Deliberate practice and minimum repetition in public speaking
The acquisition of expert performance in public speaking is frequently misunderstood as a byproduct of sheer experience or innate charisma. However, empirical research in cognitive psychology, motor learning, and communication pedagogy indicates that improvement in oral communication is governed by highly specific mechanisms of skill acquisition. Chief among these is the theory of deliberate practice, which distinguishes mere repetition from targeted, feedback-driven skill refinement. Concurrently, intervention literature across related disciplines - including clinical speech-language therapy, second language acquisition, and cognitive-behavioral exposure therapy - has quantified the "minimum effective dose" (MED) required to trigger measurable improvements in performance and fluency.
This research synthesizes the intersection of deliberate practice theory and public speaking, isolating the cognitive barriers to performance, the role of feedback mechanisms, the impact of cultural evaluation standards, and the precise dosage parameters required to optimize speech training.
Theoretical Foundations of Practice and Expertise
The scientific study of expertise centers heavily on the framework proposed by K. Anders Ericsson and colleagues in 1993, which revolutionized the understanding of skill acquisition by suggesting that expert performance is the result of prolonged, highly structured training rather than innate talent alone 123. To apply this framework to oral communication, it is necessary to differentiate between three distinct classifications of practice.
Naive, Purposeful, and Deliberate Practice
Skill acquisition exists on a continuum of intentionality and cognitive engagement. Ericsson distinguishes between naive practice, purposeful practice, and deliberate practice 343.
Naive practice consists of engaging in an activity repeatedly with the assumption that volume alone will yield improvement. In the context of public speaking, this mirrors a professional who frequently presents at meetings but does so without reflection, preparation, or targeted goals 34. While naive practice builds familiarity and basic automaticity, it quickly results in a performance plateau. Once an acceptable level of baseline competence is reached, additional years of routine practice do not yield further improvement, regardless of accumulated hours 47.
Purposeful practice introduces intentionality. It is characterized by specific, well-defined goals, intense focus, an element of feedback, and a requirement to push the learner outside their current comfort zone 347. A speaker engaging in purposeful practice might record their speech to specifically monitor and eliminate filler words, or actively solicit peer feedback after a presentation.
Deliberate practice represents the highest tier of skill acquisition. It builds upon purposeful practice but strictly requires a well-developed field with established, objective standards of performance and the guidance of an expert teacher or coach 17. The expert provides individualized diagnosis of errors, tailors remedial training tasks, and guides the sequential mastery of sub-skills 5.
| Practice Classification | Core Mechanism | Cognitive Engagement Level | Primary Feedback Source | Expected Performance Outcome |
|---|---|---|---|---|
| Naive Practice | Unstructured repetition | Low (Relying on automaticity) | None / Internal feeling | Early plateau; ingrained habits |
| Purposeful Practice | Goal-oriented repetition | High (Focused effort) | Self-monitoring / Recording | Incremental improvement |
| Deliberate Practice | Expert-guided sub-skill targeting | Very High (Maximum cognitive load) | External expert / Objective data | Continuous mastery; elite expertise |
Debates in Expertise Variance
While the deliberate practice framework is highly influential, its absolute dominance in explaining expertise has been heavily debated within the scientific community. A pivotal meta-analysis by Macnamara et al. (2014) reviewed 88 studies measuring accumulated practice and found that deliberate practice accounted for only 14% of the variance in overall performance, and as little as 1% in elite sports 15.
Ericsson and colleagues contested these findings, arguing that the meta-analysis conflated "structured practice" with strict deliberate practice, thereby including data where activities lacked expert supervision, immediate feedback, or specific goal orientation 35. When strict criteria are applied, the variance explained by deliberate practice increases significantly 5. For public speaking, this debate underscores a critical reality: simply accumulating hours on stage or practicing in isolation without an established pedagogical framework is insufficient for achieving elite communication competence. True deliberate practice requires isolating variables and receiving immediate, corrective data 39.
Cognitive Mechanisms of Public Speaking Anxiety
The application of deliberate practice to public speaking is uniquely complicated by the physiological and cognitive interference of public speaking anxiety (PSA). Studies consistently report that up to 75% of individuals experience some degree of anxiety when engaging in public speaking, making it one of the most prevalent barriers to communication mastery 1011.
Attention Control Theory and Cognitive Load
Attention Control Theory (ACT) provides a framework for understanding how anxiety impairs verbal communication. According to ACT, anxiety consumes working memory capacity, specifically the central executive system responsible for attentional control 67. Research demonstrates that under normal, low-stakes circumstances, anxiety and verbal performance are largely unrelated. However, under conditions of significant cognitive load - such as delivering an extemporaneous speech while navigating audience reactions - anxiety and performance become inversely related 6.
The cognitive demands of public speaking are formidable; speakers must simultaneously manage self-presentation, linguistic retrieval, narrative structure, and audience feedback 7. Unintentional breaks in focus at inopportune times consume further cognitive resources. Studies indicate that individuals with high self-reported attentional control capacity possess a cognitive buffer that protects against the detrimental effects of PSA, allowing them to maintain speech length and quality despite physiological arousal 7.
Dimensions of Public Speaking Anxiety
Public speaking anxiety manifests across three primary dimensions: cognitive, physiological, and behavioral 10. Comparative analyses consistently show that the cognitive component is the most dominant factor.
| PSA Dimension | Mean Impact Score (Out of 5) | Primary Manifestations | Mechanism of Interference |
|---|---|---|---|
| Cognitive | 3.4 | Fear of negative evaluation, forgetting lines, self-doubt. | Consumes working memory; disrupts attentional control 1011. |
| Behavioral | 3.2 | Shaking hands, fidgeting, speech avoidance, truncation. | Alters nonverbal delivery; prevents exposure therapy 1014. |
| Physiological | 3.1 | Elevated heart rate, sweating, flushing, vocal tremors. | Triggers fight-or-flight response; disrupts respiratory pacing 1011. |
Speakers report that the fear of negative evaluation, the fear of forgetting lines, and intrusive self-doubt impact their performance more severely than physiological symptoms 1014. However, physiological responses - which are natural chemical processes triggered by the novelty or uncertainty of the speaking environment - disrupt the speaker's ability to maintain optimal respiratory control and vocal pacing 1114.
Cultural Context and Normative Standards
A foundational requirement of deliberate practice is an established body of knowledge regarding what constitutes "expert performance" 7. In public speaking, this standard is highly culturally dependent, complicating the objective measurement required to guide deliberate practice.
Western communication norms generally represent "low context" cultures, prioritizing directness, succinct articulation, and sustained eye contact as indicators of confidence and competence 15168. In contrast, Eastern communication styles often reflect "high context" cultures, where meaning is implicit, collective harmony is prioritized over individual assertion, and sustained eye contact may be interpreted as aggression or disrespect 1516.
Critical discourse analysis of public speaking pedagogy indicates that the standard rubrics used to evaluate "competent" speaking heavily favor White, Western, Standard American English norms 91011. The National Communication Association's (NCA) standards for public speaking competency emphasize "suitable" and "appropriate" forms of communication that implicitly code the ideal competent speaker as White and Western 911. Consequently, when applying deliberate practice to public speaking, practitioners must contextualize the target outcome. If the feedback mechanism exclusively rewards low-context, direct communication, it may inadvertently penalize speakers from high-context backgrounds, misdiagnosing cultural communication differences as a lack of fluency or confidence 151012.
Sub-Skill Deconstruction and Targeted Acquisition
To transition from naive repetition to deliberate practice, public speaking must be deconstructed into isolatable sub-skills that can be drilled, measured, and refined. Expert speakers do not practice "being a better communicator" as a monolithic task 49.
Component Isolation and Neural Circuit Specialization
The deliberate practice framework dictates segmenting the presentation into individual, highly specific components. A comprehensive practice regimen isolates distinct elements such as the opening hook, storytelling pacing, visual slide integration, vocal modulation, and movement 4.
By focusing on a single sub-skill (e.g., delivering a compelling topic sentence within the first thirty seconds), the practitioner reduces overall cognitive load, establishes clear metrics for success, and accelerates the myelination of task-relevant neural circuits 49. This intense, localized focus operates just beyond the speaker's current ability level, ensuring that the practice remains effortful rather than automatic 39. Research indicates that practicing specific communication skills - such as asking open questions or maintaining narrative structure - yields significantly higher improvement rates (up to 41%) compared to passive learning or generalized rehearsal 22.
The 4/3/2 Fluency Technique
One of the most empirically validated frameworks for structured speaking repetition is the "4/3/2 technique." Originally developed to build oral fluency in second-language learners, this method requires the speaker to deliver the same monologue three consecutive times, but with a decreasing time constraint: first in four minutes, then three minutes, and finally two minutes 231314.
The progressive reduction in available time forces an increase in the rate of speech and drastically reduces unfilled pauses, hesitations, and the cognitive urge to introduce new, tangential information 2313. By the third iteration, the cognitive load dedicated to message formulation is minimized, allowing the speaker to allocate working memory entirely to delivery, articulation, and prosody 1314.
| Iteration | Time Limit | Cognitive Focus | Observed Performance Outcomes |
|---|---|---|---|
| First | 4 Minutes | Message formulation; structural organization. | High rate of hesitations; moderate fluency; cognitive load is heavily taxed 2314. |
| Second | 3 Minutes | Message refinement; elimination of tangential data. | Increased speech rate; reduced unfilled pauses; improved lexical recall 2313. |
| Third | 2 Minutes | Articulation, prosody, and delivery mechanics. | Peak automaticity; high confidence; seamless chunking of information 1314. |
Studies demonstrate that the 4/3/2 technique yields statistically significant improvements in automaticity, lexical recall, and speaker confidence compared to unstructured group discussions or standard rehearsal 2314.
The Minimum Effective Dose of Speaking Repetition
In pharmacology and exercise science, the Minimum Effective Dose (MED) is the lowest volume of an intervention required to achieve a clinically significant or meaningful outcome 151617. Translating this concept to behavioral and cognitive domains requires examining the minimum volume, frequency, and intensity of practice required to elicit neuroplastic adaptation and performance improvement without triggering cognitive fatigue 1718.
Dose-Response Relationships in Speech Motor Learning
Because public speaking relies fundamentally on speech-motor execution and linguistic retrieval, data from clinical speech-language pathology (SLT) provides a rigorous empirical foundation for establishing speaking dosage. Research consistently demonstrates a positive dose-response relationship in speech therapies; greater practice volume generally yields better outcomes, but this relationship is highly non-linear 192021.
In the treatment of speech sound disorders and aphasia, the optimal treatment dose (the number of teaching episodes or speech productions per session) is typically identified as 50 to 100 targeted productions per session 2223. A session characterized by high-frequency repetition (e.g., 100+ productions in 15 minutes) leads to higher in-session accuracy and greater generalization effects than moderate-frequency sessions (30-40 productions), primarily due to the intensity and pace of the neural activation 2425.
Repetition Ceilings and Diminishing Returns
While repetition is essential, research into oral task performance identifies a definitive ceiling effect regarding the number of optimal practice iterations. Studies analyzing immediate aural-oral repetition of communication tasks found that speech rate, fluency, and complexity improve significantly across the first few performances 2627.
Specifically, the largest gains in speech fluency occur between the first and third repetitions 27. Improvements continue, albeit marginally, through the fourth and fifth repetitions. However, beyond the fifth repetition of the exact same task, performance stabilizes, and no statistically significant improvements in speech rate or fluency are observed 2627.
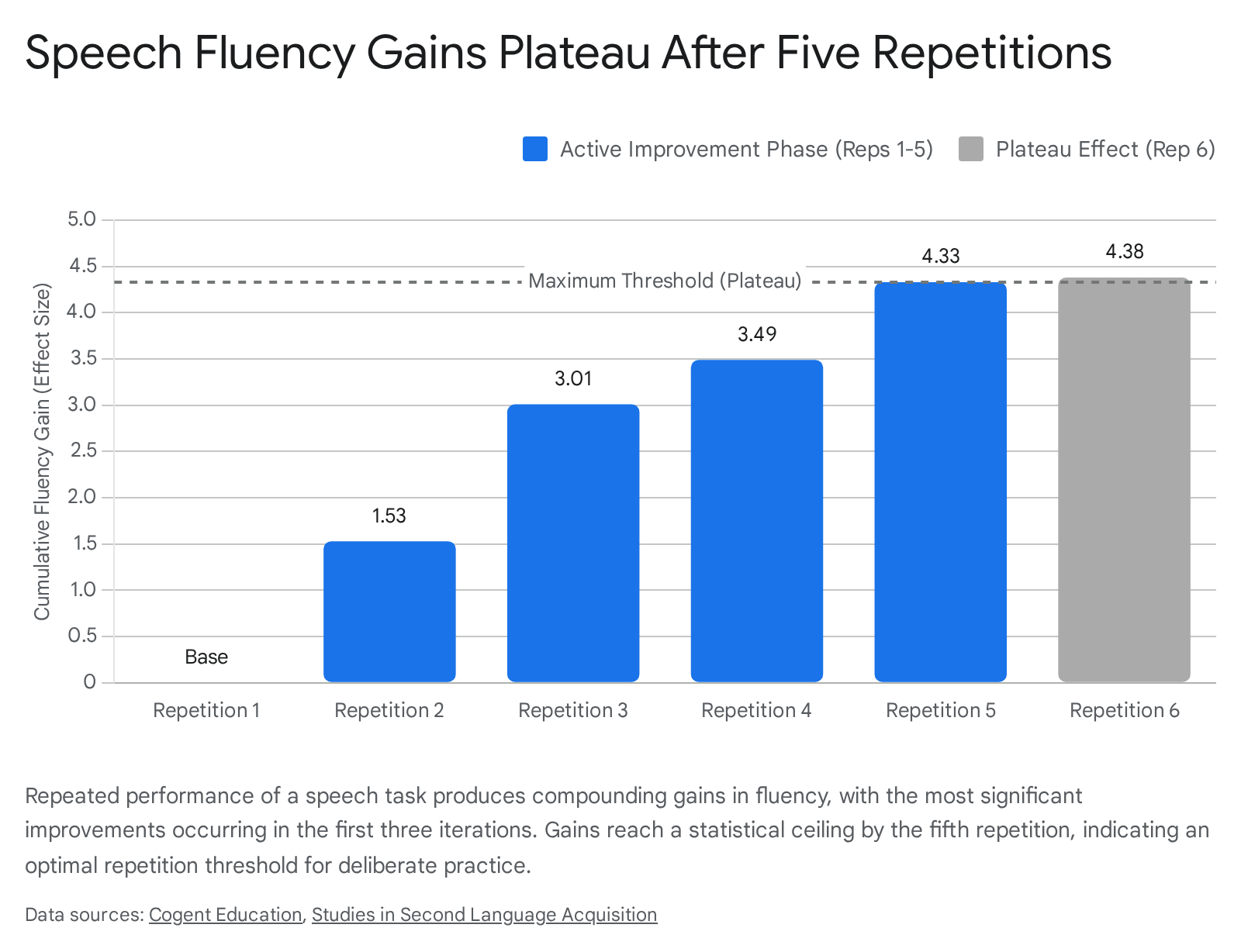
This data strongly suggests that the MED for isolated speech segment rehearsal is approximately three to five repetitions. Practicing a specific sub-skill or speech segment more than five times in a single session violates the principles of efficient deliberate practice and crosses into the realm of naive practice with diminishing returns 2627.
Frequency, Duration, and Micro-Dosing
When evaluating the optimal duration and frequency of practice sessions, longitudinal data from digital, self-managed speech therapies reveal critical thresholds. A large-scale analysis of post-stroke survivors using a digital speech therapy application found that maintaining 15 to 40 minutes of active practice per week produced significantly larger average improvements in communication scores than practicing for fewer than 15 minutes 2829.
Crucially, the data indicated a distinct plateau effect: while practicing more than 40 minutes per week (up to 60 minutes) yielded modest additional benefits, there were clear diminishing returns beyond the 60-minute mark 2829. Regarding frequency, practicing speech tasks across multiple days (e.g., 3 to 5 days a week) resulted in significantly greater skill acquisition than massing the practice into a single weekly session 283031.
For the physiological management of Public Speaking Anxiety, the MED requires as little as 2 to 5 minutes of daily diaphragmatic breathing (such as the 4-7-8 technique) to habituate the nervous system prior to entering high-stakes environments 43. When acute medication is required to facilitate exposure therapy, beta-blockers (such as Propranolol at a dosage of 10-40mg) are utilized specifically to suppress the physiological fear response, allowing the speaker to practice within a manageable anxiety range (a 4-6 on a 10-point scale) 44. This pharmacological intervention does not replace practice; rather, it acts as a stabilizing mechanism, enabling the speaker to complete the required 3 to 5 weekly exposure sessions necessary for long-term fear extinction 44.
Virtual Reality and Objective Feedback Mechanisms
The primary bottleneck in applying true deliberate practice to public speaking has historically been the availability of expert coaching to provide immediate, corrective feedback 9. Without feedback, practice remains merely purposeful at best. Furthermore, the condition of the rehearsal alters the dosage efficacy. Students who practiced their presentations in front of an actual, live audience received significantly higher performance evaluations than those who rehearsed identically but in isolation 32.
Immersive Habituation and Cognitive Load Testing
Recent advancements in Virtual Reality (VR) and Artificial Intelligence (AI) have revolutionized the feedback loop and environmental simulation. VR public speaking platforms simulate high-fidelity environments - such as lecture halls and boardrooms - complete with audience distractions, allowing for realistic cognitive load testing 463334.
These immersive environments facilitate fear extinction and habituation by directly addressing the physiological components of PSA in a low-stakes setting 495035. A 2023 study by Kroczek & Mühlberger demonstrated that practicing in front of a supportive VR audience significantly improved subjective self-efficacy and objective, observer-rated confidence during subsequent real-world presentations 3435.
AI-Driven Objective Measurement
Beyond environmental simulation, digital platforms integrate AI-driven speech coaching that provides zero-latency, objective feedback on vocal tone, pace, filler word frequency, and nonverbal cues 46365354. Advanced on-device voice AI processing eliminates cloud latency, allowing users to receive real-time coaching prompts (e.g., "slow down," "avoid filler words") while maintaining data privacy 53.
This technology fulfills the core requirements of deliberate practice by providing objective measurement of errors and facilitating remedial repetition. Users can immediately replay the scenario, implementing the AI feedback in real-time to correct the isolated deficiency 3655.
Conclusion
The application of deliberate practice to public speaking requires moving beyond naive repetition and embracing a structured, metrics-driven approach to skill acquisition. Public speaking anxiety, which primarily disrupts cognitive working memory, must be managed through systematic exposure and physiological regulation. Furthermore, the standard of "expert performance" must be carefully contextualized to account for cultural variations in high- and low-context communication styles.
Based on empirical data spanning motor learning, speech-language therapy, and communication pedagogy, the optimal framework for public speaking improvement relies on consistent micro-dosing. The minimum effective dose consists of 15 to 40 minutes of weekly practice, distributed across 3 to 5 days, with isolated speech segments rehearsed no more than 3 to 5 times per session to avoid cognitive diminishing returns. By leveraging techniques such as the 4/3/2 fluency model and utilizing VR environments for objective, zero-latency feedback, practitioners can successfully translate the mechanics of deliberate practice into measurable public speaking mastery.