How to Support a Grieving Friend According to Psychology
The provision of support to a grieving individual represents a complex psychological and sociological endeavor. For decades, the societal and clinical understanding of grief was heavily shaped by linear, prescriptive models that fundamentally failed to capture the idiosyncratic, oscillating nature of human bereavement. Current psychological research, however, reveals that effective grief support requires abandoning outdated paradigms, such as the expectation of "closure," and adopting frameworks grounded in emotional validation, proactive instrumental assistance, and profound cultural attunement 123.
To effectively support a grieving friend or community member, empirical evidence dictates a tripartite approach. First, the supporter must provide proactive, concrete instrumental aid rather than reactive, vague offers of help, recognizing that the executive functioning and working memory of the bereaved are often temporarily impaired by the trauma of loss 25. Second, the supporter must offer non-judgmental emotional presence, creating a secure psychological space for the bereaved to oscillate between confronting the loss and finding necessary respite from it 167. Third, the supporter must rigidly apply the principle of "Comfort In, Dump Out," ensuring that their own secondary emotional distress is processed entirely away from the primary mourner 39. This comprehensive report provides an exhaustive, evidence-based explainer on the psychological mechanisms of grief, the critical integration of culturally diverse mourning practices, the profound impact of the post-pandemic digital age, and concrete, peer-reviewed strategies for offering effective support.
FAQ: Why is the "Five Stages of Grief" Model Considered Outdated and Harmful?
The "Five Stages of Grief" - denial, anger, bargaining, depression, and acceptance (frequently referred to by the acronym DABDA) - is arguably the most pervasive psychological concept regarding bereavement in global popular culture. Formulated by the Swiss psychiatrist Elisabeth Kübler-Ross in her 1969 publication On Death and Dying, the model was originally developed to describe the emotional trajectory of terminally ill patients coming to terms with their own impending mortality, not the experiences of those left behind to mourn 4512.
Despite its widespread societal adoption, decades of rigorous empirical research have debunked the five-stage model as an accurate descriptor of human bereavement 56. The model lacks systematic empirical evidence for a sequential progression of stages in grieving individuals 614. Bereavement researchers and institutions, including the American Psychological Association (APA), caution heavily against its prescriptive use, noting that grief simply does not unfold in a lock-step, linear fashion with concrete boundaries 4614. The assumption that individuals must pass through a specific sequence of emotional milestones to achieve resolution is fundamentally flawed 6.
The continued application of this paradigm to bereaved individuals actively causes psychological harm 5. When society, and sometimes even misinformed clinical practitioners, expect grief to conform to neat, predictable stages culminating in a finalized state of "acceptance," it establishes a normative baseline that contradicts the inherently chaotic reality of mourning 456. Bereaved individuals who do not experience the stages in order, who skip stages entirely, or who experience fluctuating, intense emotions years after a loss often engage in severe self-criticism. They may worry they are "doing grief wrong," failing to adjust properly, or suffering from a psychological defect or complicated grief disorder 45.
Furthermore, the expectation of "acceptance" as a final destination pathologizes the enduring nature of grief. It fails to recognize that healthy psychological adaptation involves integrating the loss and continuing a bond with the deceased, rather than achieving total emotional detachment or societal "closure" 3515. Instead of a stage-based progression, modern psychological literature indicates that the majority of individuals exhibit profound resilience following a loss, while experiencing complex, oscillating emotional reactions that gradually soften over time but never entirely disappear 478.
FAQ: What is the Dual Process Model of Coping with Bereavement?
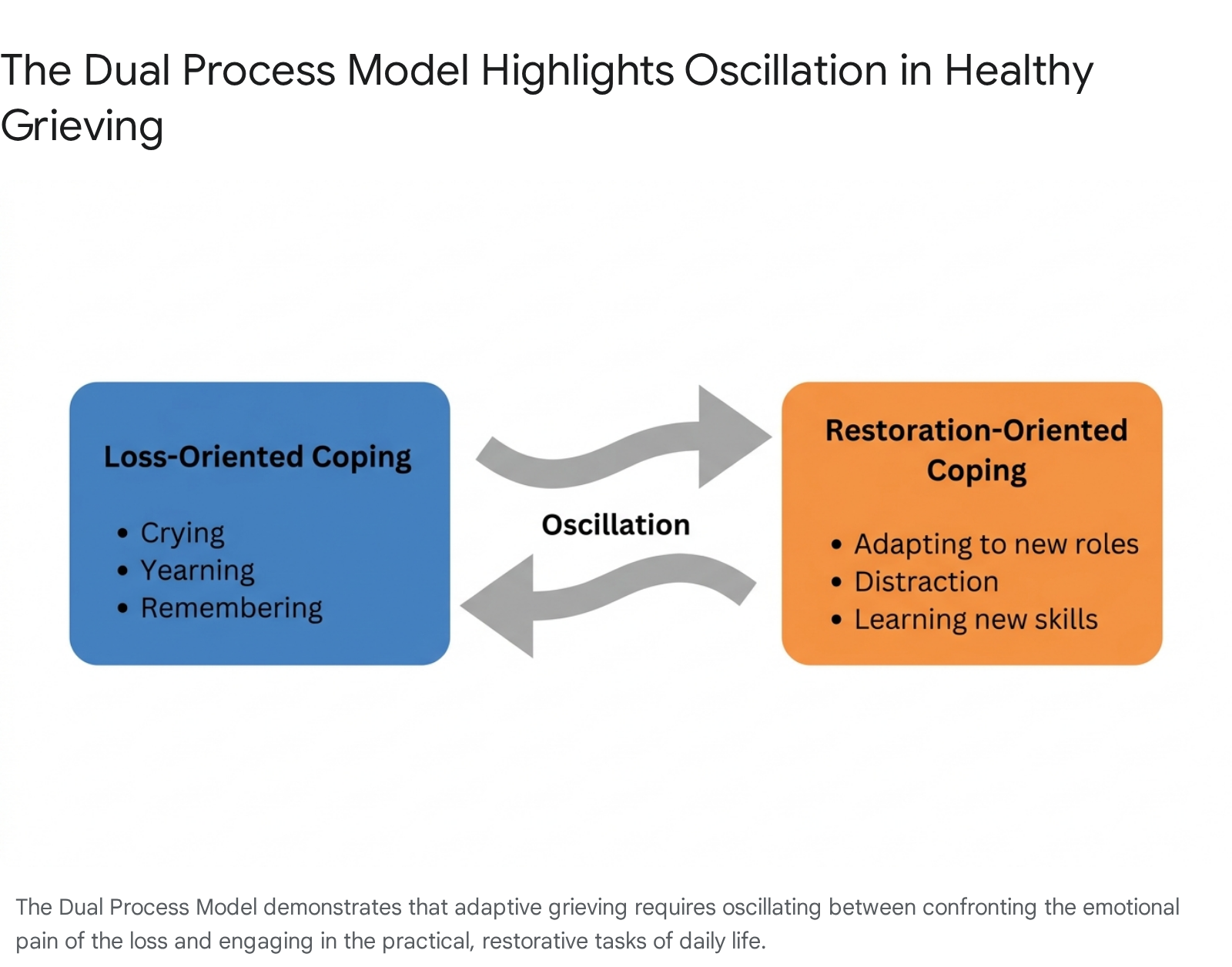
Developed by researchers Margaret Stroebe and Henk Schut in 1999 and subsequently expanded upon in journals such as Death Studies, the Dual Process Model of Coping with Bereavement (DPM) is currently recognized as one of the most robust, evidence-based frameworks for understanding how individuals adapt to loss 367. Unlike earlier "grief work" theories derived from Freudian models that demanded constant confrontation with the pain of loss, the DPM acknowledges that adaptive grieving requires both active confrontation and necessary avoidance 718.
The model categorizes coping mechanisms into two interconnected spheres of action: The first sphere is Loss-Oriented Coping. This involves directly confronting the reality of the death and processing grief-related emotions. Activities within this domain include crying, yearning, looking at photographs, visiting a gravesite, talking about memories, and sitting with the pain of absence. It is the emotional "grief work" traditionally associated with mourning 361819. The second sphere is Restoration-Oriented Coping. This focuses on adapting to the secondary stressors and practical life changes that follow a death. It includes mastering new skills (e.g., managing finances previously handled by the deceased), forming new social connections, engaging in routine household chores, or finding healthy distractions such as returning to work or consuming entertainment 361819.
The central tenet of the DPM is oscillation 671820. Healthy adaptation involves a dynamic, ongoing back-and-forth movement between these two processes. A bereaved individual may spend the morning immersed in profound sorrow (loss-oriented) and the afternoon focused entirely on organizing a closet or socializing (restoration-oriented) 3620.
For those seeking to support a grieving friend, the DPM offers profound practical guidance. It normalizes the inconsistencies of grief, significantly reducing the external judgment applied to a mourner's behavior. If a bereaved individual is laughing at a television show weeks after a profound loss, they are not exhibiting "denial"; they are engaging in vital, healthy restoration-oriented coping 3. Conversely, if they are incapacitated by sorrow six months later, they are not "stuck" or regressing, but merely oscillating back to a loss-oriented state 3. Supporters must proactively create an environment that accommodates both states without pressuring the individual to remain exclusively in one psychological lane 320.
FAQ: How Does "Ring Theory" Dictate Appropriate Behavior Around the Bereaved?
When a traumatic loss occurs, individuals on the periphery of the event often experience their own secondary grief, shock, or anxiety. A common and highly damaging failure in providing support occurs when these peripheral individuals offload their own distress onto those closer to the tragedy. To address this phenomenon, clinical psychologist Susan Silk and mediator Barry Goldman developed "Ring Theory" (often referred to as the "Circle of Support") in 2013, which provides a definitive behavioral framework for navigating emotional communication during crises 399.
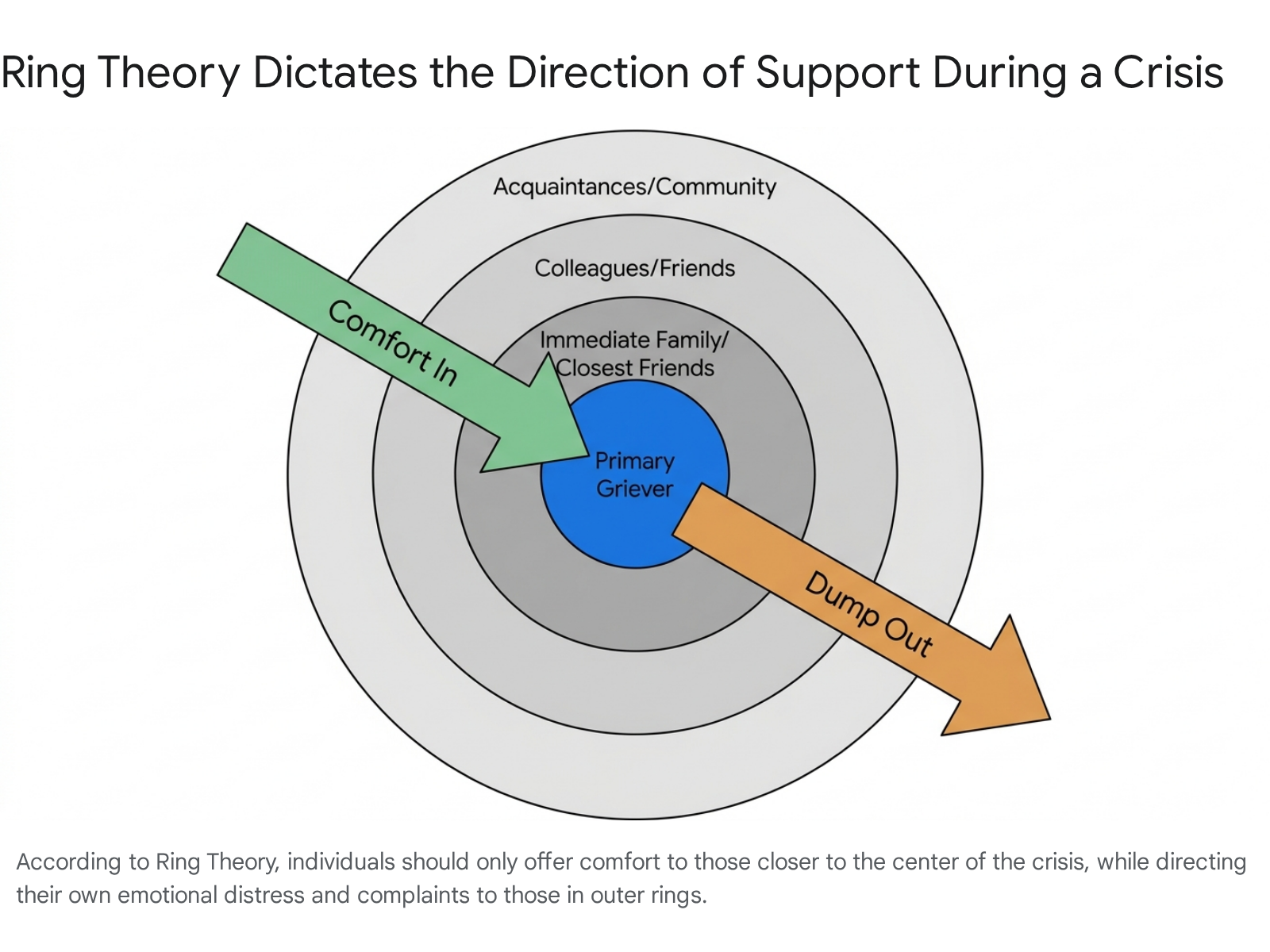
Ring Theory operates on a visual model of concentric circles representing varying levels of intimacy with the crisis. At the absolute center is the primary griever - the person most directly affected by the loss, such as the parent of a deceased child or the widowed spouse 3922. The next ring outward contains their most intimate relations, typically immediate family and best friends. Successive outward rings contain colleagues, casual friends, acquaintances, and finally, bystanders and professionals on the outermost edge 99.
The core directive of the theory is summarized in four operational words: "Comfort In, Dump Out" 3923. An individual may only offer comfort, practical assistance, and empathetic listening to those in rings smaller (closer to the center) than their own 922. Conversely, if an individual needs to express shock, complain about the unfairness of the situation, cry, or seek emotional validation for their own distress, they may only do so to individuals in rings larger (further from the center) than their own 9923.
This framework actively prevents the well-meaning but incredibly harmful phenomenon of "centering." For instance, a colleague visiting a grieving mother should not discuss how devastated they personally are by the news, nor should they offer unsolicited advice or complain about their own unrelated struggles to relate to the situation 23. The primary griever is granted absolute permission to express raw, messy emotions without needing to artificially manage the feelings of their visitors 910. Ring Theory is not only applicable to personal bereavement but has been successfully adapted for processing collective trauma and providing social justice support to marginalized groups targeted by systemic violence 99.
FAQ: What is the Difference Between Proactive Instrumental and Emotional Support?
Social support in the context of bereavement is generally bifurcated into two primary psychological categories: emotional support and instrumental support. Emotional support involves the provision of empathy, active listening, validation, and a non-judgmental presence 11122728. Instrumental support refers to actionable, tangible aid that assists with specific tasks, such as delivering meals, providing transportation, managing complex financial paperwork, or completing routine household chores 1111314.
Research consistently demonstrates that bereaved individuals identify emotional support as the most deeply desired form of assistance following a loss 11315. However, the efficacy of instrumental support is highly dependent on the mechanism of its delivery. Specifically, the ubiquitous phrase "Let me know if you need anything" is categorized in psychological literature as a passive, reactive offer that frequently backfires and causes harm 127.
The cognitive impact of grief involves significant alterations in the brain's executive functioning, working memory, and attention span, which neurological studies indicate can persist for 6 to 24 months 5. Consequently, placing the cognitive burden on the bereaved to identify a need, formulate a request, and delegate a task to a friend is often overwhelming and isolating. Proactive instrumental support - where the supporter independently identifies a specific need and executes it without requiring the griever's active management (e.g., "I am bringing dinner on Tuesday," or "I will research three funeral home options and send you a summary") - is substantially more effective 252732.
Longitudinal studies underscore the vital, life-saving role of these support types over extended periods. Data analyzing bereaved older adults in Taiwan demonstrated that consistently high levels of perceived instrumental support were associated with significantly lower mortality risks, particularly for those mourning the catastrophic loss of a child 16. Interestingly, organizational psychology meta-analyses indicate that the benefits of instrumental support are deeply intertwined with emotional engagement; instrumental aid primarily enhances well-being and reduces feelings of loneliness when the provider is also perceived as emotionally attuned and genuinely engaged 1217. Delivering a casserole is functionally helpful, but delivering it with a willingness to sit in quiet solidarity amplifies the psychological benefit exponentially.
Furthermore, peer support networks operate through specific micro-processes that bridge both emotional and instrumental domains. A 2024 qualitative study detailed in Death Studies highlighted the distinct therapeutic elements present in suicide bereavement peer support groups, emphasizing that authentic healing occurs when supporters engage in active, compassionate witnessing without normative scripts.
| Micro-Process of Peer Support | Psychological Function for the Bereaved | Clinical Outcome |
|---|---|---|
| Bearing Compassionate Witness | Providing unconditional listening and non-judgment through voice tone and silence. | Brings the reality of the grief into focus, making the pain feel more bearable 10. |
| Revealing the Unspoken | Creating a secure space to share guilt-induced self-questioning and internalized shame. | Reframes the rumination cycles of "shoulds" and "coulds" that follow traumatic loss 10. |
| Extending the Bond | Moving support beyond formal interactions into spontaneous acts of care (e.g., anniversary check-ins). | Reduces isolation and specific stigmas associated with causes of death like suicide 10. |
| Normalization without Scripts | Allowing mourners to realize that feelings of "going crazy" are standard trauma responses, without enforcing a "roadmap." | Increases flexibility and autonomy, allowing the story to unfold at the griever's pace 10. |
FAQ: How Do Cultural Differences (Non-WEIRD Perspectives) Shape Grief Expectations?
A significant and historically damaging limitation in psychological research is its over-reliance on WEIRD (Western, Educated, Industrialized, Rich, and Democratic) populations. Western clinical frameworks typically emphasize individual autonomy, stoicism, and a psychological drive toward emotional "closure," pathologizing those who do not quickly return to baseline productivity 353637. In contrast, non-WEIRD cultures frequently conceptualize grief as a profoundly communal, interdependent process rooted in elaborate rituals, physical catharsis, and ongoing spiritual connections 35363738. Applying Western clinical paradigms to collectivistic cultures frequently results in the erroneous pathologization of highly adaptive, normative grief responses 3718.
To understand the global tapestry of bereavement, psychological research from 2024 and 2025 has increasingly focused on the efficacy of specific cultural rituals across different continents.
| Cultural Context | Key Mourning Rituals & Practices | Psychological and Communal Function |
|---|---|---|
| Sub-Saharan Africa (Luhya People, Kenya) | Ritual beating of corpses in cases of suicide, retaliation rituals for murder, and physical fertility rituals for childless deceased 19. | Facilitates profound emotional catharsis by externalizing anger and frustration. Participants report deeper closure and emotional relief compared to standard clinical therapy 19. |
| East & Southeast Asia | Maintaining family altars, burning symbolic offerings (belongings of the deceased), intensive mourning for 100 days, and three-year mourning periods for parents 241. | Manifests filial piety and fosters "continuing bonds." Transforms the bereaved into a "memory-keeper," providing a structured framework for emotional resilience rather than attempting closure 414220. |
| Latin America | Emphasis on familismo, communal gatherings, and extended spiritual prayer cycles such as the novena 2122. | Buffers against prolonged grief through high social cohesion. However, disruption of these rituals due to immigration or acculturation severely spikes the risk of complicated grief 2122. |
Research spanning six Latin American countries in 2025 assessed Posttraumatic Growth (PTG) following a loss, revealing that the relationship between grief intensity and positive psychological growth is significantly moderated by age and gender 2324. For example, gender was a primary moderator for PTG in Peru and El Salvador, whereas age drove outcomes in Uruguay, indicating that broad, generalized interventions are ineffective unless they are highly tailored to the specific demographic and cultural realities of the mourner 23.
In East Asian contexts, the integration of mindfulness and death contemplation practices - often rooted in Buddhist philosophy - has been shown to reduce existential distress and lower rates of clinical depression 2549. Cultivating a positive, equanimous attitude toward death, rather than fear, promotes resilience, particularly in older adults who face frequent bereavement 25. Furthermore, a theoretical model termed the 'Four-Dimensional Framework for Understanding Cultural Grief Rituals' suggests that these diverse practices share core psychological functions: they provide emotional structure, foster cross-cultural empathy, reinforce communal cohesion, and impart spiritual wisdom, all of which act as protective factors against the development of grief disorders 2627.
FAQ: How Did the COVID-19 Pandemic Alter the Landscape of Grief?
The COVID-19 pandemic constituted a mass bereavement event of unprecedented scale that fundamentally disrupted global mourning practices and permanently altered the trajectory of grief for millions 282954. Epidemiological data suggests that for every COVID-19 death, approximately nine family members experienced acute emotional distress, creating a vast network of secondary trauma 55.
The pandemic introduced unique contextual variables that violently interfered with the natural grieving process. Social distancing measures meant that individuals frequently died in isolation, depriving families of the opportunity to engage in end-of-life care or say goodbye 2830. The suspension of communal mourning rituals, funerals, and in-person social support removed the traditional psychological scaffolding that societies have relied upon for millennia to process loss 112831. Research published in Death Studies indicates that virtual farewells via video or telephone, while practically necessary, were associated with significantly higher levels of acute suffering, regret, and enduring guilt 3058.
Consequently, the prevalence of Prolonged Grief Disorder (PGD) - a severe psychiatric condition characterized by intense, disabling yearning and identity disruption extending beyond societal norms - spiked globally. Meta-analyses of pandemic-era bereavement estimated pooled prevalence rates of grief disorders reaching an alarming 46% among affected populations 31. Post-pandemic clinical tracking revealed that emotional loneliness - defined as the distressing absence of intimacy and emotional connection, which cannot be cured merely by being around other people - was a primary predictor of severe, persistent grief symptoms, significantly outpacing general social isolation as a risk factor 59.
Despite these heightened vulnerabilities, formal help-seeking remained distressingly low. However, psychiatric evaluations indicated that help-seeking was one of the few coping strategies that significantly buffered the impact of severe grief on the overall quality of life for individuals exhibiting high grief severity 60. This period highlighted an urgent public health need to refine the definitions of grief disorders and to scale accessible, evidence-based bereavement support 32.
FAQ: How Is Digital Technology and Social Media Changing Grief Support (2023+)?
The transition of grief expression from the private sphere to highly public digital domains has introduced profound psychological complexities into modern bereavement 626364. Digital platforms act as a double-edged sword, functioning simultaneously as vital facilitators of peer support and as environments fraught with distinct psychological risks 6566.
A massive 2025 scoping review of digital grief, mapping literature from 2010 to 2025, identified five core themes driving online bereavement: acting as a cry for help, maintaining continuing bonds with the deceased, establishing digital memorialization and rituals, developing a sense of community, and functioning as a tool for emotional expression 64.
Digital technologies have democratized access to grief support, proving highly feasible and acceptable for those experiencing physical or social isolation 31. Online support groups provide immediacy, anonymity, and asynchronous connection, allowing grievers to engage at their exact pace 546533. This is particularly critical for survivors of stigmatized or sudden losses, such as suicide, where traditional family networks may be paralyzed by shame or a lack of understanding 103435. Peer-to-peer digital networks allow individuals to bypass societal taboos and normalize their traumatic reactions by reading about others' experiences 10316236.
Conversely, the rapidly evolving "cyberthanatology" landscape presents unique psychiatric hazards. The hyper-public nature of social media can pressure individuals into performative expressions of grief, actively exacerbating distress and rumination. A 2026 systematic review focusing on Generations Z and Alpha revealed that public memorial posts often lead to alienation when intimate grief is commodified or perceived by peers as inauthentic 66. The phenomenon of "grief hypejacking" - where influencers or peripheral acquaintances use a tragedy to center their own narrative or farm engagement - is a rising source of trauma for primary mourners 3637.
Furthermore, algorithmic architecture poses a persistent threat to emotional regulation. Platforms that automatically surface "memories" (e.g., Facebook's "On This Day") or algorithmically push unsolicited grief content based on user engagement metrics can ambush the bereaved with traumatic reminders 636533. This forces the bereaved to confront intense loss-oriented stressors precisely at moments when they may lack the cognitive bandwidth to process them, completely subverting the healthy oscillation described in the Dual Process Model 636533. The integration of Artificial Intelligence adds another layer of ethical concern; the creation of "Dadbots" or AI avatars trained on the digital footprint of the deceased risks commodifying grief and hindering the natural mourning process by fostering unnatural psychological dependencies 18.
The digitization of mourning necessitates a strict, modernized code of funeral etiquette that prioritizes the emotional safety of the primary mourners over the immediate broadcasting of information 377273.
| Digital Etiquette Principle | Psychological Rationale for Compliance |
|---|---|
| Do not pre-empt the primary family. | Never post an obituary or a "RIP" status before the primary mourners have publicly shared the news. Usurping this right strips the family of control during a highly vulnerable period 3772. |
| Respect digital legacies and consent. | Do not tag the deceased in photos or attempt to alter their social media profiles unless acting as a legally designated legacy contact with prior consent 37. |
| Maintain strict physical-digital boundaries. | Avoid posting selfies at funerals, "checking in" to funeral homes, or livestreaming services without explicit, prior permission from the family, as this violates the sanctity of the mourning space 3772. |
| Avoid performative "Hypejacking". | Do not use a tragedy to center your own narrative, advance advocacy efforts prematurely, or farm engagement via hashtags if you are on the outer rings of the crisis 3637. |
FAQ: What Are the Most Effective Ways to Communicate with a Grieving Friend?
Micro-sociological analyses of social support reveal that the specific language and phrasing used by supporters can profoundly impact a grieving individual's trajectory, either fostering resilience or compounding trauma 38. The most helpful interactions are those that provide "compassionate witness" - where the supporter holds space for the reality of the pain without attempting to "fix" it, rush it, or apply societal scripts regarding how the bereaved should behave 110.
Conversely, the most frequently cited "unhelpful" memorable messages in psychological studies are those that attempt to rationalize the death, exude toxic positivity, or minimize the loss 13839. These phrases often backfire precisely because they arise from the supporter's own psychological discomfort with witnessing pain; in attempting to force a silver lining, the supporter inadvertently disenfranchises the mourner's grief, making them feel profoundly isolated and misunderstood 13839.
A critical psychological competency for supporters is maintaining "calibrated uncertainty" 76777879. When faced with traumatic loss, human psychology has a powerful, intrinsic drive to resolve uncertainty by imposing neat narratives or theological explanations (e.g., "It was God's plan"). However, effective clinical support requires resisting this urge entirely. Supporters must accept the ambiguity of the situation, allowing the griever to dictate their own meaning-making process over time, rather than selling them false confidence or forced conclusions 7779.
The table below contrasts common, culturally pervasive phrases that empirical research identifies as unhelpful with evidence-based alternative approaches that foster genuine psychological support.
| Category of Support | Common Unhelpful Phrases (To Avoid) | Evidence-Based Alternatives (To Use) | Psychological Rationale |
|---|---|---|---|
| Passive Offers | "Let me know if you need anything." / "Call me if you need to talk." 1272832 | "I am bringing dinner over on Tuesday." / "I will come by to mow the lawn tomorrow." 32732 | Passive offers place the cognitive burden of project management onto the griever, whose executive functioning is impaired 527. Proactive, specific instrumental support relieves this burden. |
| Rationalization / Toxic Positivity | "Everything happens for a reason." / "They are in a better place now." / "God doesn't make mistakes." 2838 | "I am so sorry for your loss." / "I cannot imagine how hard this must be." / "I am here for you." 28 | Rationalizing death minimizes the griever's current pain. It attempts to bypass the necessary loss-oriented coping and can disenfranchise the mourner's valid feelings of anger or despair 283839. |
| Enforced Timelines | "You need to be strong." / "It's time to move on." / "You will get over it." 12728 | "Take all the time you need." / "There is no timeline for this." / "Your feelings make sense." 127 | Grief is not a linear process to be "completed." Enforcing timelines creates anxiety and self-judgement, making the bereaved feel defective for experiencing normal oscillation 135. |
| Avoidance / Erasure | Changing the subject when the deceased is mentioned. / Avoiding saying the deceased's name. 128 | "I was thinking about [Deceased's Name] today. I remember when they..." / "Tell me a story about them." 12728 | Avoidance isolates the griever, confirming their fear that their pain is a burden. Saying the deceased's name honors their continuing bond and provides profound emotional validation 11528. |
| Comparative Minimization | "I know exactly how you feel; my dog died last year." / "At least you had them for 20 years." 2728 | "This must be incredibly painful." / Listening silently without offering a comparative anecdote. 102728 | Centering one's own experiences invalidates the unique nature of the mourner's specific relationship and loss. It violates the "Comfort In, Dump Out" principle of Ring Theory 9927. |
Bottom Line
The psychological and sociological science of bereavement unequivocally demonstrates that grief is not a pathology to be cured, nor a linear set of sequential stages to be completed and filed away. It is a lifelong, highly dynamic process of adaptation characterized by a healthy oscillation between confronting profound sorrow and engaging in the restorative, practical tasks of rebuilding a life 367.
For those seeking to effectively support a grieving friend, the evidence demands a radical shift from reactive, platitude-driven responses to proactive, structurally sound care. Supporters must abandon the innate human desire to "fix" the unfixable and instead embrace the discipline of "calibrated uncertainty," bearing compassionate witness to the pain without imposing enforced timelines or toxic positivity 11077. Utilizing established frameworks like Ring Theory ensures that emotional burdens flow outward, protecting the primary mourner from the secondary distress of their community 9. Furthermore, integrating a nuanced understanding of culturally specific rituals - recognizing that communal mourning, ancestral reverence, physical catharsis, and digital memorialization are vital tools for maintaining continuing bonds - ensures that support is not only well-intentioned but profoundly effective and resonant across diverse populations 2202765. Ultimately, the most powerful psychological support one can offer is an unwavering, non-judgmental presence, coupled meticulously with specific, tangible actions that ease the logistical burdens of navigating a permanently changed world.