Effects of moderate alcohol consumption on the brain and body
For decades, the prevailing scientific consensus and public health guidance suggested that moderate alcohol consumption - historically defined as one to two standard drinks per day - conferred protective physiological benefits, particularly concerning cardiovascular health and longevity. This paradigm, heavily influenced by observational epidemiology and cultural narratives such as the "French Paradox," shaped global dietary guidelines and clinical advice. However, advancements in genetic epidemiology, high-resolution neuroimaging, and molecular biology have fundamentally dismantled this consensus.
By 2026, comprehensive reappraisals of legacy data, combined with advanced Mendelian randomization studies and large-scale biobank analyses, indicate that alcohol operates as a dose-dependent toxin across all exposure levels. The purported health benefits of moderate drinking have been largely attributed to systemic methodological flaws in older observational studies, notably the abstainer bias and the healthy user bias. Consequently, major global health organizations have radically shifted their policy frameworks, moving away from defining "safe" daily limits and instead emphasizing that physiological risk begins with the first drop of ethanol consumed.
Definitions and Epidemiological Measurement Standards
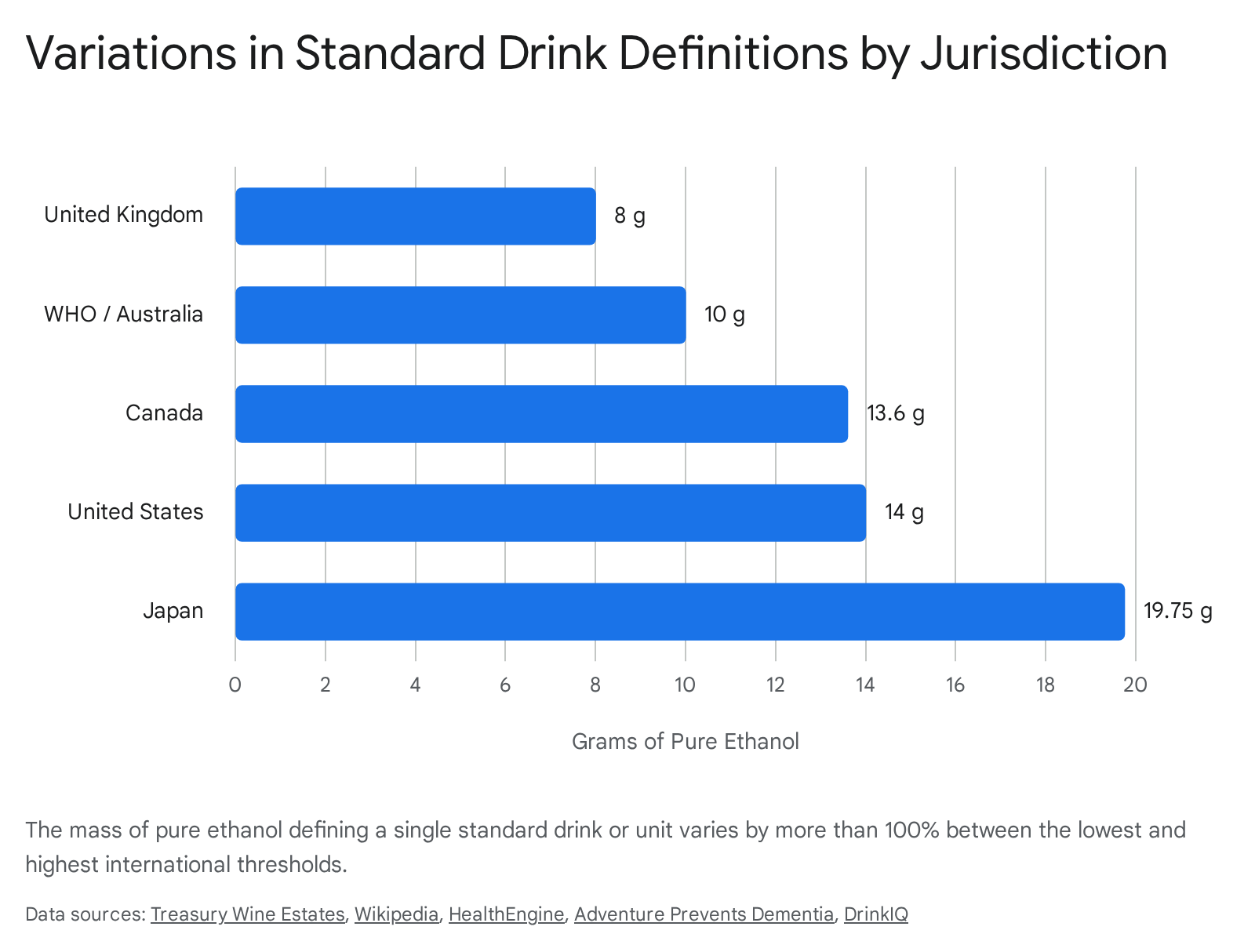
A primary structural challenge in global alcohol epidemiology is the absence of a universal definition for a "standard drink" or "unit" of alcohol. Different jurisdictions define a standard beverage based on varying masses of pure ethanol (measured in grams), which severely complicates the aggregation of self-reported consumption data and the translation of international research into localized public health advice 11.
The World Health Organization (WHO) utilizes a baseline of 10 grams of pure ethanol for its standard metrics and clinical screening tools, such as the Alcohol Use Disorders Identification Test (AUDIT). This 10-gram metric has been adopted by several nations, including Australia, New Zealand, France, and Germany 113. In contrast, the United Kingdom defines a unit as 8 grams, while the United States establishes a standard drink at 14 grams, and countries like Japan define a standard unit as nearly 20 grams 145.
| Jurisdiction or Organization | Mass of Pure Ethanol per Standard Drink | Equivalent Beverage Example (Approximate) |
|---|---|---|
| United Kingdom | 8.0 grams | 1/2 pint of lower-strength beer (3.6% ABV) |
| World Health Organization | 10.0 grams | Global baseline metric for clinical screening |
| Australia and New Zealand | 10.0 grams | 100 ml glass of table wine (12.5% ABV) |
| Canada | 13.6 grams | 5 oz glass of table wine (12% ABV) |
| United States | 14.0 grams | 12 oz can of regular beer (5% ABV) |
| Japan | 19.75 grams | 1 gō (180 ml) of traditional sake |
| Austria | 20.0 grams | 500 ml serving of strong beer |
Table 1: International variations in the definition of a standard drink by mass of pure ethanol 11345.
Because jurisdictional definitions differ so widely, the exact same physical beverage represents vastly different self-reported unit counts depending on the subject's geographic location. For example, a 150 ml glass of wine at 13% ABV represents one standard drink in the United States, 1.5 standard drinks in Australia, and nearly two units in the United Kingdom 15.
When aggregating historical observational data, failure to account for these differing national baselines frequently led to distorted dose-response estimates. Epidemiological studies must normalize alcohol exposure into absolute grams of ethanol per day or week to achieve cross-cohort validity 52. The lack of standardized cutoffs for exposure categories - such as defining what constitutes "light," "moderate," or "heavy" drinking - has historically been recognized as an overarching limitation in synthesizing global health data 2.
Public Health Policy Shifts and Dietary Guidelines
The aggregation of new toxicological and genetic evidence has forced a paradigm shift within global health policy. Regulatory bodies have transitioned away from harm-reduction models that endorsed moderate consumption, moving toward frameworks that clearly delineate the biological risks of any ethanol exposure.
Global Health Directives and the WHO Stance
In January 2023, the World Health Organization released a definitive consensus statement declaring that "no level of alcohol consumption is safe for our health" 78. The WHO reaffirmed that alcohol is a toxic, psychoactive, and dependence-producing substance, permanently classifying ethanol as a Group 1 carcinogen alongside asbestos, radiation, and tobacco 79. The agency emphasized that currently available scientific evidence cannot indicate the existence of a biological threshold at which the carcinogenic effects of alcohol "switch on"; rather, the risk to the drinker's health begins with the first drop of any alcoholic beverage 710.
To operationalize this understanding, the WHO spearheaded the SAFER initiative and implemented the Global Alcohol Action Plan (GAAP) 2022 - 2030. The GAAP aims to significantly reduce the harmful use of alcohol by restricting availability, enforcing pricing policies, and limiting marketing exposure 8312. Unlike previous strategies that invited the alcohol industry to contribute to harm reduction within their "core roles," the GAAP explicitly frames industry corporate social responsibility (CSR) activities as policy interference, establishing a more adversarial public health posture analogous to the historical regulation of the tobacco industry 313.
Revisions to National Dietary Guidelines
National health authorities have subsequently updated their domestic guidance to reflect the WHO's consensus. In 2023, Canada radically revised its national recommendations, stating that zero alcohol is the only risk-free approach. The Canadian guidelines established a stratified risk continuum: zero drinks per week is safest; 1 - 2 drinks represent the lowest risk of harm; 3 - 6 drinks indicate an increasing risk for certain cancers; and 7 or more standard drinks per week constitute a significantly elevated risk for cardiovascular disease and severe health outcomes 8144.
The United States followed suit, albeit with profound structural changes to its dietary advice. On January 7, 2026, the Department of Health and Human Services (HHS) and the Department of Agriculture (USDA) released the Dietary Guidelines for Americans (DGA) for 2025 - 2030 95. For 35 years prior, federal policy had explicitly permitted up to two drinks per day for men and one drink per day for women 94. The 2026 update eliminated these specific daily numeric thresholds entirely.
The revised U.S. guidelines now utilize the blanket advisory: "Consume less alcohol for better overall health" 51718. The guidelines also list categories of individuals who should completely avoid alcohol, including pregnant women, those recovering from alcohol use disorder, and individuals taking interacting medications 17.
Policy Debates and Clinical Backlash
The removal of the specific numeric limits from the U.S. Dietary Guidelines generated considerable debate within the medical community. The American Association for the Study of Liver Diseases (AASLD) issued a formal statement expressing deep concern over the omissions 5. While the AASLD agreed that consuming less alcohol supports overall health, the organization argued that removing quantitative daily limits denies the public evidence-based guardrails 518. Furthermore, critics noted that the new guidelines fail to account for the well-established biological differences in alcohol metabolism between men and women, and they omitted previous warnings directly linking alcohol consumption to breast cancer 519.
Some public health experts raised concerns that the vague directive to "consume less" was influenced by industry lobbying rather than strict epidemiological science 420. Clinicians pointed out that without a defined limit, individuals - who frequently misjudge the volume of a standard drink - might inadvertently consume larger quantities under the assumption that they are drinking "less" relative to heavier drinkers 418. Despite these criticisms, the policy shift marks the definitive end of governmental endorsement of moderate daily alcohol consumption in the United States.
Methodological Revisions in Alcohol Epidemiology
The historical consensus that moderate alcohol consumption improved longevity and reduced the risk of coronary heart disease was largely derived from the "J-shaped curve" frequently observed in longitudinal cohort studies. This curve suggested that light-to-moderate drinkers experienced lower mortality rates than both heavy drinkers and total abstainers 21623. However, modern epidemiological standards have demonstrated that this apparent protective effect was largely a statistical artifact generated by profound systematic biases.
Deconstructing Observational Biases
Observational studies linking moderate alcohol consumption to health benefits have historically suffered from severe confounding and selection bias. The most prominent methodological error is the "abstainer bias," commonly referred to as the "sick quitter" phenomenon 2325267.
In numerous historical cohorts, researchers compared moderate drinkers against a control group labeled "non-drinkers." However, this non-drinking control group inappropriately aggregated lifetime abstainers with former drinkers who had ceased consuming alcohol due to pre-existing illnesses, frailty, advanced age, or prior alcohol use disorder 223258. Because these "sick quitters" were already in poor health, the overall mortality and morbidity rates of the non-drinking group were artificially inflated 8. When compared against this baseline, moderate drinkers appeared deceptively healthy. When researchers disaggregate the data and properly classify sick quitters, the baseline mortality risk for true lifetime abstainers drops significantly, thereby flattening the J-curve 2526.
Furthermore, the "healthy user bias" systematically skewed observational outcomes. Epidemiological analyses reveal that individuals who maintain light-to-moderate drinking habits - particularly wine drinkers - tend to possess higher socioeconomic status, achieve higher levels of education, have better access to preventive healthcare, consume higher-quality diets, and engage in more regular physical activity than both heavy drinkers and strict abstainers 25299. Because these favorable lifestyle factors co-occur with moderate alcohol intake, traditional observational models mistakenly attributed the resulting cardiovascular benefits to the alcohol itself. Once modern statistical models rigorously adjust for these coincident healthy behaviors, the cardioprotective effects associated with modest alcohol intake consistently attenuate or disappear entirely 299.
The Role of Mendelian Randomization
To bypass the intractable confounding variables inherent in observational data, modern epidemiology increasingly relies on Mendelian randomization (MR). MR utilizes inherited genetic variants as instrumental variables to predict lifelong exposure to a risk factor, effectively serving as a natural randomized controlled trial that is immune to environmental confounding and reverse causation 10321112.
In alcohol research, MR studies primarily utilize variants in the alcohol dehydrogenase 1B gene (ADH1B, specifically the rs1229984 A-allele). Individuals carrying this genetic variant metabolize alcohol into toxic acetaldehyde far more rapidly than non-carriers 13. The rapid accumulation of acetaldehyde causes acute physiological discomfort, including facial flushing, nausea, and tachycardia 36. Consequently, carriers of this variant naturally self-limit their alcohol intake, consuming significantly fewer units of alcohol per week over their entire lifetimes 13. Because this genetic allele is randomly allocated at conception and is not linked to socioeconomic status, diet, or exercise, it provides an unconfounded proxy for low alcohol exposure 113738.
Systematic Reviews of All-Cause Mortality
When applying advanced methodologies to adjust for historical biases, the supposed mortality benefits of alcohol vanish. A definitive 2023 systematic review and meta-analysis published in JAMA Network Open evaluated 107 cohort studies encompassing over 4.8 million participants and 425,564 recorded deaths 394041.
The researchers employed mixed linear regression models to adjust for sampling variation, former drinker bias, median cohort age, and sex 4142. The meta-analysis found no statistically significant reduction in the risk of all-cause mortality for occasional drinkers (0 to 1.3 grams per day) or low-volume drinkers (1.3 to 24.0 grams per day) when compared to lifetime nondrinkers 3940.
Crucially, the data demonstrated a strict dose-response relationship for harm at higher intake levels, with biological sex serving as a significant vulnerability modifier. A statistically significant increase in all-cause mortality risk emerged for female drinkers consuming 25 or more grams of ethanol per day (approximately two standard drinks), whereas a similar statistically significant risk elevation in males was observed at 45 or more grams per day 394042. This meta-analysis confirmed that low-volume alcohol drinking is not associated with protection against death from all causes, underscoring that the safest level of consumption is strict abstinence 4041.
Neurological Atrophy and Cognitive Decline
The historical hypothesis that low-to-moderate alcohol consumption maintains cognitive health and preserves brain volume in aging populations has been rigorously contested by recent neuroimaging studies and genetic analyses. Ethanol and its metabolites act as potent neurotoxins, and their deleterious effects are detectable at exposure levels previously deemed benign.
Brain Volume and Structural Degradation
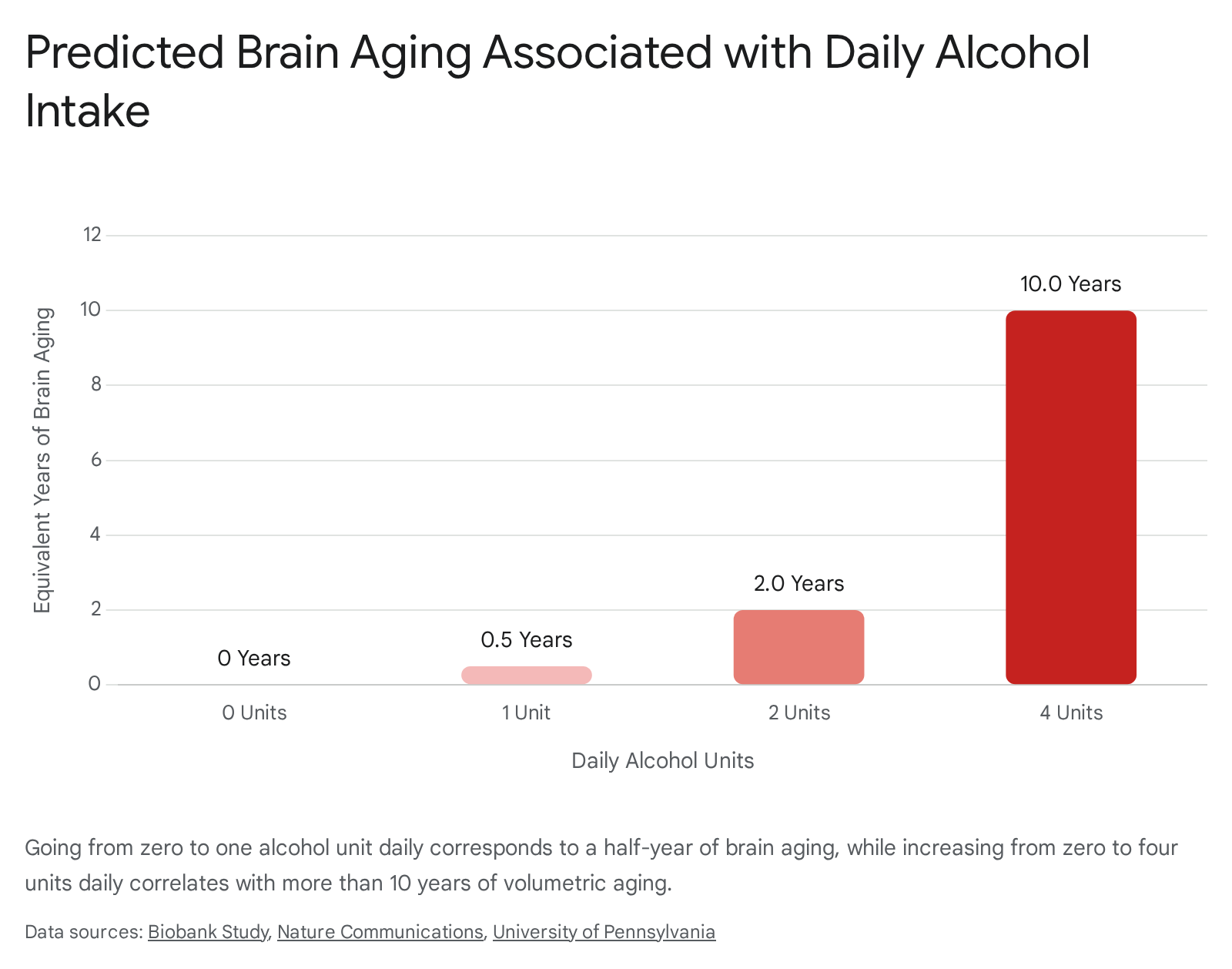
High-resolution magnetic resonance imaging (MRI) analyses have established a direct, non-linear relationship between daily alcohol consumption and macroscopic brain atrophy. A landmark 2022 study analyzing brain scans from 36,678 middle-aged participants in the UK Biobank revealed that even light-to-moderate alcohol consumption correlates with widespread reductions in overall brain volume, including significant decreases in regional gray matter density and compromised white matter microstructure 434414.
The structural degradation scales exponentially with increased intake. Researchers quantified the volumetric loss by mapping it against the natural neurological aging process. Transitioning from zero to one alcohol unit per day (approximately 8 grams of ethanol) was associated with the equivalent of a half-year of brain aging. Increasing from one to two units per day resulted in morphological changes equivalent to two full years of aging. Individuals consuming four units per day exhibited brain volumes consistent with over ten years of accelerated aging 434414.
These findings have been validated across diverse cohorts. A 2025 cross-sectional MRI study investigating 1,134 healthy adults without Alcohol Use Disorder (AUD) confirmed that moderate-to-high alcohol intake drives simultaneous structural changes across multiple organ systems. Compared to matched abstainers, the alcohol consumption group exhibited 10% larger liver volumes, 5.7% larger kidney volumes, and 15.6% higher visceral fat percentages 46. Crucially, cross-organ analyses revealed significant associations between this enlarged liver/kidney volume and accelerated brain atrophy in the left superior frontal cortex and right hippocampus, independent of confounding variables 46.
Neurometabolic Alterations in Healthy Drinkers
The neurotoxic effects of alcohol precipitate metabolic dysregulation well before macroscopic atrophy becomes visible. A 2025 study evaluating healthy, non-smoking adults (aged 22 - 70) with no history of AUD - who consumed an average of just 19 standard drinks per month - found measurable declines in vital brain metabolites 4715.
Using advanced spectroscopy, researchers observed lower levels of choline-containing compounds and myo-inositol in the anterior cingulate cortex (ACC) and the dorsolateral prefrontal cortex (DLPFC) in correlation with higher average monthly alcohol intake 15. Corresponding structural analyses of these participants revealed that higher monthly drink totals correlated with lower cerebral perfusion (blood flow) and reduced cortical thickness in these regions, which govern memory, decision-making, and executive function 4715.
Dementia Risk Reassessment
The persistent myth that light drinking prevents dementia has been comprehensively refuted by a 2025 study published in BMJ Evidence Based Medicine. This large-scale analysis combined genetic and observational data from over 559,559 individuals in the U.S. Million Veteran Program and the UK Biobank 4950.
While unadjusted observational data initially showed a U-shaped curve - where non-drinkers appeared to have a 41% higher risk of dementia than light drinkers - the genetic Mendelian randomization analysis revealed no such protective effect at low levels . The apparent protective effect in observational cohorts is a classic example of reverse causation: patients in the prodromal phases of cognitive decline, or those experiencing subclinical neurodegeneration, naturally reduce their alcohol intake in the years preceding a formal dementia diagnosis 495016.
When researchers measure alcohol consumption closer to the time of a dementia diagnosis, moderate drinking appears artificially protective because the individuals destined to develop dementia have already stopped drinking 16. However, when utilizing genetic variants (which reflect lifetime exposure risks unaffected by recent behavioral changes), the risk for all-cause dementia rises linearly in tandem with the quantity of alcohol consumed, beginning with the first unit 4950. The authors concluded that there is no safe level of alcohol for brain health and that reducing alcohol consumption is an essential strategy for dementia prevention 4916.
Biological Mechanisms of Ethanol Carcinogenicity
Alcohol is unequivocally classified as a Group 1 carcinogen. Current epidemiological and molecular data definitively link ethanol consumption to at least seven distinct types of cancer: bowel (colorectal), female breast, liver (hepatocellular carcinoma), oral cavity, pharynx, larynx, and esophagus 7175318. The physiological pathways driving this oncogenesis are complex, involving direct DNA damage, hormonal modulation, and oxidative stress.
Acetaldehyde Accumulation and DNA Damage
The primary mechanism of alcohol-induced carcinogenicity is driven by its highly toxic first metabolic byproduct: acetaldehyde. Upon ingestion, ethanol is oxidized primarily in the liver (and to a lesser extent in the oral cavity and gastrointestinal tract) by the enzyme alcohol dehydrogenase (ADH) into acetaldehyde 365556. Under normal physiological conditions, acetaldehyde is subsequently metabolized into harmless acetate by the enzyme aldehyde dehydrogenase (ALDH) 3657.
However, during active alcohol consumption, acetaldehyde transiently accumulates in tissues, inflicting direct genotoxic damage. Acetaldehyde is a highly reactive electrophile that interacts directly with DNA to form stable adducts, such as N2-ethylidene-2'-deoxyguanosine 5556. More critically, it forms interstrand cross-links (ICLs), which physically bind the two opposing strands of the DNA double helix together. These ICLs present a formidable barrier to the cellular machinery, actively obstructing DNA replication and RNA transcription 555758.
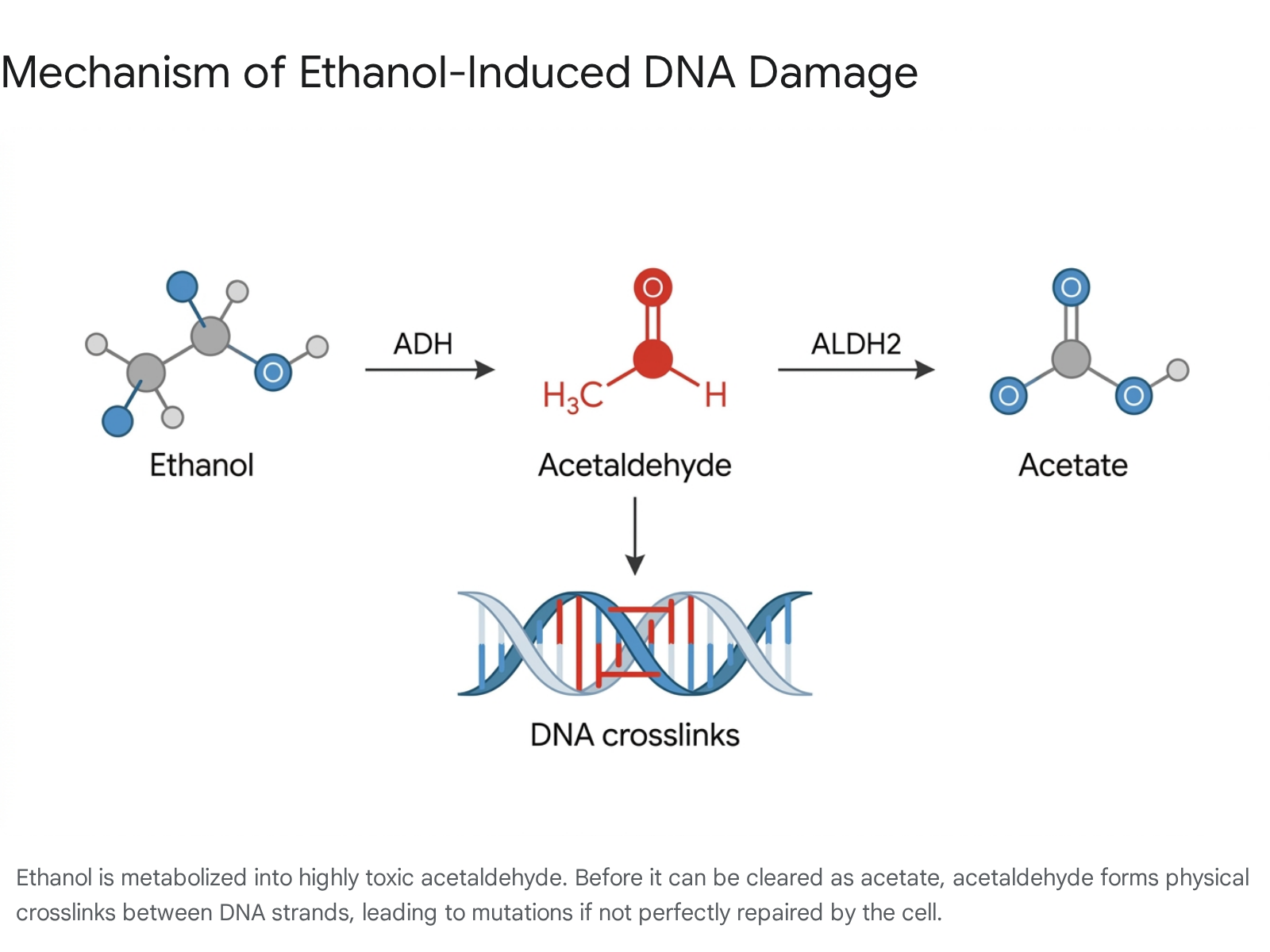
If cellular DNA repair mechanisms fail to adequately excise and reconstruct these cross-links, the resulting chromosomal instability leads to large genomic alterations, mutagenesis, uncontrolled cell proliferation, and ultimately oncogenesis 5758.
Cellular Repair Deficiencies and Genetic Vulnerability
The human body relies on highly specialized enzyme complexes to mitigate acetaldehyde-induced damage. The primary mechanism for excising interstrand cross-links relies on the Fanconi anemia (FA) repair pathway, specifically utilizing the SXE enzyme complex (SLX4-XPF-ERCC1) to surgically cut out the damaged DNA site and initiate repair 5758. If individuals carry genetic mutations affecting these specific DNA repair mechanisms, their cells cannot efficiently reverse the structural damage caused by low doses of alcohol.
This biological vulnerability is drastically exacerbated in individuals with genetic deficiencies in the ALDH2 enzyme. A mutation in the gene coding for ALDH2 limits the body's ability to convert toxic acetaldehyde into benign acetate. This deficiency is highly prevalent globally, affecting nearly half of the East Asian population (over 2 billion people) 365357. When individuals lacking a fully functional ALDH2 enzyme consume alcohol, acetaldehyde accumulates rapidly in the blood and local tissues, causing immediate symptoms like a flushed complexion and nausea 3653. More insidiously, laboratory studies demonstrate that mice lacking the ALDH2 enzyme suffer four times as much permanent DNA damage in their blood stem cells when exposed to ethanol compared to those with fully functioning enzymes 3657. For these populations, even minimal alcohol exposure carries an exponentially higher risk of mutagenesis.
Dose-Response Relationships in Specific Cancers
Epidemiological evidence confirms that the oncological risk of alcohol consumption follows a strict dose-response relationship, with elevated risks evident even at very low exposure levels.
For female breast cancer, ethanol not only causes direct DNA damage but also alters endocrine profiles. Alcohol elevates endogenous hormone levels, specifically estrogen, thereby creating a microenvironment highly conducive to tumor development 953. Dose-response meta-analyses indicate that consuming just 10 grams of ethanol per day (approximately one standard unit) elevates the relative risk of developing premenopausal breast cancer by 5%, and postmenopausal breast cancer by 9% 17. Consequently, global health models estimate that nearly 100,000 cases of breast cancer worldwide annually are directly attributable to light-to-moderate drinking 53.
The risk profile scales identically for other malignancies. Light alcohol consumption is significantly associated with higher risks of esophageal and colorectal cancers 59. As consumption moves from light to moderate (12.5 to 24.9 g/day), individuals face increasingly elevated risks for laryngeal cancer 59. At heavy consumption thresholds (above 45 - 50 grams per day), the risk profile expands to include stomach, pancreatic, and prostate cancers 1859. Furthermore, heavy alcohol consumption dramatically increases the risk of hepatocellular carcinoma (liver cancer) by inducing chronic inflammation and alcoholic liver disease, leading to cellular cirrhosis - the primary precursor to hepatic malignancies 1753.
Cardiovascular Disease Reevaluation
For decades, the strongest argument in favor of moderate alcohol consumption was its purported ability to reduce the risk of ischemic heart disease and mortality. This assumption has collapsed under the weight of large-scale genetic epidemiology and a reevaluation of the biochemical mechanisms involved.
Genetic Evidence against Cardioprotection
Mendelian randomization (MR) studies have systematically failed to confirm the cardioprotective benefits of alcohol previously seen in observational research. A 2025 multi-biobank MR analysis investigated the causal role of alcohol on eight specific cardiovascular diseases 1012.
The genetic data demonstrated a consistent, causal relationship between genetically predicted alcohol consumption and an increased risk of severe vascular diseases. In the inverse variance-weighted analyses, a 1-standard-deviation (1-SD) increase in genetically predicted log-transformed alcoholic drinks per week resulted in an odds ratio (OR) of 1.27 for stroke and a massive OR of 3.05 for peripheral artery disease 1012. Furthermore, the study found suggestive positive associations linking alcohol consumption to higher risks of coronary artery disease, atrial fibrillation, and abdominal aortic aneurysms 103212.
Crucially, the MR analyses found no evidence of any causal association - protective or harmful - between genetically predicted alcohol consumption and heart failure, venous thromboembolism, or aortic valve stenosis 12. Other large MR cohort studies utilizing the UK Biobank similarly confirmed that light alcohol intake is associated with modest, continuous increases in cardiovascular risk, while heavier consumption triggers exponential increases in the risk of both hypertension and coronary artery disease 299. There is no genetically supported evidence indicating that a low dose of ethanol protects the human cardiovascular system.
Debunking the French Paradox and Resveratrol
The most enduring cultural justification for moderate drinking originated from the "French Paradox" - a term coined in 1992 by researchers Serge Renaud and Michel de Lorgeril. They observed that French populations experienced unexpectedly low rates of coronary heart disease despite diets rich in saturated fats 1920. They hypothesized that the routine consumption of red wine, which constituted roughly 57% of all alcoholic beverage intake in France, mitigated the atherosclerotic process by decreasing platelet aggregation and improving endothelial function 20.
Subsequent molecular research zeroed in on polyphenols found in grape skins, particularly resveratrol, as the active cardioprotective agents. Laboratory models suggested that resveratrol exerts potent antioxidant, anti-inflammatory, and anti-proliferative effects 2062. For example, studies indicated that resveratrol inhibits the formation of inflammatory factors linked to heart disease by binding to and activating a regulatory protein known as KSRP, which subsequently destabilizes the messenger RNA of inflammatory mediators 63.
However, translating these isolated in vitro cellular mechanisms to clinical dietary advice represents a profound scientific fallacy. By 2026, the scientific community broadly rejects the notion that red wine consumption is a viable therapeutic mechanism, primarily due to insurmountable pharmacokinetic limitations regarding dosage and bioavailability 6221.
Pharmacokinetics and Bioavailability Discrepancies
While high-dose, purified resveratrol supplements have demonstrated varying degrees of efficacy in modifying blood pressure and inflammation markers in controlled clinical trials, the required therapeutic dosage far exceeds what is biologically obtainable through red wine 6566.
Clinical consensus indicates that the therapeutic range for trans-resveratrol supplementation begins at 150 mg per day and scales up to 1,000 mg per day to achieve measurable cardiovascular or insulin-sensitizing effects 2167. Red wine contains negligible, trace concentrations of resveratrol, typically ranging between 0.36 and 1.97 milligrams per liter 68.
| Source | Concentration / Clinical Dose | Volume Required to Reach a 150 mg Therapeutic Dose |
|---|---|---|
| Clinical Resveratrol Supplement | 150 mg - 500 mg per capsule | 1 oral capsule |
| Average Red Wine | ~1.5 mg per Liter | 100 Liters (approx. 133 standard bottles) |
| Raw Peanuts | 0.03 - 0.14 μg per gram | Over 1,000 kilograms |
Table 2: Comparison of resveratrol concentrations in clinical applications versus dietary sources 216768.
To achieve even the lowest therapeutic dose of 150 mg from dietary sources alone, an individual would need to consume highly toxic, lethal volumes of wine on a daily basis. Furthermore, the bioavailability of dietary resveratrol is exceedingly low; after ingestion, the compound undergoes rapid and extensive first-pass metabolism in the liver and intestines, meaning only a minute fraction of the ingested polyphenol ever reaches systemic circulation in its active form 6221.
Consequently, any hypothetical cardiovascular benefit derived from the trace amounts of resveratrol in a daily glass of wine is overwhelmingly neutralized by the cardiotoxic, neurotoxic, and carcinogenic properties of the accompanying ethanol 2562. The lower rates of heart disease historically observed in the French Paradox are now recognized to be the result of broader dietary patterns (the Mediterranean diet), socioeconomic factors, and methodological discrepancies in older epidemiological reporting, rather than the consumption of wine itself 1962.
Conclusion
The comprehensive evidence base compiled by 2026 indicates unequivocally that moderate alcohol consumption provides no net physiological or cognitive benefit to the human body. The historical perception of alcohol as a cardioprotective or neuroprotective agent was an epidemiological illusion, generated by complex socio-behavioral confounders, flawed control groups, and an incomplete understanding of genetic variables.
Physiologically, even modest daily intake (10 to 20 grams of ethanol) compromises global brain volume, reduces essential cortical thickness, and accelerates macroscopic neurological aging. Systemically, ethanol metabolism generates toxic acetaldehyde, which inflicts direct DNA interstrand cross-links and drives the dose-dependent oncogenesis of several major malignancies, including breast and colorectal cancers. Furthermore, advanced genetic methodologies confirm that alcohol linearly increases the risk of severe cardiovascular events, rendering the protective hypotheses of red wine and resveratrol biologically unfeasible. While human beings must contextualize and manage various lifestyle risks, the scientific reality is unambiguous: the physiological threshold for safe alcohol consumption does not exist.