued states, lower doses (around 3 mg/kg) are highly effective. Trials measuring post-exhaustive endurance exercise indicate that a 3 mg/kg dose yields an 11.5% improvement in attention, an 8.2% improvement in basic reaction time, and a 43% increase in positive mood states, suggesting that lower doses are optimal for preserving cognitive function under physical stress 17.
The Working Memory Paradox
While caffeine is universally acknowledged to enhance alertness and vigilance, its impact on higher-order executive functions, particularly working memory, remains highly contested. Recent double-blind, placebo-controlled clinical trials suggest that acute caffeine administration may actually impair specific domains of working memory, contradicting the popular perception of the substance as a universal cognitive enhancer 1011.
In spatial working memory assessments utilizing spatial span tasks, an acute dose of 200 mg of caffeine significantly impaired performance across delay-independent conditions (P = 0.013 for maximum scores obtained) 11. Furthermore, performance on verbal working memory tasks did not show any significant main effects following caffeine intake 11. Functional neuroimaging (fMRI) provides a physiological basis for these behavioral observations. In N-back working memory tasks, acute caffeine intake increases cerebral metabolic demands. However, over a period of daily, chronic intake (e.g., 150 mg administered three times daily over ten days), participants exhibited higher error rates and longer reaction times in complex (3-back) tasks compared to a placebo 10. Notably, blood-oxygen-level-dependent (BOLD) activity in the right hippocampus was significantly reduced in the caffeine condition compared to the placebo, indicating an adapted neurocognitive response to daily exposure that may negatively alter memory encoding and retrieval efficiency 10.
Ergogenic Effects in Physical Performance
In the domain of physical endurance and athletic performance, caffeine exerts a robust and well-documented ergogenic effect. A meta-analysis of 48 clinical trials involving 716 participants evaluated aerobic time-trial performance and determined that both low (≤3 mg/kg) and moderate (4 - 6 mg/kg) doses significantly reduced completion times compared to a placebo 13. The mean effect size for low doses was a standardized mean difference of -0.27 (a ~2.14% performance improvement), while moderate doses yielded an SMD of -0.52 (a ~2.18% improvement), establishing 4 - 6 mg/kg as the optimal range for consistent aerobic enhancement 13.
The mechanism for this enhancement is multifold. Peripheral adenosine receptor blockade reduces the subjective rating of perceived exertion and mitigates pain sensation, while central neurological effects maintain motor unit recruitment and delay central nervous system fatigue 1712. The genetic polymorphism of CYP1A2 also plays a subtle role in specific sports. For example, in elite basketball cohorts, the presence of the CA heterozygous genotype was statistically correlated with significant improvements in high-intensity intermittent exercise performance (such as the Yo-Yo IR2 test), suggesting that intermediate metabolizers may achieve an optimal balance of sustained systemic caffeine levels without excessive toxicity during prolonged matches 5. Doses exceeding 6 mg/kg, however, do not typically offer additional performance benefits and significantly increase the risk of adverse physiological side effects 137.
Adverse Effect Thresholds and Anxiety Syndromes
While moderate consumption is generally recognized as safe, high doses of caffeine precipitate a range of undesirable and potentially severe psychological effects. Clinical studies identify a specific threshold at 6 mg/kg where side effects such as nervousness (P = 0.001) and excessive activeness (P = 0.046) become statistically significant, detracting from any performance gains 6.
In absolute terms, daily doses exceeding 400 mg are associated with a marked increase in clinical anxiety and jitteriness 11322. A comprehensive meta-analysis of 14 studies involving 546 participants found a highly significant, dose-dependent anxiogenic effect. High-dose caffeine intake (≥400 mg) generated a massive standardized mean difference of 2.86 for anxiety risk, compared to an SMD of 0.61 for low-dose intake (<400 mg) 1. Mechanistically, caffeine's blockade of adenosine A1 and A2A receptors increases heart rate and triggers the release of adrenaline, mimicking the body's acute stress response 1. In susceptible individuals - particularly non-habitual consumers or those with pre-existing panic disorders - this physiological arousal is cognitively interpreted as impending danger, triggering acute anxiety episodes and panic attacks 12214.
Chronobiology and Sleep Architecture Disruption
The interference of caffeine with sleep architecture is one of its most consistently documented, yet frequently underestimated, side effects. Because caffeine competitively binds to adenosine receptors - the specific neurochemical sites responsible for accumulating "sleep pressure" throughout the waking day - its presence directly impedes both sleep initiation and maintenance 915.
A landmark 2023 systematic review and meta-analysis by Weakley et al., which aggregated data from 24 controlled crossover trials, provided highly specific pharmacokinetic guidelines regarding caffeine timing 1516. The aggregate polysomnographic data demonstrated that caffeine consumption prior to sleep results in profound and measurable architectural disruptions to the sleep cycle.
| Polysomnographic Metric | Average Impact of Pre-Sleep Caffeine | Clinical Implication |
|---|---|---|
| Total Sleep Time (TST) | Reduced by 45 minutes | Significant loss of recovery time; cumulatively results in 5.25 hours of lost sleep per week. |
| Sleep Efficiency | Decreased by 7% | More time spent in bed lying awake; fragmented and non-restorative rest. |
| Sleep Onset Latency (SOL) | Increased by 9 minutes | Prolonged transition from wakefulness to the first epoch of N1 sleep. |
| Wake After Sleep Onset (WASO) | Increased by 12 minutes | Disruption of sleep maintenance and continuity. |
| Stage 1 (N1) Light Sleep | Duration increased by 6.1 minutes | Shift toward superficial, easily disrupted sleep states. |
| Deep Sleep (N3 & N4) | Duration decreased by 11.4 minutes | Suppression of slow-wave sleep critical for physical recovery and memory consolidation. |
Data aggregated from the systematic review of 24 controlled crossover trials 1516.
Chronobiological Cutoffs: The 8.8-Hour Rule
Historically, public health advice suggested a generic "2:00 PM cutoff" for daily coffee consumption. However, the 2023 meta-analysis introduced precise, dose-dependent chronobiological guidelines based on advanced meta-regression models 162627.
To avoid statistically significant reductions in total sleep time, the clearance time must scale proportionately with the ingested dose. The researchers concluded that a standard cup of coffee (defined in the analysis as 107 mg of caffeine) must be consumed at least 8.8 hours prior to the target bedtime to mitigate sleep disruption 151627. A high-dose pre-workout supplement (defined as 217.5 mg of caffeine) requires a substantially longer clearance window of 13.2 hours prior to bedtime 151627. Conversely, very low doses (under 47 mg, roughly equivalent to a weak tea) are unlikely to negatively affect total sleep time regardless of their proximity to sleep initiation 1627.
Crucially, an individual's subjective perception of sleep quality does not reliably align with objective polysomnographic data. Clinical trials demonstrate that even when individuals consume caffeine six hours before bed and subjectively report sleeping well without perceived disruptions, objective at-home sleep monitors reveal a dramatic reduction in total sleep time (frequently exceeding one hour) and a suppression of deep sleep phases 281730. This disconnect suggests a widespread population-level accumulation of sleep debt driven by late-afternoon caffeine consumption.
Neurobiology of Reward, Tolerance, and Withdrawal
Caffeine's classification as an addictive substance has been historically debated within psychiatric circles, but modern neurobiology confirms that it induces physiological dependence, tolerance, and a robust, recognized withdrawal syndrome 1819.
Neurobiological Mechanisms of Addiction
Like classical drugs of abuse (e.g., cocaine, amphetamines, and opioids), caffeine acts upon the brain's mesolimbic reward pathway, though its mechanisms are fundamentally indirect and less potent 2420. The mesolimbic pathway is the critical neural circuit associated with motivation, incentive salience, and reward, projecting from the ventral tegmental area (VTA) of the midbrain to the nucleus accumbens (NAc) and the medial prefrontal cortex 42135.
Classical stimulants trigger a massive, direct surge of dopamine within the nucleus accumbens, flooding the synaptic cleft and creating an intense, intoxicating "high" 35. Caffeine, however, does not directly stimulate dopaminergic release in this violent manner. Instead, it exerts its primary action by blocking inhibitory adenosine A1 receptors located on both glutamatergic and dopaminergic terminals within the shell of the nucleus accumbens 2. By antagonizing these inhibitory receptors, caffeine effectively removes the chemical "brakes" on the system, facilitating a mild, secondary release of dopamine 2. This subtle neurochemical modulation promotes incentive salience (the psychological "wanting" or craving of the substance) and reinforces habitual consumption patterns, but it does so without triggering the intense, destructive compulsions and loss of control associated with illicit narcotics 42035.
Receptor Upregulation and Tolerance
With chronic, prolonged daily use (typically defined as regular consumption exceeding 400 mg/day), the central nervous system adapts to the constant blockade of adenosine receptors by upregulating the production of new adenosine receptors 1822. This physiological neuroadaptation means that an individual requires increasingly larger doses of caffeine to occupy the newly formed receptors and achieve the baseline alerting effects previously experienced at lower doses 2237. Because the dependent brain now possesses an excess of adenosine receptors, missing a regular dose of caffeine results in a massive, unimpeded influx of adenosine binding, triggering a rapid and severe withdrawal state 22.
The Clinical Withdrawal Syndrome
Caffeine withdrawal is a robust, clinically significant syndrome that occurs upon the abrupt cessation or substantial reduction of prolonged daily caffeine use. It can occur after the cessation of even relatively low daily doses (<100 mg) if the consumption has been chronic 1838.
The timeline of caffeine withdrawal is highly predictable. Symptoms typically emerge within 12 to 24 hours of the last dose, reach peak intensity between 20 and 51 hours, and gradually resolve over a period of 2 to 9 days 2238. The hallmark symptom is a severe, throbbing headache (reported in up to 50% of clinical cases), caused by the sudden rebound vasodilation of cerebral blood vessels that were previously chronically constricted by caffeine's action 2237. Other prominent symptoms include marked generalized fatigue, dysphoric or depressed mood, severe irritability, difficulty concentrating, and occasionally flu-like somatic symptoms such as nausea, vomiting, and muscle stiffness 223738. Approximately 13% of individuals experience symptoms severe enough to cause functional impairment in their occupational or social lives 1822. These symptoms are rapidly reversed - often within 30 to 60 minutes - upon the re-administration of caffeine, powerfully reinforcing the cycle of dependence 38.
Psychiatric Diagnostic Frameworks
The psychiatric community has formalized the diagnosis of caffeine-related disorders to address the clinical realities of dependence, though subtle taxonomic distinctions exist between the two major diagnostic manuals.
| Diagnostic Manual | Recognized Caffeine Syndromes | Key Criteria and Thresholds | Clinical Status |
|---|---|---|---|
| DSM-5-TR (APA) | Caffeine Intoxication, Caffeine Withdrawal | Diagnosis requires prolonged daily use followed by abrupt cessation causing ≥3 specific symptoms (headache, fatigue, dysphoria, etc.) resulting in clinically significant distress. | Officially recognized disorders. |
| DSM-5-TR (APA) | Caffeine Use Disorder (CUD) | Requires endorsement of 3 criteria: (1) persistent desire/unsuccessful effort to control use; (2) continued use despite physical/psychological harm; (3) clinical withdrawal. | Section III ("Condition for Further Study"); diagnosis purposefully conservative to prevent over-pathologizing. |
| ICD-11 (WHO) | Caffeine Dependence (Code 6C48) | Evident over a period of at least 12 months. Characterized by impaired control over use, increasing priority given to caffeine, and persistent use despite harm. | Officially recognized as a dependence syndrome. |
Data derived from psychiatric diagnostic criteria 382324414225.
Epidemiological surveys indicate that while daily consumption is nearly ubiquitous, only about 8% to 9% of the general adult population meets the strict, multi-criteria threshold for a proposed Caffeine Use Disorder diagnosis under the DSM-5 framework 2426.
Long-Term Health Evidence
While acute doses of caffeine modulate alertness and metabolic rates, the chronic, lifelong consumption of caffeinated beverages has profound impacts on population health, particularly concerning cardiovascular disease, metabolic syndrome, and neurodegeneration.
Cardiovascular Outcomes and the CYP1A2 Interaction
The epidemiological literature regarding caffeine and cardiovascular disease (CVD) appears contradictory until the data is stratified by genetic phenotype. Massive observational cohort studies consistently show that moderate coffee consumption is associated with a neutral or even slightly reduced overall risk of arrhythmias and heart disease 911.
However, when analyzing cohorts based on the CYP1A2 rs762551 polymorphism, a stark divergence in cardiovascular outcomes appears. For "fast metabolizers" (the AA genotype), consuming coffee - even at high volumes of up to 4 cups a day - does not increase the risk of myocardial infarction or hypertension. In fact, for this specific genetic group, habitual consumption may offer a protective vascular effect 611.
Conversely, in "slow metabolizers" (those carrying the CC or AC genotypes), chronic heavy caffeine intake acts as a severe, chronic cardiovascular stressor due to the prolonged half-life of the drug in the systemic circulation. Studies show that slow metabolizers who consume three or more cups of coffee daily face a staggering 64% higher risk of non-fatal myocardial infarction, an elevated risk of ischemic stroke, and significantly higher rates of essential hypertension compared to those drinking less than one cup 691011. Because approximately 50% of the global population carries at least one slow metabolizer allele, blanket dietary recommendations regarding the universal cardiovascular safety of high caffeine intake are fundamentally flawed and lack precision 10.
Type 2 Diabetes and Insulin Sensitivity
The relationship between caffeine and blood glucose regulation presents a complex physiological paradox involving conflicting short-term and long-term data.
In the acute, short-term setting, caffeine ingestion actively reduces insulin sensitivity. Hyperinsulinemic-euglycemic clamp studies - the gold standard clinical methodology for measuring in vivo insulin resistance - demonstrate that an intravenous dose of caffeine decreases whole-body insulin sensitivity by 15% compared to a placebo 327. This acute resistance is mediated by caffeine's potent stimulation of the sympathetic nervous system, leading to a fivefold increase in plasma epinephrine and a subsequent elevation in free fatty acids, which collectively impair the peripheral uptake of glucose by skeletal muscle tissue 3.
Despite this acute metabolic impairment, long-term epidemiological studies overwhelmingly show that habitual coffee consumption significantly reduces the risk of developing Type 2 Diabetes Mellitus 2728. A massive meta-analysis of 30 prospective studies found a 6% relative risk reduction for diabetes for every daily cup of coffee consumed 28. To bridge this gap, recent meta-analyses of long-term randomized controlled trials have investigated the chronic effects of coffee consumption (over periods exceeding seven days). These analyses conclude that chronic consumption results in a non-significant, neutral overall effect on established surrogate markers of insulin resistance, such as the HOMA-IR and Matsuda indices, indicating that the body adapts to the acute epinephrine surges over time 2829.
Furthermore, the specific chronobiological timing of consumption alters metabolic outcomes. A 2024 analysis of National Health and Nutrition Examination Survey (NHANES) data encompassing 21,138 participants revealed that consuming moderate amounts of coffee (1-2 cups) exclusively in the morning optimally improves insulin resistance. Conversely, heavier intake (≥3 cups) proves to be more metabolically beneficial when the consumption is distributed evenly throughout the day rather than consumed in a single bolus, provided the beverage is consumed black without added sugars or creamers 30.
Neuroprotection: Parkinson's and Alzheimer's Disease
Chronic caffeine consumption exhibits strong neuroprotective properties, primarily documented through massive observational cohorts and longitudinal studies 31. Cohorts tracking post-menopausal women and older adults consistently demonstrate that habitual caffeine intake is associated with a significantly delayed onset of general cognitive decline 31.
This neuroprotection is highly specific and evident in Parkinson's Disease (PD). Caffeine's targeted antagonism of A2A adenosine receptors in the basal ganglia functionally opposes the dopaminergic neuronal depletion that is characteristic of PD pathophysiology. This receptor blockade improves existing motor symptoms in patients and reduces the overall lifetime risk of developing the disease, particularly in men, though the protective benefits extend to women as well 713.
Regarding Alzheimer's Disease and vascular dementia, recent large-scale Asian cohort studies strongly correlate the consumption of green tea (the primary caffeine source in the region) with preserved brain integrity and structural health. A landmark 2025 study involving nearly 9,000 community-dwelling older adults in Japan demonstrated that regular green tea consumers possessed significantly fewer cerebral white matter lesions - structural brain changes intimately linked to cognitive decline, memory impairment, and vascular dementia risk 505132. This specific neuroprotective effect is largely attributed to the synergistic action of caffeine and tea polyphenols operating on cellular antioxidant pathways, a benefit that was not observed to the same degree in isolated coffee consumption within the same cohort 5132.
Pediatric Development and Anthropometric Outcomes
A persistent public health myth suggests that regular caffeine consumption stunts linear growth in children and adolescents. This misconception originated from early 20th-century advertising campaigns for grain-based coffee alternatives (such as Postum) and was perpetuated by initial, flawed observational studies suggesting that caffeine excessively impaired calcium absorption 5333.
Contemporary clinical evidence conclusively debunks the growth-stunting hypothesis. Rigorous longitudinal prospective studies tracking adolescents over six-year periods demonstrate zero statistical correlation between typical dietary caffeine intake and impaired total body bone mineral gain or final adult height, provided the youth consume adequate dietary calcium 533355. However, leading pediatric associations still strictly advise limiting intake to less than 2.5 mg/kg of body weight per day. The clinical rationale is not growth stunting, but rather the severe downstream effects of caffeine on pediatric sleep architecture, the developing cardiovascular system, and a significantly increased risk of triggering adolescent anxiety and mood disorders 535556.
Comparative Analysis of Caffeine Sources
The health outcomes associated with caffeine cannot be fully isolated from its delivery vehicle. The predominant global botanical sources - coffee, green tea (matcha), and yerba mate - contain vastly different phytochemical matrices that modulate the absorption, pharmacological action, and metabolic outcomes of the isolated caffeine molecule.
| Feature | Coffee (Coffea arabica/robusta) | Matcha / Green Tea (Camellia sinensis) | Yerba Mate (Ilex paraguariensis) |
|---|---|---|---|
| Caffeine per Cup | High (~95 - 200 mg) | Moderate (~30 - 70 mg) | Moderate to High (~30 - 80 mg) |
| Primary Bioactives | Chlorogenic acids, Diterpenes | L-theanine, EGCG (Catechins) | Theobromine, Theophylline, Saponins |
| Cognitive Profile | Rapid alertness, high peak energy. Higher risk of post-peak crash and jitters. | Sustained focus. L-theanine promotes alpha brainwaves, mitigating caffeine-induced anxiety. | Smooth, sustained energy release due to theobromine synergy. Low jitter risk. |
| Unique Health Evidence | Strongest inverse association with Parkinson's and liver disease. | Nrf2 pathway activation. Strongest evidence for stroke reduction and white matter lesion prevention. | Modulates lipid metabolism (lowers LDL). Unique evidence for increasing bone mineral density. |
Matcha and Green Tea
Matcha, a shade-grown, finely milled powdered green tea native to Japan, provides a unique pharmacokinetic experience compared to aqueous coffee extracts. Because the entire leaf is consumed rather than just an infusion, matcha offers a higher concentration of caffeine than standard steeped green tea, delivered alongside massive doses of the polyphenol Epigallocatechin gallate (EGCG) and the unique amino acid L-theanine 345859.
L-theanine actively crosses the blood-brain barrier and promotes the generation of alpha brain waves, inducing a state of calm relaxation that directly counteracts the jittery, anxiogenic side effects typically caused by pure caffeine 5860. Meta-analyses of randomized controlled trials confirm that the specific combination of L-theanine and caffeine produces superior effects on sustained attention, alertness, and complex task accuracy compared to caffeine alone, avoiding the abrupt energy crash associated with coffee 5058. Furthermore, the high concentrations of EGCG in matcha upregulate the Nrf2 cellular pathway, which stimulates the endogenous production of glutathione (the body's master antioxidant), protecting unsaturated fatty acids and neural tissue from age-related oxidative stress 51.
Yerba Mate
Yerba Mate, prepared from the dried leaves and twigs of the Ilex paraguariensis plant, is traditionally consumed in massive quantities (often exceeding one liter per day) in South American nations such as Argentina, Uruguay, and Brazil 35.
Beyond a moderate caffeine content, mate contains extraordinarily high levels of the related methylxanthines theobromine and theophylline. Theobromine acts as a potent vasodilator and smooth muscle relaxant, buffering the cardiovascular constriction typically caused by caffeine and resulting in a smoother, prolonged cognitive lift without acute spikes in blood pressure 626364.
Clinically, long-term cohort studies on yerba mate demonstrate highly unique metabolic benefits not seen with other caffeine sources. In 40-day clinical trials, the daily consumption of one liter of yerba mate significantly decreased LDL cholesterol fractions by 8.5% to 13% while simultaneously increasing cardioprotective HDL cholesterol in dyslipidemic patients 3536. Furthermore, unlike coffee, which has been historically scrutinized for causing slight urinary calcium excretion, longitudinal studies on postmenopausal women demonstrate that drinking one liter of yerba mate daily actually increases bone mineral density by nearly 10%, offering an unexpected but potent preventative dietary measure against the progression of osteoporosis 3566.