Neurobiology and Psychology of Grief
Bereavement represents one of the most profound physiological and psychological stressors a human being can endure. Historically, the scientific understanding of how the mind and body adapt to the permanent loss of an attachment figure was dominated by psychoanalytic interpretations and heuristic observational models. For decades, grief was broadly categorized as a transient emotional state characterized by sequential psychological stages that inevitably culminated in resolution. However, contemporary research across neuroscience, clinical psychology, and psychoneuroimmunology has driven a radical paradigm shift.
Today, grief is understood not merely as a passive emotional reaction, but as a complex, extended biological and cognitive learning process driven by neuroplasticity. When a primary attachment bond is severed by death, the brain is forced to update its fundamental predictive models of the social environment. This transition requires the extensive rewiring of neural circuits associated with reward, memory, and emotional regulation 112. Furthermore, grief extends far beyond the brain, acting as a systemic stressor that triggers profound neuroendocrine and immunological cascades, altering everything from inflammatory cytokine production to epigenetic aging markers 345.
While the vast majority of bereaved individuals exhibit a remarkable biological and psychological capacity for resilience, a significant minority experience a stalling of this neurobiological adaptation, resulting in severe, unremitting distress. This maladaptive trajectory has recently been codified in the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) and the World Health Organization's International Classification of Diseases, 11th Revision (ICD-11) as Prolonged Grief Disorder (PGD) 678.
This comprehensive report synthesizes the contemporary science of grief. It explores the distinct brain networks and structures involved in bereavement, the neuroplastic mechanisms driving adaptation, the formalization of PGD, and the profound influence of cross-cultural frameworks on biological resilience trajectories.
1. Debunking Foundational Misconceptions in Bereavement Science
To accurately interpret the modern neurobiology of grief, it is first necessary to address and dismantle two pervasive misconceptions that have historically distorted both clinical practice and public perception. These are the myth that grief operates on a predictable timeline or in sequential stages, and the myth that a lack of profound, extended distress implies a pathological lack of attachment.
The Myth of Predictable Timelines and Sequential Stages
The most deeply entrenched misconception in bereavement science is the "Five Stages of Grief" model - comprising denial, anger, bargaining, depression, and acceptance - originally introduced by Swiss-American psychiatrist Dr. Elisabeth Kübler-Ross in 1969 91012. Although originally formulated based on qualitative interviews with terminally ill patients confronting their own mortality, the model was rapidly co-opted by popular psychology and misapplied to the bereavement process of survivors 1012.
Rigorous scientific inquiry over the past two decades has repeatedly debunked the empirical validity of the stage model. Large-scale longitudinal studies of bereaved individuals have found no evidence of uniform, sequential emotional stages 912. Instead, grief is a non-linear, oscillating, and highly individualized process. Kübler-Ross herself noted that the stages were merely a heuristic device and that emotional responses are fluid, overlapping, and often missed altogether 1012. However, the persistence of the stage model in public consciousness has inadvertently created unrealistic expectations, leading many bereaved individuals to feel that they are grieving "incorrectly" if they do not follow a prescribed emotional sequence 1211. Experts in contemporary psychopathology and clinical psychology widely advocate for the retirement of the stage model from clinical bereavement practice due to its lack of theoretical underpinning and empirical support 1012.
The Myth that Resilience Indicates a Lack of Attachment
A second critical misconception assumes that profound, debilitating, and extended distress is the only normative response to the death of a close loved one. Consequently, individuals who maintain their daily functioning or display positive emotions shortly after a loss have historically been viewed with clinical suspicion. In traditional psychoanalytic models, this absence of overt distress was often labeled as "delayed grief" or viewed as a pathological repression of emotion 1215.
Empirical evidence entirely contradicts this assumption. The absence of prolonged trauma symptoms or acute grief does not equate to a lack of attachment or love; rather, it is indicative of natural human resilience 1011. Resilience is not the evasion of pain, but the biological and psychological capacity to maintain a stable equilibrium and generative functioning despite the presence of sadness 1115.
Research into adult attachment styles further illuminates this dynamic. Individuals classified with a "dismissing-avoidant" attachment profile - characterized by high avoidance but low anxiety - are often stereotyped as emotionally detached. However, longitudinal studies of bereaved spouses and parents reveal that these individuals frequently exhibit a highly adaptive pattern of resilience to loss. They report fewer symptoms of depression and post-traumatic stress, and their recovery trajectories mirror those of securely attached individuals 131419. This directly challenges the traditional belief that emotional avoidance inherently leads to delayed pathological adjustment. A dismissing-avoidant style allows these individuals to regulate attachment-related distress effectively, relying on internal coping mechanisms to maintain functionality 1419. Thus, a lack of overt psychological breakdown is an empirically validated indicator of psychological strength, not an emotional deficit.
2. Comparing the Conceptual Frameworks of Grief
The evolution of bereavement science can be understood by comparing three distinct conceptual frameworks that have dominated the literature over the last century: the Kübler-Ross stages model, George Bonanno's empirical resilience trajectories, and Mary-Frances O'Connor's neurobiological mapping model.
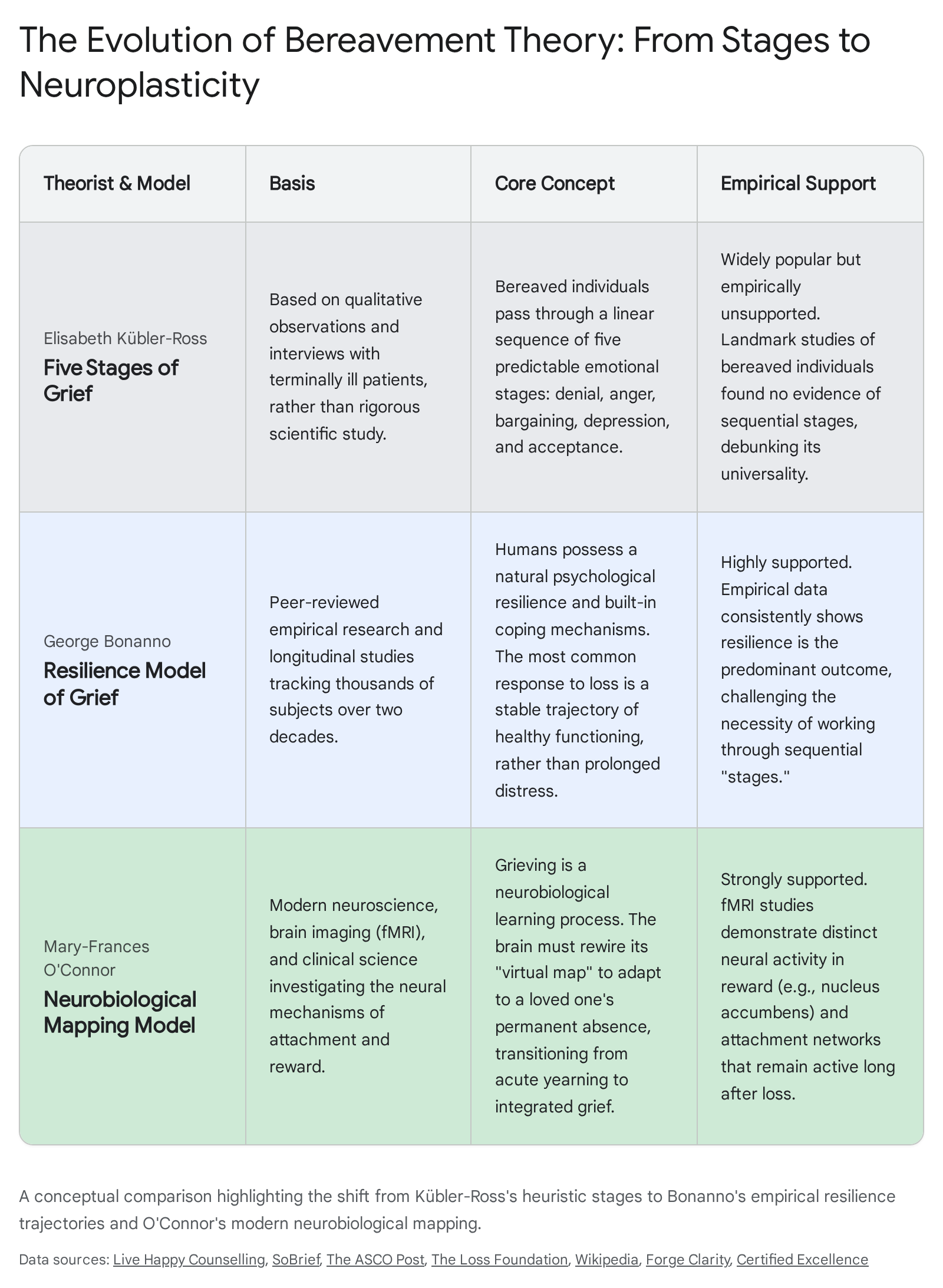
Kübler-Ross's Qualitative Heuristic
As noted, the Kübler-Ross model was initially conceived as a heuristic device to describe the emotional reactions of patients confronting terminal illness 1012. Its conceptual basis relies on qualitative observations of subjective distress. While Kübler-Ross acknowledged the fluidity of emotional states, the framework fundamentally conceptualizes grief as a series of emotional hurdles to be cleared, culminating in an endpoint of "acceptance" 10. It lacks a biological mechanism and fails to account for the vast individual differences in attachment, coping, and sociocultural context. Modern analysis views it primarily as a historical artifact that lacks predictive power.
Bonanno's Empirical Resilience Trajectories
In stark contrast to stage-based assumptions, George Bonanno's Resilience Model of Grief was derived from thousands of subjects evaluated over two decades using rigorous longitudinal and empirical methodologies 91012. Bonanno mapped the actual behavioral and psychological outcomes of bereavement over time, identifying four primary, statistically distinct trajectories 2015:
| Grief Trajectory | Prevalence & Characteristics | Psychological Mechanism |
|---|---|---|
| Resilience | The most common trajectory (~65%). Characterized by transient perturbations in normal functioning (e.g., several weeks of restless sleep or preoccupation) followed by a rapid, stable return to equilibrium. | Driven by "regulatory flexibility," utilizing a diverse range of coping strategies, self-compassion, and the ability to experience positive emotions alongside sadness. |
| Recovery | Normal functioning temporarily gives way to threshold or subthreshold psychopathology (e.g., depressive symptoms) lasting several months, followed by a gradual return to pre-loss functioning. | Gradual emotional processing and the slow mobilization of external support networks. |
| Chronic Grief | Intense, persistent, and debilitating distress that hinders daily functioning and long-term well-being. Individuals struggle to accept the reality of the loss. | Corresponds directly with Prolonged Grief Disorder. Reflects a failure of emotional regulation and neurobiological adaptation. |
| Delayed Grief | An unexpectedly late grief reaction after a period of seemingly normal functioning. | Bonanno's research demonstrates this is exceedingly rare; long-term empirical evidence has found virtually no solid proof for delayed grief as a common phenomenon. |
Bonanno's model fundamentally repositioned grief research by establishing that resilience is the normative human response, driven by inherent regulatory flexibility rather than pathological denial 111215.
O'Connor's Neurobiological Mapping Model
While Bonanno mapped the behavioral trajectories, Mary-Frances O'Connor provides the mechanistic, neurobiological layer to grief. Her "Gone-But-Also-Everlasting" model shifts the paradigm by defining grieving as an extended form of biological learning 12.
O'Connor's model posits that the brain operates as a prediction engine. To navigate the social world, the brain encodes relationships into a neural "map of safety," tracking attachment figures along the dimensions of psychological closeness, space ("here"), and time ("now") 122. Because humans evolved as a deeply social species, these attachment figures are critical for survival, and the brain permanently encodes the semantic knowledge that the loved one is "everlasting" 12. In intimate relationships, there is a literal neural overlap between the representation of the self and the representation of the other; the circuitry is re-wired to include both members of the dyad as a single functioning unit 2.
When death occurs, a profound neurocognitive conflict arises. The episodic, autobiographical memory of the death event directly contradicts the deeply entrenched semantic neural map that expects the loved one's presence. When the bereaved individual reaches for the phone to call the deceased, they experience a massive "prediction error" 222. Grief, therefore, is the acute physiological and emotional response to this prediction error. Grieving is the slow, effortful process of neuroplasticity required to update the internal neural map so that it accurately reflects the external reality of the person's permanent absence, transitioning from physical presence to internal, continuing presence 1223.
3. The Neurobiology of Grief: Brain Networks and Structures
Advanced functional and structural magnetic resonance imaging (fMRI/sMRI) has provided unprecedented insight into the specific brain regions activated during acute and typical grief. The neurobiology of grief involves a complex, system-wide interplay between networks responsible for reward processing, emotion regulation, memory retrieval, and autonomic control 1617. The intense emotional pain of grief is not a localized phenomenon, but rather an emergent property of multiple interacting neural systems.
The Nucleus Accumbens and Reward Circuitry
A defining feature of acute grief is "yearning" - the intense, physical ache and desire to be reunited with the deceased. Evolutionarily, this drive ensures that separated social mammals seek out and reunite with their kin to maintain group cohesion and survival 118.
Neuroimaging reveals that yearning is mediated heavily by the brain's reward circuitry, specifically the nucleus accumbens, located deep within the ventral striatum 232719. When a deep attachment bond is initially formed, significant neuroplastic changes occur. Specific neuronal ensembles in the nucleus accumbens encode the motivational drive to approach the mate, altering the way proteins are folded within this reward network 12.
In the aftermath of loss, these "craving cells" remain highly active 23. When the bereaved individual is exposed to reminders of the deceased, the nucleus accumbens signals an intense motivational drive, neurologically indistinguishable from the craving for primary biological needs like food or water 118. In typical grief adaptation, this reward pathway gradually recalibrates through neuroplasticity as the brain learns to fulfill attachment needs through continuing internal bonds, conceptualizing the deceased not as physically absent, but internally present 2227.
The Amygdala and Emotion Regulation
The amygdala, a core structure in the limbic system, plays a critical role in threat detection, salience processing, and generating the intense emotional affect characteristic of acute grief 2220. Upon the loss of an attachment figure, the brain's internal "map of safety" is disrupted, stripping the individual of their primary co-regulator. As a result, the amygdala's threat-detection system becomes hyper-reactive 22.
During fMRI tasks designed to elicit grief - such as viewing photographs of the deceased or engaging in the Emotional Counting Stroop (ecStroop) task using grief-related words - the amygdala displays heightened activation, which directly correlates with the intensity of subjective sadness reported by the individual 2030. The effective regulation of this intense affect depends heavily on functional connectivity between the amygdala and prefrontal regulatory regions. In individuals adapting typically to loss, top-down cognitive control is exerted by the dorsolateral prefrontal cortex (DLPFC). High functional connectivity between the DLPFC and the amygdala effectively modulates limbic activity, mitigating attentional bias toward grief-related stimuli and allowing the individual to integrate the loss without being emotionally overwhelmed 2021.
The Cingulate Cortex: Anterior and Posterior
The anterior cingulate cortex (ACC), particularly the rostral (rACC) and subgenual (sACC) subdivisions, is frequently activated during the processing of grief and emotional pain 1617. The ACC is essential for conflict monitoring, emotional regulation, and processing social rejection or separation 3021. In typical grieving, the ACC assists in regulating the distress caused by the "prediction error" of the deceased's absence, helping the brain adjudicate the conflict between semantic memory and current reality. Interestingly, greater activation in the sACC during grief has been positively associated with local systemic inflammation, demonstrating the profound link between neural emotional processing and peripheral immune responses 17.
Furthermore, the posterior cingulate cortex (PCC) is heavily implicated in autobiographical memory retrieval and self-referential processing 1722. Activation in the ventral PCC has been linked to lower baseline parasympathetic activity (measured by respiratory sinus arrhythmia), suggesting a direct anatomical connection between autonomic nervous system regulation and the deep emotional processing of self-relevant memories during bereavement 17.
Neuroplasticity as the Driver of Adaptation
The transition from acute, debilitating grief to integrated adaptation relies entirely on neuroplasticity - the brain's ability to reorganize and form new neural connections in response to experiential feedback. As the bereaved individual confronts the reality of the loss daily (e.g., waking up alone, experiencing a holiday without the deceased), the brain uses this feedback to override outdated neural predictions. This biomechanical process requires the learning of new automatic habits, updating the concept of "self" to include the absence of the deceased, and revising the attachment hierarchy 1223. While low to moderate stress can promote nerve growth and enhance this neuroplastic adaptation, the chronic stress associated with severe, unmitigated grief can actually reduce nerve growth and impair cognitive functions, effectively freezing the brain in an acute state 2334.
4. Recent Insights from fMRI Meta-Analyses (2023 - 2026)
Recent coordinate-based meta-analyses (CBMA) of task-based fMRI studies have advanced the quantitative understanding of how the brain navigates bereavement, yearning, and emotional regulation. By synthesizing data across multiple independent studies utilizing tools like Seed-based d Mapping (SDM), these meta-analyses offer robust statistical evidence of the neural correlates of adaptation 2436.
A central focus of recent literature is how emotional regulation mechanisms operate under acute stress - a reliable proxy for the persistent stress of bereavement. Under stress conditions, individuals rely heavily on cognitive reappraisal to reinterpret a stimulus and reduce its emotional impact 21. Recent meta-analytic neuroimaging reveals that while successful reappraisal typically engages the dorsolateral and ventrolateral prefrontal cortices to dampen limbic responses, acute stress attenuates this prefrontal activation and enhances amygdala reactivity, suggesting a partial disruption of top-down control mechanisms 21. In vulnerable individuals, this decoupling between prefrontal regulatory regions and the amygdala results in impaired emotion regulation, while highly resilient individuals manage to maintain stronger prefrontal-limbic communication even under high stress 2125.
Furthermore, recent meta-analytic data have evaluated emotion-focused interventions aimed at improving functional outcomes in dysregulated populations. These interventions demonstrate a dual-pathway model of neural plasticity. Emotional recalibration is characterized by increased activation in the right caudate (indicating the active engagement of frontostriatal reward and learning circuitry) and decreased activation in the right insula and left inferior frontal gyrus (reflecting a dampening of overly sensitive salience and semantic-control responses) 24. This indicates that as the brain adapts to emotional trauma, it shifts processing power from acute pain and salience detection toward reward-based learning and integration.
When specifically assessing autobiographical memory retrieval - a constant occurrence in grieving - coordinate-based meta-analyses show distinct functional differences. Emotional impairment and mood dysregulation are associated with reduced activity in the salience network, right insula, and fusiform gyrus, coupled with compensatory over-activation in the left anterior cingulate cortex and left middle frontal gyrus 36. This indicates that the grieving or depressed brain struggles to appropriately integrate emotional salience when recalling memories of the deceased, requiring intense cognitive effort to maintain equilibrium. Conversely, during non-autobiographical retrieval, increased right inferior frontal gyrus activity suggests a more vigilant and self-monitoring retrieval mode in dysregulated individuals 36.
5. Prolonged Grief Disorder: Formalization and DSM-5-TR/ICD-11 Criteria
While resilience and integrated adaptation are the most common trajectories, approximately 7% to 10% of bereaved individuals experience a severe complication in the neurobiological learning process 82226. This maladaptive state has been formally recognized as Prolonged Grief Disorder (PGD).
The inclusion of PGD in major diagnostic manuals validates the clinical reality that for a distinct subset of individuals, the normative trajectory of adaptation stalls. This stalling leads to severe functional impairment, physical health deterioration, cognitive decline, and heightened risk of premature mortality and suicidality 67.
Diagnostic Frameworks and Criteria
Both the DSM-5-TR (2022) and the ICD-11 (2018) require specific "gateway symptoms" to establish a PGD diagnosis: a persistent, intense yearning or longing for the deceased, and/or a severe preoccupation with thoughts or memories of the deceased 222627. These symptoms must be accompanied by emotional pain, identity disturbances, and a profound loss of meaning 68.
However, key differences exist between the manuals regarding the timeline and rigidity of the diagnosis:
| Diagnostic Feature | ICD-11 (World Health Organization) | DSM-5-TR (American Psychiatric Association) |
|---|---|---|
| Timeline Criterion | Symptoms must persist for a minimum of 6 months following the death. | Requires that the bereavement occurred at least 12 months prior to diagnosis (6 months for children/adolescents). |
| Symptom Requirement | Simpler clinical guideline; does not specify a rigid minimum number of required associated symptoms, relying more on clinical judgment of impairment. | Stricter criteria; requires the presence of at least three associated symptoms (e.g., identity disruption, avoidance of reminders, intense emotional pain) occurring most days. |
| Cultural Caveat | Symptoms must clearly exceed expected social, cultural, or religious norms. | Symptoms must clearly exceed expected social, cultural, or religious norms. |
Differential Diagnosis
Historically, opponents of the PGD diagnosis argued that it would pathologize normal grief, leading to unnecessary stigma and the over-prescription of psychotropic medications 78. However, robust latent class and network analyses have proven that PGD is a distinct psychopathological entity, separate from Major Depressive Disorder (MDD) and Post-Traumatic Stress Disorder (PTSD), which are highly comorbid with PGD 6.
- PGD vs. MDD: While MDD is characterized by global anhedonia, generalized sadness, and a lack of specific focus, PGD is intensely focused on the specific loss. A patient with PGD may still experience positive emotions in certain contexts but is crippled by yearning for the deceased 1.
- PGD vs. PTSD: While PTSD is rooted in the fear network and trauma processing (perceiving the external environment as fundamentally threatening), PGD is rooted in the reward and attachment networks (perceiving the external environment as fundamentally lacking) 616.
6. Contrasting Typical Neurobiological Adaptation with Prolonged Grief Disorder
The formalization of PGD has catalyzed neuroimaging research to identify the specific biomarkers and neural signatures that differentiate healthy integration from pathological stalling. The evidence reveals profound functional, connectivity, and structural contrasts 1722.
Reward System Dysfunction and Craving
In typical grief, the nucleus accumbens updates its predictions over time, shifting from acute yearning to integrated memory 12. In PGD, this neuroplastic updating fails. Functional MRI studies demonstrate that individuals with PGD exhibit persistent hyperactivation in the nucleus accumbens when exposed to reminders of the deceased 171927. This indicates a profound reward dysfunction - the brain continues to signal a "craving" for the deceased, utilizing neural mechanisms remarkably similar to those observed in addiction disorders 7. The bereaved individual is locked in a neurobiological loop, continually motivated to seek out an attachment figure who cannot be found, which actively interferes with their ability to adapt to the present reality 719.
Because of this specific reward pathway dysfunction, novel pharmacological interventions are being explored that diverge from standard antidepressant protocols. For example, ongoing clinical trials supported by the National Cancer Institute are testing the efficacy of Naltrexone - an opioid antagonist typically used for alcohol use disorder - to treat PGD. The therapeutic rationale is to chemically dampen the reward pathway, diminishing the overwhelming feelings of yearning and social bonding craving, thereby creating the cognitive space necessary for psychotherapeutic learning to take place 7.
Functional Connectivity and Emotion Regulation
In normal adaptation, the prefrontal cortex successfully establishes functional connectivity with the amygdala to regulate emotional pain 20. In PGD, this regulatory network breaks down. Resting-state fMRI identifies significant hyperconnectivity within the limbic system (between the right amygdala and the thalamus) and a failure of prefrontal down-regulation 17. When executing tasks that require cognitive control (such as the ecStroop task using grief-related words), individuals with PGD show a notable absence of the necessary rostral ACC and fronto-cortical recruitment seen in non-complicated grievers 30. Consequently, they are unable to disengage from idiographic loss-relevant stimuli, leading to rumination and persistent emotional flooding 30.
Structural Brain Changes and Neurotoxicity
Chronically elevated stress levels in PGD exert toxic effects on brain architecture. Structural MRI studies have revealed significant volume reductions and atrophy in the hippocampus (particularly the left hemisphere) and the amygdala among bereaved populations suffering from prolonged grief 161728. For example, studies of "Shidu" parents in China - parents who have lost their only child - demonstrate reduced right amygdala grey matter volume and stronger amygdala-to-whole-brain structural connectivity associated with intense prolonged grief 20. Additionally, atrophy in the supramarginal gyrus has been shown to mediate the association between intense grief and impaired cognitive inhibition 17. Prolonged grief is also associated with white matter abnormalities, increasing the long-term risk for cognitive decline and neurodegenerative diseases 1617.
| Neurobiological Metric | Typical/Integrated Grief | Prolonged Grief Disorder (PGD) |
|---|---|---|
| Nucleus Accumbens (NAcc) | Adaptive recalibration; decreased reward-craving upon reminders. | Persistent hyperactivation; reward-dysfunction similar to addiction craving. |
| Prefrontal-Amygdala Coupling | Strong functional connectivity; efficient top-down emotion regulation. | Reduced connectivity; failure of prefrontal cortex to dampen limbic distress. |
| Brain Structure (Hippocampus & Amygdala) | Volume generally maintained post-acute stress phase. | Significant volume reductions/atrophy due to chronic stress neurotoxicity. |
| Anterior Cingulate Cortex (ACC) | High recruitment during emotional tasks to resolve conflict. | Blunted or absent recruitment during grief-specific emotional regulation tasks. |
7. Cross-Cultural Frameworks and the Processing of Grief
Grief is a biological imperative, yet its expression, cognitive processing, and resolution are profoundly shaped by sociocultural context. Western psychiatric models have historically emphasized individualism and the psychological process of "letting go" to achieve closure. However, cross-cultural studies highlight that communal mourning, meaning-making, and ongoing bonds dictate entirely different, yet highly adaptive, resilience trajectories 124129.
Cultural Influences on Cognitive Processing and Coping
In societies with interdependent social structures, such as India, grief is intrinsically interwoven with joint family systems, religious diversity, and community rituals 41. These cultural frameworks provide a robust psychological buffer, embedding the bereaved within a highly regulated social field. The cognitive processing of grief in these contexts often focuses less on individual "moving on" and more on fulfilling duties to the deceased and maintaining spiritual continuity 1241. Similarly, traditional mourning rituals in African and East Asian contexts foster communal support that directly mitigates post-loss psychopathology by distributing the emotional burden across the community 4130.
Idioms of Distress and Symptom Presentation
Cultural frameworks also dictate how grief manifests symptomatically. In many non-Western contexts, grief is expressed through culturally specific "idioms of distress." For example, a cross-cultural study demonstrated that feelings of loss and difficulty moving on were central symptoms in samples from Ghana and Nigeria, while Western core symptoms like preoccupation and longing were less prevalent 30. Furthermore, bereaved Cambodian refugees frequently report hallucinating and dreaming of the deceased, which holds significant cultural meaning rather than indicating psychotic pathology 30. In India, grief often presents through somatic complaints and spiritual distress, which may elude formal diagnosis if clinicians rely solely on Western criteria frameworks 41.
When vital cultural rituals are disrupted - as witnessed globally during the COVID-19 pandemic - the lack of structural support dramatically amplifies the severity of grief. The inability to engage in traditional mourning practices was associated with heightened risks for spiritual concerns, distressing somatic symptoms, and a global spike in complicated grief 4130. Recent longitudinal methodologies, such as Experience Sampling Methods (ESM) deployed via mobile applications across Switzerland, Viet Nam, and Rwanda, are currently mapping how these collective beliefs uniquely shape the real-time dynamics, symptom variability, and chronicity of PGD across diverse populations 30.
8. Biological Resilience Trajectories and the Physiological Toll of Loss
The social and cultural environment directly modulates the biology of the bereaved. "Biological resilience" refers to the body's ability to withstand and adapt to the severe allostatic load - the cumulative physiological wear and tear - imposed by the stress of bereavement 3145. Grief extends its effects across multiple organismic systems, profoundly impacting neuroendocrine and immunological function 16.
Inflammatory Markers and Immune Dysregulation
Bereavement is consistently associated with heightened systemic inflammation. Studies evaluating spousally bereaved individuals demonstrate significant elevations in pro-inflammatory cytokines, specifically Interleukin-6 (IL-6), soluble E-selectin, Interferon-gamma (IFN-γ), and Tumor Necrosis Factor-alpha (TNF-α) 34323334. This inflammatory cascade is a direct biological response to the stress of social disconnection, as the body reacts to the loss of a primary co-regulator as if it were a physical wound 34.
Resilient individuals, who leverage strong social support and cultural integration, exhibit significantly lower levels of these inflammatory biomarkers, maintaining immune homeostasis and thereby reducing their risk for subsequent cardiovascular disease, cancer, and metabolic disorders 349. Conversely, individuals suffering from high grief severity and PGD show a persistent inflammatory state, creating a negative bio-social loop wherein systemic inflammation crosses the blood-brain barrier to further exacerbate psychosocial distress and depressive symptoms 3435.
Cortisol and HPA Axis Dysregulation
The trauma of loss heavily activates the hypothalamic-pituitary-adrenal (HPA) axis. While an acute spike in the stress hormone cortisol is a normative biological reaction designed to mobilize energy, chronic grief is characterized by profound HPA-axis dysregulation. Bereaved individuals, particularly those exhibiting PGD, frequently demonstrate flattened diurnal cortisol slopes and altered morning cortisol responses (the cortisol awakening response, or CAR), indicating that the biological stress response has lost its flexibility and remains locked in a maladaptive state 333436.
Heart Rate Variability and Autonomic Flexibility
Vagally mediated Heart Rate Variability (HRV) has emerged as a premier biomarker for both psychological and biological resilience. HRV measures the flexibility of the autonomic nervous system and its ability to rapidly switch between sympathetic arousal and parasympathetic recovery. Research highlights that bereaved individuals with higher baseline HRV demonstrate enhanced cognitive resilience, superior emotional regulation, and a much faster recovery from grief symptoms over time, even among those with compounding vulnerabilities such as a history of childhood maltreatment 373854. High HRV indicates robust "inflammatory resilience" and the biological capacity to return to baseline rapidly following a stressor 3854.
Epigenetic Aging and Bio-Social Looping
The immense allostatic load of bereavement can actually accelerate biological aging at the cellular level. Research into "GrimAge" - a DNA methylation-based biomarker of lifespan - demonstrates that cumulative stress is associated with accelerated epigenetic aging, driven by increased insulin resistance and adrenal sensitivity 5. However, psychological resilience factors, such as high emotion regulation and self-control, actively moderate this relationship, blunting the epigenetic impact of stress 5.
Ultimately, these biological markers do not operate in a vacuum. A phenomenon known as "bio-social looping" demonstrates that the nervous system of the individual and the social field of the community are deeply intertwined 45. Culturally resonant practices, communal support, and meaningful rituals directly down-regulate the sympathetic nervous system, buffer cortisol responses, and suppress inflammatory gene expression, actively forging the biological pathway toward resilience and integrated adaptation 455439.
Conclusion
The science of grief has transcended the simplistic, sequential stages of the past, evolving into a rigorous, multidimensional discipline anchored in neuroscience, psychoneuroimmunology, and cross-cultural psychiatry. Bereavement forces the brain into a profound state of cognitive dissonance and prediction error, necessitating an arduous, energy-intensive process of neuroplasticity to redraw internal maps of attachment and safety. While empirical research confirms that resilience is the inherent and dominant human response to loss, the formal recognition of Prolonged Grief Disorder highlights the devastating psychological and physiological consequences when this neurobiological learning process stalls.
Recent neuroimaging and biomarker data provide unprecedented clarity: the transition from acute grief to integrated adaptation requires functional frontostriatal circuitry, flexible top-down prefrontal control, and a resilient autonomic nervous system capable of mitigating systemic inflammation. When treating PGD, clinical interventions must move beyond standard depression protocols to specifically target the persistent reward-craving dysregulation within the nucleus accumbens. Furthermore, recognizing that biological resilience is inexorably linked to cultural frameworks and social integration ensures that future therapeutic models will be holistically designed to treat the bereaved mind, body, and community.