Complicated Grief vs. Normal Grief: What's the Difference
Complicated grief, clinically formalized as prolonged grief disorder, occurs when the intense, disabling pain of a loss remains at peak levels for months or years, severely impairing daily life. While normal grief comes in oscillating waves that gradually allow the bereaved to integrate the loss and rebuild their lives, complicated grief traps the brain in a persistent state of yearning and addiction-like craving for the deceased.
The Myth of the Five Stages: Redefining Normal Grief
For decades, the public understanding of mourning has been dominated by a single framework: the "Five Stages of Grief," consisting of denial, anger, bargaining, depression, and acceptance. However, modern bereavement researchers and clinical psychologists have thoroughly debunked the idea that grief is a linear, step-by-step process 12.
This widely misunderstood framework was introduced in 1969 by Swiss-American psychiatrist Elisabeth Kübler-Ross in her landmark book On Death and Dying. Crucially, this model was developed based on interviews with patients facing their own terminal illnesses, not individuals who had lost a loved one 233. The model was never intended to serve as a sequential roadmap for the bereaved. Empirical studies monitoring the trajectory of widowed individuals have repeatedly failed to find evidence that grieving people move through these discrete stages in a predictable order 23. In fact, Kübler-Ross herself later expressed regret that her framework was misinterpreted as a strict chronological progression 3.
When grieving individuals believe they must complete specific stages to achieve a mythical state of "closure," it can create unnecessary psychological pressure. Survivors often feel a sense of failure or assume they are grieving incorrectly when their emotional reality does not match the five-stage model 14. Furthermore, telling a griever that they are simply in the "depression stage" can inadvertently serve as a roadblock to seeking actual mental health support, as it frames persistent, debilitating despair as a mandatory hurdle rather than a condition requiring intervention 3.
The Dual Process Model of Coping
Instead of a straight line, healthy mourning is better understood as an ongoing, fluid oscillation. In 1999, psychologists Margaret Stroebe and Henk Schut introduced the "Dual Process Model of Coping with Bereavement," which remains a foundational concept in the scientific understanding of normal grief 56.
This model posits that healthy adaptation to loss requires a person to constantly swing back and forth between two distinct modes of coping. The first mode is loss-oriented coping, which involves facing the emotional pain directly. This encompasses behaviors such as crying, looking at old photographs, intensely yearning for the deceased, and cognitively processing the profound weight of the absence 678. The second mode is restoration-oriented coping, which involves adjusting to the new reality. This encompasses engaging with the outside world, taking on new household or financial roles, returning to work, socializing with friends, and finding moments of distraction or joy 67.
Normal grief is characterized by this healthy rhythm. A person might spend the morning sobbing heavily over a memory, yet genuinely laugh with a friend over dinner that same evening 710. This oscillation prevents emotional burnout and allows the bereaved to integrate the loss into their life in tolerable increments 5810. Problems arise when a person becomes entirely stuck in one mode - particularly the loss-oriented mode - rendering them unable to access the restoration-oriented tasks necessary for psychological survival and adaptation 78.
The Statistical Trajectories of Bereavement
Because the Dual Process Model acknowledges that grief fluctuates, researchers have mapped how these fluctuations trend over time to distinguish normal adaptation from pathological responses. By tracking bereaved individuals for up to three years post-loss using growth mixture modeling, empirical studies have identified four distinct emotional trajectories 910.
An analysis of these trajectories demonstrates that severe, unyielding grief is a statistical anomaly, occurring in only a small fraction of the bereaved population.
| Trajectory Type | Estimated Prevalence | Description of Grief Course |
|---|---|---|
| Resilience | 26% - 45% | The most common outcome following a loss. Individuals experience a brief period of acute sadness but maintain stable, low levels of clinical grief symptoms and quickly return to baseline functioning 910. |
| Moderate-Improving | 30% - 33% | Individuals experience moderate to high levels of acute grief immediately after the death. Over a period of several months to a year, their symptoms steadily decline without clinical intervention 910. |
| Delayed Grief | ~10% | A smaller subgroup initially presents with relatively low levels of grief immediately following the death, but experiences an unexpected spike in distress roughly six months post-loss 9. |
| Prolonged-Stable | 7% - 10% | Individuals experience intense, disabling grief immediately after the loss that does not improve. Their symptom trajectory remains flat and highly elevated for years, representing the clinical threshold for complicated grief 910. |
This data indicates that the vast majority of human beings possess a profound psychological resilience following traumatic loss. Complicated grief, characterized by the "Prolonged-Stable" trajectory, is distinct because time alone fails to act as a healing mechanism.
Defining Complicated Grief (Prolonged Grief Disorder)
When the oscillation between loss-oriented and restoration-oriented coping breaks down entirely, a person may be experiencing complicated grief. After decades of scholarly debate regarding the terminology - previously referred to as persistent complex bereavement disorder or traumatic grief - the condition was officially recognized as "Prolonged Grief Disorder" (PGD) in the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Text Revision (DSM-5-TR) in 2022, following its formal inclusion in the World Health Organization's International Classification of Diseases (ICD-11) 7111213.
The fundamental difference between normal and complicated grief is not determined by the depth of love the survivor held for the deceased, nor is it measured simply by the presence of sadness. Normal grief can be incredibly painful and highly disruptive in the short term. The defining separator is the trajectory and the long-term impact on functionality 7. In normal mourning, acute pain eventually integrates into the survivor's evolving identity, allowing them to envision a meaningful future. In prolonged grief disorder, the acute pain remains frozen, and the individual suffers a profound identity disruption, often feeling that a vital part of themselves has died alongside their loved one 141516.
Diagnostic Algorithms: DSM-5-TR vs. ICD-11
While both major psychiatric manuals now recognize Prolonged Grief Disorder, they utilize different diagnostic algorithms. These variations are significant because they directly impact the prevalence rates of the disorder in clinical settings. Studies evaluating populations in Germany and the United States have consistently demonstrated that applying the ICD-11 criteria yields a substantially higher prevalence rate of PGD than the stricter DSM-5-TR criteria 111718.
| Diagnostic Criterion | DSM-5-TR (American Psychiatric Association) | ICD-11 (World Health Organization) |
|---|---|---|
| Time Threshold | Symptoms must persist for at least 12 months post-loss for adults (6 months for children) 719. | Symptoms must persist for an atypically long period, at least 6 months post-loss 719. |
| Core Symptoms | Requires intense yearning/longing OR persistent preoccupation with the deceased 518. | Requires intense longing OR persistent preoccupation with the deceased 1920. |
| Accessory Symptoms | Requires at least 3 out of 8 specific accessory symptoms to a functionally impairing degree 518. | Requires any 1 of 10 accessory symptoms to a functionally impairing degree 1819. |
| Cultural Caveat | Reaction must clearly exceed expected social, cultural, or religious norms 19. | Reaction must clearly exceed expected social, cultural, or religious norms 1921. |
Harmonizing these two diagnostic sets remains a priority for the psychiatric community to prevent overdiagnosis while ensuring those suffering from debilitating grief receive adequate care 1118.
Recognizing the Red Flags in Daily Life
For the general public, understanding complicated grief requires looking beyond clinical manuals to observe how the condition manifests in daily life. Those suffering from PGD often exhibit severe behavioral blockages. To prevent overwhelming emotional pain, an individual might actively avoid all reminders of the deceased, refusing to visit certain locations or speak the person's name 2223. Conversely, they may exhibit intense preoccupation, leaving the deceased's belongings exactly as they were prior to the death and refusing to alter the physical environment for years 1523.
Cognitively, the persistent physiological stress of complicated grief drastically affects executive function, leading to a phenomenon colloquially known as "grief brain fog" 24. Because grief acts as a full-body stress event, the nervous system remains stuck in a heightened state of sympathetic arousal. This chronic stress, heavily compounded by the severe sleep deprivation common in bereavement, narrows attention and impairs working memory 24. Survivors may frequently lose their train of thought mid-sentence, forget routine appointments, and find themselves completely unable to track multi-step tasks at work or home 24.
While mild cognitive impairment and distraction are highly common in the early stages of acute grief, their persistence beyond a year is a critical red flag. When this cognitive fog is accompanied by severe emotional detachment, extreme isolation, a sense of meaninglessness, or an inability to return to baseline occupational functioning, it strongly indicates the presence of Prolonged Grief Disorder rather than a natural healing process 162224.
The Neurobiology of the "Stuck" Brain
Why does the brain get trapped in a state of complicated grief while others adapt? Recent neuroimaging studies have provided fascinating insights into the biological underpinnings of loss, revealing that prolonged grief is intimately tied to a dysfunction in the brain's reward-learning circuitry 72526.
When human beings form deep attachments, the brain physically encodes this bond. The presence of a loved one - or even visual and auditory reminders of them - triggers the release of feel-good neurotransmitters. Over years of connection, the brain builds an internal predictive model that constantly expects this person to be available to provide comfort and co-regulation 72529.
Following a death, the brain faces an impossible physiological task: updating this deeply ingrained predictive model to reflect a permanent absence. In normal grief, the painful reality of the loss gradually reshapes these neural pathways through neuroplasticity. However, in complicated grief, neuroimaging reveals a distinct and problematic neural signature 72527.
When bereaved individuals are shown photographs of their deceased loved ones while inside functional magnetic resonance imaging (fMRI) scanners, both normal grievers and those with PGD show immediate activation in the brain's pain networks, specifically the dorsal anterior cingulate cortex (dACC) and the insula 252628. This confirms that reminders of the deceased are universally painful. However, pioneering research conducted by Dr. Mary-Frances O'Connor revealed that only individuals diagnosed with complicated grief showed significant, ongoing activation in the nucleus accumbens 252628.
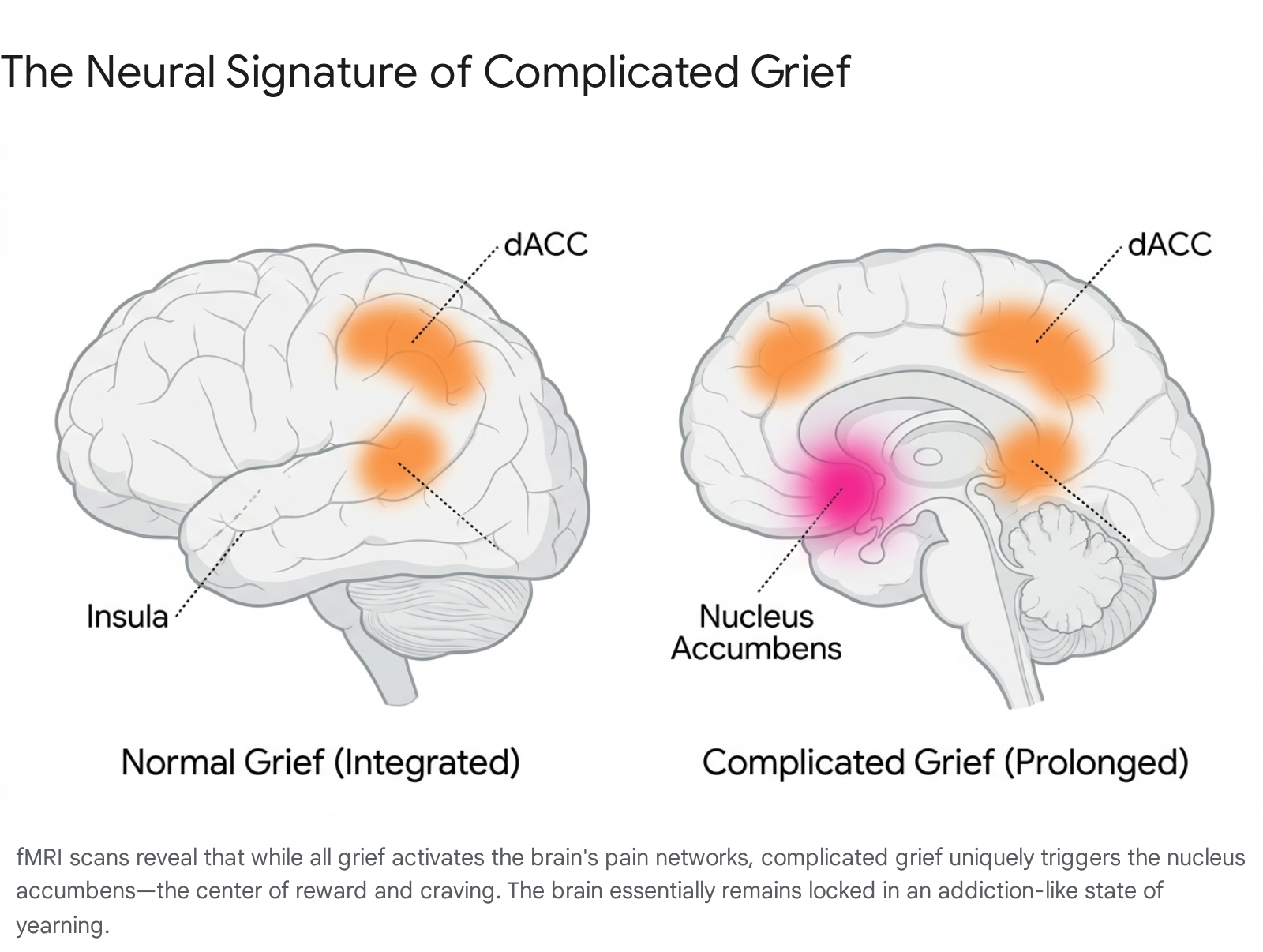
The nucleus accumbens is a central node in the brain's reward and craving system. It is the exact same region that activates when a person craves an addictive substance, smells food when severely hungry, or feels intense romantic attraction 2527. In complicated grief, this craving signal remains firing at full intensity 2527. The brain's reward system essentially refuses to update; it continues fiercely searching for the deceased, expecting the reward of their presence. When this neurological expectation inevitably collides with the physical reality of the death, it generates massive "prediction errors" that manifest as acute, relentless emotional pain 725. Because the underlying neural mechanisms overlap so heavily, the sensation of complicated grief can feel and function remarkably similarly to the neurobiology of severe addiction withdrawal 7262930.
The Medicalization Debate: Are We Pathologizing Love?
The formal inclusion of Prolonged Grief Disorder in the DSM-5-TR and ICD-11 was not without immense controversy. It reignited a fierce, decades-long debate within psychiatry, psychology, and sociology regarding the progressive "medicalization" of the human experience 121331.
Critics of the diagnosis argue that grief is a fundamental, inescapable part of the mammalian experience - a necessary emotional cost of our biological capacity to form strong attachments 32. Prominent figures in the field, including Dr. Allen Frances, the former chair of the DSM-IV task force, have been highly critical of codifying grief as a mental disorder. Critics argue that medicalizing grief inherently stigmatizes a natural process, strips dignity from the survivor's pain, and ignores the deep existential reality of human loss 2932. Opponents fear that establishing rigid timelines, such as the six or twelve-month thresholds, risks creating false epidemics of mental illness. They warn this could funnel naturally grieving individuals toward unnecessary pharmaceutical interventions, overriding reliance on community support and time-honored cultural mourning rituals 293233.
Conversely, proponents of the PGD diagnosis emphasize that while grief is universal, prolonged and functionally disabling grief is statistically abnormal 34. Because only an estimated 7% to 10% of the bereaved suffer from this specific, unyielding trajectory, diagnosing it does not pathologize normal love 934. Advocates assert that giving this severe suffering a formal clinical name is a necessary act of compassion. It allows highly distressed, functionally impaired individuals to access health insurance coverage, receive specialized care, and find validation that their chronic inability to function is a recognized condition with a path to treatment, rather than a personal failure 71234.
Cross-Cultural Blind Spots in Diagnosis
A major compounding factor in the medicalization debate is the stark cultural bias present in current diagnostic criteria. While the emotional response to loss is a universal human experience, the diagnostic parameters for Prolonged Grief Disorder are overwhelmingly rooted in Western empirical data and individualized psychological norms 1935. This has sparked grave concern among global mental health experts regarding the cross-cultural validity of the diagnosis 193536.
Expressions of grief, acceptable duration of mourning, and behavioral expectations vary vastly across the globe. Therefore, defining what constitutes an "atypically long" or "abnormal" grief response is highly dependent on cultural context: * Duration of Mourning: In modern Western societies, an expectation exists that the most acute phases of grief will subside within a year. However, traditional Chinese culture may prescribe a dedicated mourning period lasting up to three years 3537. Conversely, the Navaho culture restricts outward expressions of grief to just four days, after which speaking of the deceased or showing extreme sadness is actively discouraged 19. In Bali, mourning rituals can extend up to ten years after a loss 35. * Emotional vs. Somatic Expression: Western psychology often frames grief strictly as a set of emotional and cognitive symptoms (e.g., sadness, yearning). However, in Chinese populations, grief is frequently somatized - expressed intensely through physical bodily distress, such as chronic back pain, stomach issues, and headaches. Current Western diagnostic tools often fail to capture these physical symptoms adequately, risking misdiagnosis 193536. * Behavioral Norms: In many European and American cultures, open sadness is the expected norm for mourning. However, the Kaluli tribe of New Guinea culturally responds to loss with outward anger directed toward finding compensation rather than internalizing guilt 19. In Balinese culture, public mourning rituals can involve laughter and cheerfulness, masking the individual's internal distress to prioritize communal harmony 19.
To account for these stark differences, both the DSM-5-TR and ICD-11 include a crucial caveat: to diagnose PGD, the reaction must clearly exceed the expected social, cultural, or religious norms for the individual's specific context 1921. Nonetheless, transcultural researchers advocate heavily for the development of "emic" measures - diagnostic tools developed organically from within specific cultures. Forcing Western "etic" tools onto global populations currently risks pathologizing culturally appropriate mourning behaviors 2036.
Evidence-Based Treatments for Prolonged Grief
Because complicated grief represents a distinct psychological and neurobiological state, it requires distinct therapeutic interventions. Historically, bereaved individuals suffering from severe, long-term distress have been prescribed antidepressants or directed toward general supportive counseling. However, rigorous clinical trials have consistently shown that medications like selective serotonin reuptake inhibitors (SSRIs), such as citalopram, do not significantly alleviate the core symptoms of PGD, particularly the intense yearning for the deceased 273839. While medication may be helpful if the patient is suffering from co-occurring major depressive disorder, it is generally ineffective as a standalone treatment for complicated grief 3840.
Because complicated grief involves severe cognitive blockages and deep-seated avoidance behaviors, specialized psychotherapies are required to help the brain update its predictive models.
Prolonged Grief-Specific Cognitive Behavioral Therapy (PG-CBT)
Extensive clinical research indicates that targeted, grief-focused cognitive behavioral therapies are highly efficacious for treating PGD 3941. Traditional CBT is modified into PG-CBT (also known as Complicated Grief Treatment), which blends standard cognitive restructuring with narrative and exposure techniques 4243.
A critical component of this specialized treatment involves "exposure therapy" directly targeted at the memories of the death. Bereaved individuals with complicated grief often expend massive amounts of cognitive energy avoiding reminders of the loss. By having the patient confront the reality of the loss and narrate the specific, often painful circumstances of the death in a safe clinical environment, the brain is forced to process the reality it has been avoiding 4243. A major multi-center study published in JAMA Psychiatry demonstrated that PG-CBT led to significantly greater reductions in PGD severity compared to present-centered therapy (which focuses purely on general emotional support). Furthermore, long-term follow-ups show that adding exposure techniques to CBT yields additive gains that extend years after the treatment is complete 394243.
Mindfulness-Based Therapies
For individuals highly reluctant to engage in the emotionally demanding exposure aspects of CBT, mindfulness-based therapy has emerged as a viable, evidence-based alternative. Recent clinical trials conducted in Australia evaluated the efficacy of CBT against mindfulness therapies for treating PGD. The results indicated that while CBT provided the most enduring, long-term symptom relief, mindfulness therapies successfully helped patients tolerate acute grief-related distress and effectively break the immediate cycle of rumination 14.
Crucially, none of these therapies aim to make the patient "forget" the deceased or sever their attachment. Instead, the clinical goal is to shift the patient out of the neurobiological paralysis of complicated grief and back into the healthy, natural oscillation of the Dual Process Model. This allows the survivor to honor the memory of the deceased while successfully restoring their engagement with the living future 710.
Bottom line
Complicated grief, recognized clinically as Prolonged Grief Disorder, is a severe condition where the natural oscillation of mourning stalls, leaving a person functionally impaired and trapped in a state of intense, unyielding yearning for more than a year. Neuroimaging reveals this state is directly linked to the brain's reward circuitry, which acts similarly to addiction withdrawal by failing to adapt to the reality of the loss. While the formal medicalization of grief remains heavily debated - especially regarding its application across diverse cultural norms - identifying the condition has proven vital for connecting suffering individuals with specialized, highly effective cognitive behavioral therapies that allow them to rebuild their lives.