Disruptive innovation and digital health platform value chains
Theoretical Foundations of Disruptive Innovation in Healthcare
Sustaining Innovation Versus Disruptive Innovation
The structural transformation of the modern healthcare sector can be critically analyzed through the lens of disruptive innovation, a theoretical framework originally articulated by Clayton Christensen. In its foundational premise, the theory distinguishes between sustaining innovations and disruptive innovations 1234. Sustaining innovations are advancements that market leaders introduce to improve the performance of existing products or services, typically targeting their most demanding and profitable customer segments 14. Within the healthcare ecosystem, sustaining innovations encompass incremental or leapfrog improvements that rely on established business models and clinical workflows. Examples include advanced robotic surgical procedures, highly specialized pharmaceutical biologics targeting complex syndromes, and sophisticated diagnostic imaging modalities 14. While these innovations yield superior clinical efficacy, they inherently drive up systemic costs, require profound technical expertise, and inadvertently limit healthcare accessibility to populations with comprehensive insurance or high socioeconomic status 12.
In contrast, disruptive innovation aims to simplify access and reduce costs rather than optimize performance for the high-end market. Disruptive technologies initially take root in simple applications at the bottom of a market or create entirely new markets by targeting "non-consumers" - individuals who previously lacked the financial resources or geographic proximity to access a service 234. Over time, these disruptive solutions relentlessly improve and move upmarket, eventually displacing established legacy competitors. In medical practice, disruptive innovations are characterized by their ability to decentralize care, shifting interventions away from high-cost, specialized acute care hospitals and toward lower-cost venues, such as retail clinics, community centers, or the patient's own home 235.
Typologies of Disruption
The academic literature further stratifies disruptive innovation into distinct typologies that dictate how new entrants penetrate the healthcare market.
Low-end disruptions occur when a new operating or financial approach leverages lower gross profit margins and higher asset utilization to capture the least profitable customers of incumbent organizations 4. Retail clinics, such as CVS MinuteClinic, exemplify low-end disruption by utilizing nurse practitioners rather than specialized physicians to treat a narrow scope of common, low-acuity conditions at a fraction of traditional costs 3. Conversely, new-market disruptions involve products that are significantly more affordable and simpler to use, enabling a completely new population to own and operate the technology 4. The transition from centralized mainframe computing to the personal desktop computer serves as the classic historical analog 25. In healthcare, the proliferation of over-the-counter continuous glucose monitors and mobile health (mHealth) applications represent new-market disruptions, transferring chronic disease monitoring capabilities from the clinic directly to the patient 35. Hybrid disruptions combine elements of both low-end and new-market approaches, creating expansive digital platforms that serve both unresourced populations and routine primary care patients 4.
| Innovation Category | Primary Objective | Target Demographic | Cost Trajectory | Examples in Healthcare |
|---|---|---|---|---|
| Sustaining Innovation | Enhance performance of existing solutions | High-acuity, demanding patients | Increases systemic costs | Advanced biologics, robotic surgery, specialized oncology treatments |
| Low-End Disruption | Provide "good enough" care at a lower price point | Least profitable or over-served patients | Decreases per-encounter costs | Retail clinics, asynchronous urgent care messaging |
| New-Market Disruption | Create access where none previously existed | Non-consumers lacking prior access | Expands overall market access affordably | Wearable biometric sensors, direct-to-consumer telehealth apps |
Core Prerequisites for Healthcare Disruption
For a healthcare intervention to successfully achieve disruptive scale, it must integrate three interdependent elements: an enabling technology, an innovative business model, and a coherent value network 35.
An enabling technology is the mechanism that democratizes capability, allowing lower-cost providers or patients themselves to perform tasks that historically required extensive expertise 25. Telehealth infrastructure and artificial intelligence (AI) symptom checkers serve as contemporary enabling technologies 3. However, technology alone is insufficient to disrupt entrenched systems; it must be coupled with an innovative business model designed to operate profitably at lower price points. Legacy healthcare institutions, structured with heavy administrative overhead to support complex procedures, often struggle to adopt these low-margin models natively 245. Consequently, disruption relies on a coherent value network - a supportive ecosystem in which suppliers, distributors, insurers, and patients are mutually incentivized to prioritize and sustain the disruptive technology over the status quo 35.
Restructuring the Patient Care Value Chain
Application of the Value Chain Framework to Healthcare Delivery
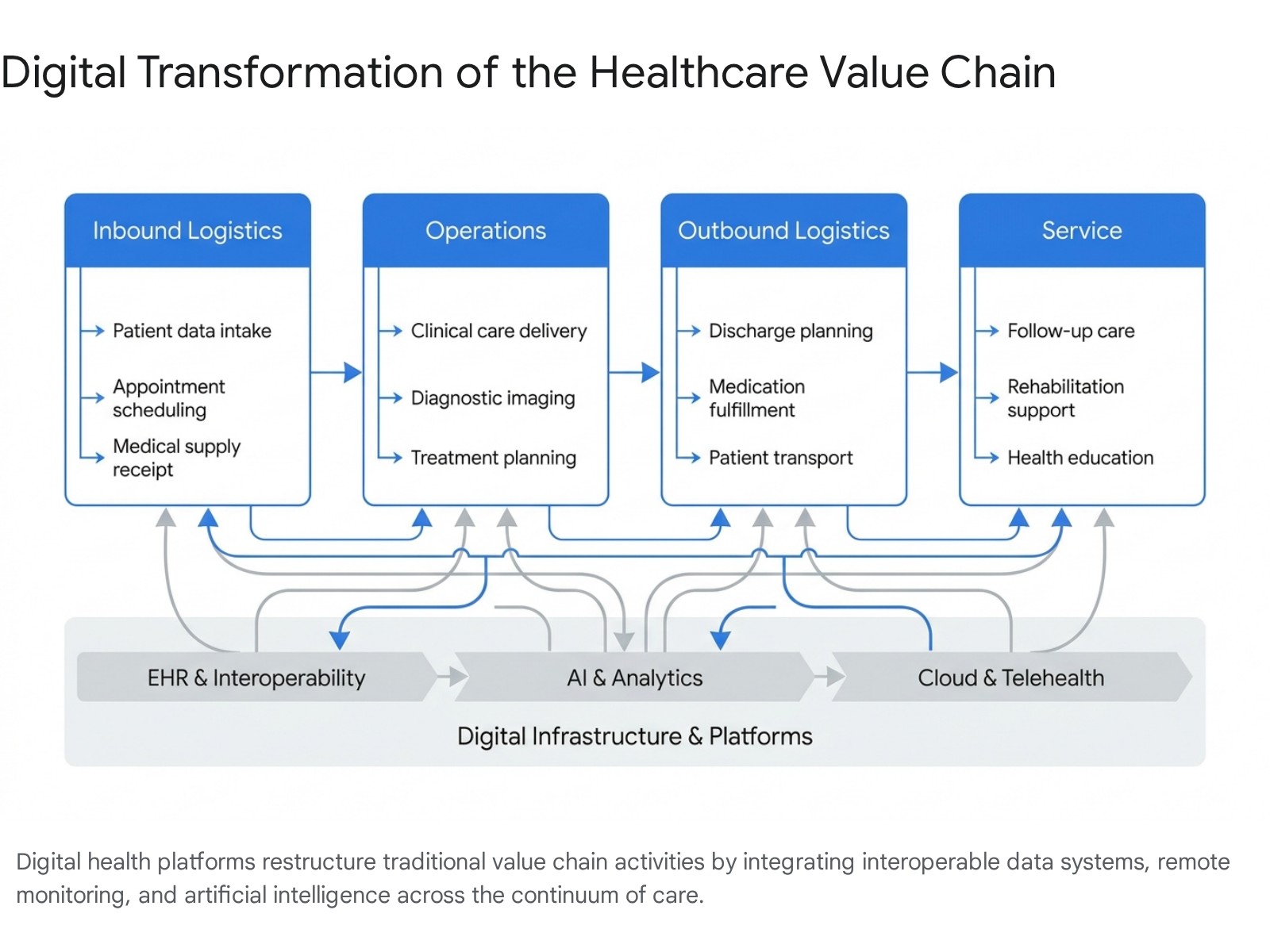
The operational restructuring driven by digital health can be analyzed using Michael Porter's value chain framework. Originally conceptualized to map how a firm adds value by transforming inputs into outputs, the value chain in healthcare has historically been a linear, highly centralized sequence of in-person events 678. It encompasses primary activities - inbound logistics (patient intake), operations (clinical diagnosis and treatment), and outbound logistics (discharge and follow-up) - supported by secondary functions such as procurement, human resources, and technological infrastructure 68.
Digital health platforms are actively dismantling this linear model. By integrating electronic health records (EHRs), the Internet of Medical Things (IoMT), cloud computing, and AI, these platforms establish a decentralized, continuous, and data-driven ecosystem 691010. This digital transformation enhances operational efficiency, enables strategic differentiation through personalized medicine, and supports cost leadership by minimizing physical resource utilization 68.
Inbound Logistics and Administrative Optimization
In the inbound logistics phase of healthcare - comprising patient triage, scheduling, and initial intake - digital health platforms are radically mitigating administrative bottlenecks and optimizing patient flow. Front-end digital solutions powered by AI and natural language processing (NLP) are increasingly utilized to triage patients before they interact with clinical personnel 11.
Data from highly scaled platforms indicates that AI-driven symptom checkers can safely navigate vast volumes of preliminary inquiries. For example, some primary care platforms report that 70% of individuals initiating a conversation with an AI triage assistant complete the entire medical encounter via chat, diverting non-acute cases away from overburdened emergency departments and physical waiting rooms 11. When these virtual care recommendations are evaluated by human healthcare providers, the AI-generated diagnosis aligns with the provider's assessment in approximately 84.2% of cases 11. By automating these inbound activities, healthcare facilities reduce administrative overhead, minimize early diagnostic errors, and allocate specialized human resources solely to complex, high-acuity cases 9121314.
Clinical Operations and Diagnostic Augmentation
Within the core operations phase - where clinical diagnosis, intervention, and treatment occur - the value chain is augmented by clinical decision support systems (CDSS) and predictive analytics 91516. The integration of artificial intelligence and machine learning allows clinicians to process vast corpuses of unstructured medical data, imaging, and genomic profiles to deliver highly personalized treatment regimens 15161718.
A significant advancement in operational restructuring is the emergence of digital twin technology. Digital twins create dynamic, virtual representations of physical systems or physiological states spanning their lifecycles 15. In healthcare operations, digital twins integrate data from diverse sources - such as EHRs, medical devices, and administrative workflows - facilitating the simulation of clinical interventions and the optimization of hospital processes without introducing operational risk to actual patients 15. Furthermore, the application of large language models (LLMs) to administrative operations is beginning to reduce documentation burdens, though researchers warn that reliance on AI-generated clinical notes requires vigilant human oversight to prevent automation bias and clinical hallucination 1920.
Outbound Logistics and Post-Acute Care Management
The disruption of the value chain is perhaps most pronounced in the outbound logistics and post-sale service phases, which correspond to hospital discharge, rehabilitation, and chronic disease management. Historically, patient surveillance ceased or became highly fragmented once the patient left the clinical setting 621. Remote patient monitoring (RPM) platforms, wearable biometric technologies, and continuous data streaming have fundamentally uncoupled surveillance from physical proximity 692223.
This technological shift has catalyzed the Hospital-at-Home (HaH) and virtual ward service models. Patients recovering from acute events or managing chronic conditions are monitored 24/7 via IoMT devices that transmit vital signs directly to cloud-based monitoring centers 62223. These platforms enable real-time detection of clinical deterioration, significantly reducing hospital readmission rates and optimizing medication adherence 91118. By transitioning care from episodic, fragmented events to a continuous, digitally mediated partnership, health systems improve patient safety while lowering the infrastructural costs associated with maintaining inpatient bed capacity 9212223.
The Unbundling of Care and Asynchronous Delivery Models
Transition from Synchronous to Asynchronous Care
A profound mechanism driving the restructuring of the healthcare value chain is the unbundling of care 242527. Traditional medical reimbursement and delivery have been heavily bundled around the synchronous, face-to-face outpatient visit 24. Digital health platforms dismantle this paradigm by fragmenting the comprehensive clinical encounter into distinct, technologically mediated micro-interactions, shifting substantial portions of care to asynchronous modalities 2426.
Asynchronous care - frequently categorized as store-and-forward telemedicine - enables patients and providers to communicate, exchange medical data, and execute treatment plans without the requirement of real-time co-presence 272829. This model relies on secure patient portals, integrated electronic messaging, and uploaded data from continuous monitoring devices 142427. By uncoupling the clinical encounter from the rigid constraints of synchronous scheduling, asynchronous platforms introduce massive operational scalability. Clinicians are empowered to manage a significantly higher volume of patient interactions per hour, processing routine follow-ups, adjusting medications, and monitoring chronic disease trajectories during dedicated workflow blocks 262830.
Clinical Efficacy and Patient Outcomes
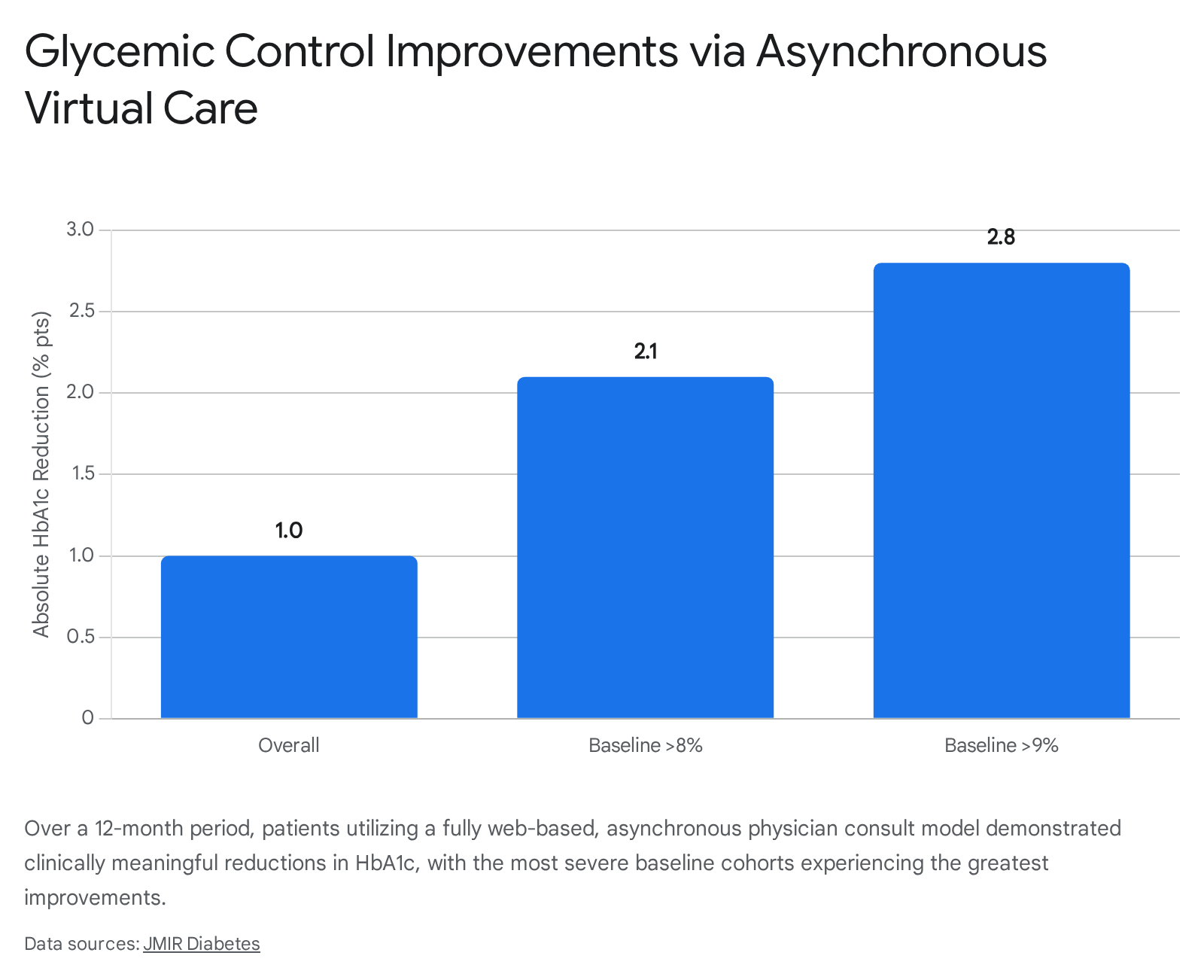
The expansion of asynchronous care is not merely an administrative convenience; empirical evidence demonstrates its clinical efficacy across diverse patient populations. Fully web-based, asynchronous physician review models, combined with asynchronous coaching and nutrition support, have yielded substantial improvements in chronic disease management 3132.
In longitudinal evaluations of diabetes management, patients participating in asynchronous remote monitoring and physician consultation models achieved an average hemoglobin A1c (HbA1c) reduction of 1.0 percentage point over 12 months 31. Notably, high-risk populations with a baseline HbA1c above 9.0% achieved an average reduction of 2.8 percentage points under this unbundled care model 31.
Similar results are observed in behavioral and lifestyle interventions; randomized non-inferiority trials suggest that asynchronous, text-based coaching yields weight loss outcomes equivalent to, or superior to, synchronous video conferencing, while drastically reducing the per-patient cost of delivery 32.
Operational Efficiency and Provider Cognitive Load
While asynchronous models alleviate geographical and scheduling barriers, their integration introduces novel challenges regarding provider cognitive load and workflow fragmentation 33. The continuous influx of secure patient messages outside of scheduled clinical encounters interleaves complex medical decision-making with routine administrative tasks, substantially increasing Task Switching Intensity (TSI) for providers 33.
To quantify the cognitive burden of asynchronous telehealth, health systems and researchers have developed metrics such as the Decision Complexity (DC) Index, a composite measure that evaluates the Information Engagement Depth (IED) and task switching required to appropriately respond to portal-based clinical inquiries 33. Recognizing this uncompensated labor, U.S. health systems and payers introduced billing codes between 2020 and 2023 designed to reimburse providers for complex, asynchronous medical decision-making (e-visits) 33. However, initial uptake of these message billing codes has remained extremely low, accounting for fewer than 1% of portal messages in some health systems 33. This discrepancy highlights the ongoing friction of retrofitting traditional fee-for-service reimbursement infrastructures onto highly unbundled, digitally native workflows 33.
Economic Implications and Value-Based Financing
Macroeconomic Pressures on Traditional Delivery
The imperative to restructure the healthcare value chain is largely driven by unsustainable macroeconomic pressures. In the United States, healthcare expenditures have escalated to approximately $4.1 trillion annually, consuming roughly 20% of the gross domestic product (GDP), with projections suggesting costs could surpass $6 trillion to $9 trillion by 2035 if systemic inefficiencies persist 2234. The structural economics of the traditional system are fundamentally misaligned: approximately 90% of healthcare costs are attributed to treating chronic and mental health conditions via acute, episodic interventions, while 25% of total spending is absorbed by administrative overhead 34.
Furthermore, traditional clinical models face severe inflationary forces. Hospital margins plummeted to an average of 2.1% by late 2024, battered by rapidly rising clinical wages, escalating supply chain costs, and surging pharmacy expenditures 35. In this highly constrained environment, digital health platforms are increasingly evaluated not strictly on their novelty, but on rigorous health economics and outcomes research (HEOR) to determine cost-effectiveness and systemic savings 363738.
Cost-Effectiveness of Digital Health Interventions
Cost-effectiveness analyses across various clinical domains consistently demonstrate that digital health interventions can yield significant systemic savings by shifting care to preventative, out-of-hospital settings.
In cardiovascular medicine, health economic modeling comparing digital monitoring strategies for atrial fibrillation against usual care reveals strong cost-effectiveness. Wearable-based monitoring strategies yield an Incremental Cost-Effectiveness Ratio (ICER) ranging from EUR 2,321 to EUR 3,647 per Quality-Adjusted Life Year (QALY) . Implantable digital monitors provide additional diagnostic yield at an acceptable incremental cost of EUR 5,520 to EUR 9,391 per QALY, remaining securely below standard willingness-to-pay (WTP) thresholds utilized by European health systems . Similarly, simulation models evaluating digital applications for lipid-lowering therapy adherence indicate that achieving optimal adherence through mobile health platforms can prevent between 34 to 63 cardiovascular events per 1,000 patients over a lifetime, generating absolute cost savings for healthcare systems in middle-income countries 38.
In long-term residential and skilled nursing settings, the deployment of sensor-based digital health technologies (DHT) for incontinence management demonstrated overall cost-savings of $1,467 per resident over a 2.34-year horizon. These savings were primarily driven by optimized labor allocation, reduced waste of physical absorbent products, and the prevention of skin-related clinical consequences 36. In the physical rehabilitation sector, systematic reviews of telerehabilitation interventions indicate a 90% probability of cost-effectiveness at a $30,000 per QALY threshold, achieving parity in clinical outcomes with traditional therapy while eliminating patient travel costs and mitigating hospital readmission risk 37.
| Clinical Domain | Digital Intervention | Primary Economic Outcome | ICER / Cost Savings Measure |
|---|---|---|---|
| Cardiovascular | Wearable AFib Monitoring | Highly cost-effective | EUR 2,321 - 3,647 / QALY |
| Cardiovascular | Implantable Loop Recorders | Acceptable incremental cost | EUR 5,520 - 9,391 / QALY |
| Residential Care | Incontinence Sensor Tech | Absolute cost savings | $1,467 saved per resident |
| Rehabilitation | Telerehabilitation Platforms | Highly cost-effective | 90% probability at $30k/QALY |
The Transition to Value-Based Healthcare
Despite the promising ICER metrics of isolated platforms, the realization of systemic financial benefits is frequently hindered by software fragmentation. The procurement of disparate, unintegrated software-as-a-service (SaaS) platforms can generate "cumulative costs" related to IT infrastructure, cybersecurity, and manual data reconciliation that outpace direct operational savings 19213940.
To extract maximum financial utility from digital restructuring, global health systems are pivoting from volume-driven fee-for-service models toward Value-Based Healthcare (VBHC) and Outcomes-Based Financing (OBF) 2741424344. Under VBHC frameworks, provider reimbursement is explicitly linked to the achievement of superior patient outcomes and the reduction of total cost of care over a longitudinal episode 4244. By aligning financial incentives with holistic patient health, VBHC provides the necessary economic justification for hospitals to invest in predictive analytics, continuous remote monitoring, and preventative digital outreach, as providers capture shared savings by preventing acute hospitalizations rather than billing for high-volume procedures 424344.
Global Implementation and Healthcare Leapfrogging
The Concept of Leapfrogging in Emerging Economies
The disruptive potential of digital health platforms is uniquely profound in Low- and Middle-Income Countries (LMICs). Faced with systemic deficits in physical medical infrastructure, severe shortages of trained clinical personnel, and vast geographic barriers to access, emerging economies are leveraging digital technologies to entirely bypass the traditional, hospital-centric developmental stages experienced by high-income nations. This phenomenon is termed "leapfrogging" 4546474849.
Analogous to how the African continent bypassed the slow, capital-intensive construction of landline telephone networks by rapidly adopting mobile cellular telecommunications, digital health leapfrogging utilizes high smartphone penetration and expanding broadband networks to instantly scale clinical access 454748. By skipping the initial requirement to build massive physical hospitals in rural areas, health ministries and private innovators deploy decentralized, cloud-based ecosystems that deliver care directly to the population 454850.
Infrastructure Bypass and Mobile Health Integration
The COVID-19 pandemic served as a massive accelerant for digital leapfrogging across Sub-Saharan Africa and Asia, forcing health systems to innovate rapidly to maintain care for highly prevalent non-communicable diseases (NCDs) amidst lockdowns 47515253.
Specific regional implementations illustrate the breadth of this value chain restructuring: * Telemedicine Hubs and Triage: Platforms such as 'Babyl' in Rwanda, 'Hello Doctor' in South Africa, and 'Tremendoc' in Nigeria have established expansive remote consultation networks. These platforms connect rural and underserved populations directly with licensed physicians via mobile networks, mitigating the impact of severe physician shortages 4753. Rwanda successfully integrated dedicated telemedicine centers into its national infrastructure, utilizing AI-assisted triage to manage population-level health efficiently 4749. * Mobile Financial Integration: A critical enabler of leapfrogging in LMICs is the seamless integration of digital health with mobile financial services. In Kenya, platforms like Access Afya partner with the ubiquitous M-Pesa mobile money network to offer transparent, micro-payment structures for remote care and bundled micro-insurance 125254. This circumvents the lack of traditional banking and complex insurance infrastructures, making primary care financially accessible to remote populations 1254. * AI and Supply Chain Optimization: Machine learning algorithms are being aggressively deployed for macro-level public health management. AI models analyze diverse datasets - including climate patterns, social media, and electronic health records - to predict disease outbreaks, a strategy proven effective during recent Ebola and COVID-19 responses 4953. Furthermore, supply chain disruptions are mitigated through digital ledgers and drone technology. Nations like Rwanda utilize nationwide digital networks to optimize inventory management, dispatch drone-assisted deliveries of vaccines and blood products to remote clinics, and secure the supply chain against counterfeit pharmaceuticals 10124749. * Chronic Disease Self-Management: With the World Health Organization estimating that 85% of premature deaths from NCDs occur in LMICs, shifting toward preventative care is an economic imperative 52. Platforms such as India's HealthifyMe - reaching over 30 million subscribers - leverage digital apps and wearables to provide highly tailored dietary and fitness coaching, aiming to preemptively manage lifestyle-related diseases across massive populations 5253.
Ecosystem Approaches and Public-Private Partnerships
To ensure the sustainability of these leapfrogging initiatives, there is a strategic shift away from traditional, fragmented philanthropic aid toward a sustainable "ecosystem approach" to public-private partnerships (PPPs) 46. This model relies on robust collaborations between national governments, global technology conglomerates, and local digital health start-ups 4654. For instance, federated data architectures spearheaded by organizations like IBM and the Mayo Clinic Platform enable LMICs to keep sensitive patient health data localized and secure, while simultaneously benefiting from the advanced algorithmic insights generated by global cloud-based AI networks 54.
Systemic Challenges and Implementation Barriers
Information Fragmentation and Interoperability Roadblocks
Despite the proven clinical and economic efficacy of digital disruption, the global healthcare sector confronts formidable friction in scaling these technologies. The paramount technological barrier is the profound fragmentation of the digital health ecosystem 214355565763. The rapid, often ad-hoc procurement of digital point solutions - accelerated by pandemic-era necessity - has inadvertently generated impenetrable data silos across the care continuum 125556.
When wearable biometric sensors, asynchronous patient portals, AI diagnostic algorithms, and foundational electronic health records cannot natively exchange structured clinical data, the patient care pathway remains fundamentally broken 9215558. This lack of interoperability forces highly trained clinicians to perform redundant manual data entry, compromises the integrity of longitudinal patient records, and neutralizes the predictive capabilities of big data analytics 435558.
The interoperability divide is particularly stark in Long-Term and Post-Acute Care (LTPAC) and rural settings. While heavily resourced academic medical centers may implement sophisticated, API-driven data exchanges, smaller facilities frequently lack the technical infrastructure, financial capital, and broadband connectivity required to participate 5759. Policy efforts to mandate data exchange encounter significant resistance and operational hurdles; a 2024 analysis projected that up to 32% of existing Health Information Organizations (HIOs) may decline participation in the federal Trusted Exchange Framework and Common Agreement (TEFCA), threatening to leave large segments of the healthcare system technologically isolated 57. Resolving this fragmentation necessitates the universal adoption of open standards, such as Fast Healthcare Interoperability Resources (FHIR), and the transition toward federated data spaces that prioritize secure, cross-platform communication 234363.
The Digital Divide and Health Inequities
While disruptive digital innovations aim to democratize care, they simultaneously harbor the risk of exacerbating existing health disparities through the expansion of the "digital divide" 4360616263. Often mischaracterized merely as a lack of internet access, the digital divide is a multidimensional socio-ecological inequity determined by five intersecting pillars: Access, Availability, Adequacy, Acceptability, and Affordability 3964.
| Dimension of Digital Divide | Manifestation in Healthcare Ecosystem | Resulting Impact on Patient Access |
|---|---|---|
| Access & Availability | Absence of broadband infrastructure in rural or tribal regions. | Precludes participation in video telehealth or real-time remote monitoring. |
| Affordability | High cumulative costs of hardware, data plans, and app subscriptions. | Excludes low-income populations from asynchronous care portals. |
| Adequacy | Substandard connection speeds or reliance on obsolete legacy devices. | Results in dropped clinical calls and failed transmission of vital biometric data. |
| Acceptability (Literacy) | Low digital health literacy, technophobia, and language barriers. | Causes non-adherence to digital treatment protocols, particularly in the elderly. |
Academic literature further conceptualizes this phenomenon across three strata. The primary digital health divide refers to fundamental inequalities in physical access to hardware and broadband 6371. The secondary divide highlights disparities in digital health literacy and the skills required to effectively navigate complex patient portals and identify reliable health information 637172. The tertiary divide encompasses the unequal clinical benefits derived from technology, where identically deployed interventions consistently yield superior health outcomes for affluent, highly educated demographics compared to marginalized groups 6371.
Vulnerable populations - particularly older adults, racial and ethnic minorities, and rural residents - disproportionately experience the compounding effects of these divides 59616566. Research indicates that older adults frequently exhibit lower e-health literacy and higher technological anxiety, leading to frustration and disengagement from asynchronous care platforms and patient portals 29716566. Furthermore, the financial fragility of digital inclusion was underscored in 2024 when the Affordable Connectivity Program (ACP) subsidies lapsed in the United States, immediately resulting in a 13% drop-off in broadband connectivity among low-income households, severing their access to telehealth infrastructure 39. Dismantling the digital divide requires multi-sectoral strategies, including the development of offline-compatible health applications, targeted investments in digital literacy curricula, and the intentional integration of social determinants of health (SDOH) into algorithmic risk models to prevent digital redlining 536171726768.
Regulatory Governance and Algorithmic Vulnerability
Systemic Artificial Intelligence Risk in Clinical Infrastructure
As digital health platforms mature from isolated diagnostic aids into the foundational infrastructure of healthcare delivery, the sector confronts unprecedented risks associated with algorithmic vulnerability. Artificial intelligence is increasingly embedded into enterprise-wide triage systems, automated clinical decision support (CDSS), and cloud-based EHR platforms that serve hundreds of hospitals simultaneously 15164169.
This vendor-scale diffusion introduces the concept of "systemic healthcare AI risk" 69. Unlike a localized human error or a failure in a standalone device, a flaw in a widely deployed algorithm - whether stemming from dataset bias, covariate shift, concept drift, or out-of-distribution generalization - can trigger a cascade of clinical errors across entire populations and disparate hospital systems simultaneously 162069. Healthcare AI systems now function as critical cyber-physical systems (CPS), where algorithmic outputs directly influence physical clinical processes and resource allocation 69. Consequently, traditional regulatory frameworks, which historically focused on the localized validation of static software, are fundamentally inadequate for overseeing dynamic, continuously learning LLMs and machine learning algorithms 1569.
Emerging Regulatory Frameworks and Compliance Mandates
In response to these systemic vulnerabilities, global regulatory bodies are aggressively modernizing governance frameworks to enforce transparency, continuous monitoring, and accountability 15205570.
In Europe, the implementation of the EU AI Act (2024) established the world's most stringent regulatory mandates for high-risk medical AI 1520. The legislation requires developers to provide transparent disclosures regarding training data sources and demographic representation, ensures that human physicians retain ultimate decision authority and override capabilities, and mandates rigorous independent validation across diverse patient populations 20. Furthermore, it enforces continuous post-market monitoring and rapid adverse event reporting 20.
Concurrently, the United States Food and Drug Administration (FDA) is adapting its oversight through the transition to the Quality Management System Regulation (QMSR), which harmonizes U.S. device manufacturing with ISO 13485 standards, demanding rigorous lifecycle risk management for AI devices 1520. To bridge the gap between innovation and clinical utility, the FDA launched pilot programs such as TEMPO (Technology-Enabled Meaningful Patient Outcomes) in coordination with the Centers for Medicare & Medicaid Services (CMS). These initiatives offer pathways for enforcement discretion while developers collect real-world evidence to prove the clinical and economic validity of their AI models in exchange for modernized reimbursement codes 20.
At the global level, the World Health Organization continues to issue guidance mitigating the distinct risks of generative AI and large multi-modal models (LMMs). The WHO warns against the dangers of AI "hallucinations" - where models confidently generate false medical information - and highlights the risk of bias amplification when models trained predominantly on data from high-income nations are deployed in LMICs, underscoring the urgent need for context-specific validation and equitable digital governance 2049.
Ensuring that digital health platforms fulfill their disruptive potential - by demonstrably improving patient outcomes, reducing systemic expenditures, and universally democratizing access - requires more than rapid technological deployment. It necessitates the deliberate alignment of adaptable regulatory oversight, robust interoperability standards, and proactive health equity initiatives to secure the digital architecture of modern medicine 43617071.