Determining the need for trauma therapy versus depression therapy
Diagnostic and Nosological Frameworks
The clinical presentation of severe psychological distress frequently involves profound sadness, lethargy, cognitive impairment, and a loss of interest in daily activities. While these symptoms typically lead to a diagnosis of Major Depressive Disorder (MDD), a critical diagnostic distinction exists between standard biogenic or endogenous depression and trauma-induced reactive depression 1. Recognizing this distinction is vital for determining whether an individual requires standard therapeutic interventions for depression or highly specialized trauma processing therapy.
Standard MDD is traditionally characterized by persistent low mood and anhedonia, often treated through a combination of standard cognitive therapies and pharmacotherapy, such as selective serotonin reuptake inhibitors (SSRIs) 12. In contrast, trauma-induced depression arises as a secondary consequence of acute, prolonged, or developmental trauma 13. Individuals with a history of trauma, particularly childhood maltreatment or complex interpersonal trauma, exhibit significantly higher rates of treatment-resistant depression when provided with standard SSRI protocols or traditional talk therapies alone, demonstrating a response profile that more closely aligns with post-traumatic stress disorder (PTSD) than unipolar depression 1.
The complexity of distinguishing between these conditions is compounded by how trauma-related disorders are classified in major diagnostic manuals. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) conceptualizes PTSD broadly, requiring symptoms across intrusion, avoidance, negative alterations in cognition and mood, and alterations in arousal and reactivity 4. Under the DSM-5-TR framework, trauma-induced depressive symptoms are often categorized under the "negative alterations in cognition and mood" cluster or diagnosed sequentially as comorbid MDD 14. Consequently, the DSM-5-TR criteria consistently yield substantially higher baseline PTSD rates compared to alternative diagnostic frameworks 56.
Conversely, the International Classification of Diseases, Eleventh Revision (ICD-11), separates standard PTSD from Complex PTSD (CPTSD). The ICD-11 aims to delineate a distinct PTSD phenotype by removing broad mood and anxiety diagnostic criteria 7. A diagnosis of ICD-11 CPTSD requires the core symptoms of PTSD - re-experiencing in the present, avoidance, and a persistent sense of threat - alongside a secondary cluster known as Disturbances in Self-Organization (DSO) 48. The DSO cluster captures the profound personality and affective changes often mistaken for standard depression.
| Diagnostic Feature | DSM-5-TR PTSD | ICD-11 Complex PTSD (CPTSD) |
|---|---|---|
| Diagnostic Structure | Single broad diagnosis capturing high heterogeneity. Does not distinguish complex trauma 4. | Sibling diagnoses (PTSD and CPTSD) distinguishing between acute trauma and complex trauma 49. |
| Trauma Definition | Restricted to exposure to actual or threatened death, serious injury, or sexual violence 48. | Broader and more inclusive; events must be "extremely threatening or horrific" but impact defines the diagnosis 48. |
| Core Symptom Clusters | Intrusion, avoidance, negative alterations in cognition and mood, alterations in arousal and reactivity 46. | Re-experiencing, avoidance, sense of threat, plus Disturbances in Self-Organization (DSO) 4810. |
| Self-Concept Symptoms | Categorized generally under negative alterations in cognition and mood 4. | Specifically requires pervasive negative identities (worthlessness, feeling permanently damaged or alienated) 41011. |
Because the DSO symptoms of CPTSD - particularly negative self-concept and emotional numbing - closely mirror the clinical criteria for standard depression, trauma survivors are frequently misdiagnosed with treatment-resistant MDD 101112. Empirical data underscores this overlap. In a study of 1,061 survivors of traumatic injury in Israel, individuals identified by ICD-11 PTSD criteria had 2.12 times the odds of receiving a comorbid depressive disorder diagnosis compared to those identified by ICD-10 criteria alone, suggesting that depressive symptomology is inherently intertwined with the PTSD phenotype 7. Similarly, among treatment-seeking individuals who self-report severe depressive symptoms, the prevalence of underlying CPTSD is exceptionally high, reaching up to 57.1% in certain non-clinical samples exhibiting mood disturbances 1112.
Symptomatology and Autonomic Nervous System Dysregulation
While standard depression and trauma-induced depression share surface-level similarities, their underlying autonomic and physiological mechanisms differ significantly. Trauma fundamentally alters how the human body processes stress at a biological level 13.
In standard MDD, a hallmark symptom is anhedonia - both anticipatory (the reduced capacity to look forward to a rewarding activity) and consummatory (the reduced experience of pleasure during the activity) 21314. Anhedonia is commonly measured using clinical instruments such as the Snaith-Hamilton Pleasure Scale (SHAPS) and the Dimensional Anhedonia Rating Scale (DARS) 213. High severity of anhedonia is robustly associated with poorer outcomes in standard MDD populations, including longer times to remission and a greater likelihood of persistent depressive symptoms despite aggressive pharmacological intervention 1315.
While trauma survivors may also experience profound anhedonia, their presentation is typically rooted in autonomic hypoarousal rather than a primary deficit in dopaminergic reward processing 213. When an individual is subjected to prolonged, inescapable stress, the nervous system may shift from a sympathetic "fight or flight" response (hyperarousal) into a dorsal vagal "freeze" or "shutdown" state (hypoarousal) 1316. This trauma-driven hypoarousal presents clinically as emotional numbness, profound fatigue, systemic withdrawal, and dissociation - a state that mimics standard clinical depression 1317.
Crucially, trauma-induced hypoarousal rarely exists in isolation. It frequently alternates with periods of extreme hyperarousal, manifesting as panic attacks, emotional flashbacks, hypervigilance, and exaggerated startle responses 1318. Standard biogenic depression does not feature trauma-related intrusive memories or severe hypervigilance unless a comorbid anxiety or trauma disorder is present 17. Furthermore, trauma-induced depression is heavily characterized by persistent dissociative symptoms, encompassing both psychoform and somatoform dissociation, which are largely absent in uncomplicated unipolar depression 1012.
Neurobiological Mechanisms of Trauma and Depression
The clinical necessity for specialized trauma therapy over standard depression counseling is firmly rooted in neurobiology. Psychological trauma reorganizes core physiological systems, altering stress regulation, memory encoding, and emotional processing pathways 161920.
Exposure to severe trauma leads to the hyperactivation of the amygdala, the brain's primary threat detection center. This hyperactivation results in exaggerated fear responses and chronic hypervigilance, sustaining the release of stress hormones 161920. Concurrently, trauma impairs the functioning of the hippocampus, which is responsible for consolidating memories and providing temporal context. When hippocampal volume and function are reduced, traumatic memories fail to encode as cohesive autobiographical narratives. Instead, they are stored as fragmented sensory experiences, resulting in the phenomenon of flashbacks where the individual experiences the trauma as an immediate, present-tense threat 1620.
Furthermore, acute trauma triggers a functional decrease in the activity of the dorsolateral prefrontal cortex, the cortical region responsible for executive functioning, logic, language, and emotional inhibition 162221. When the amygdala detects a threat, it can override prefrontal cortical control to facilitate immediate survival responses 1620. This neurobiological reality explains why standard talk therapy - which relies heavily on the prefrontal cortex to analyze and restructure thoughts - frequently fails trauma survivors. If a patient is triggered during a standard cognitive therapy session, their prefrontal cortex effectively goes "offline," rendering them unable to engage in rational cognitive restructuring 2221. The traumatic imprint remains trapped in the non-verbal, subcortical regions of the brain and the body's autonomic nervous system 2222.
Additionally, trauma induces significant dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, altering cortisol levels and contributing to the chronicity of depressive symptoms 11923. Epigenetic modifications, particularly in stress-related genes such as FKBP5, have been documented in trauma survivors, indicating that trauma exposure alters neurobiology at a cellular level and may facilitate the intergenerational transmission of trauma-related psychopathology 2324.
Top-Down and Bottom-Up Treatment Paradigms
Because trauma simultaneously impacts higher-order cognitive functions and deep subcortical survival systems, therapeutic interventions are broadly categorized into "top-down" and "bottom-up" approaches. Understanding these dual paradigms is essential for determining the appropriate treatment pathway and differentiating standard depression therapy from trauma resolution.
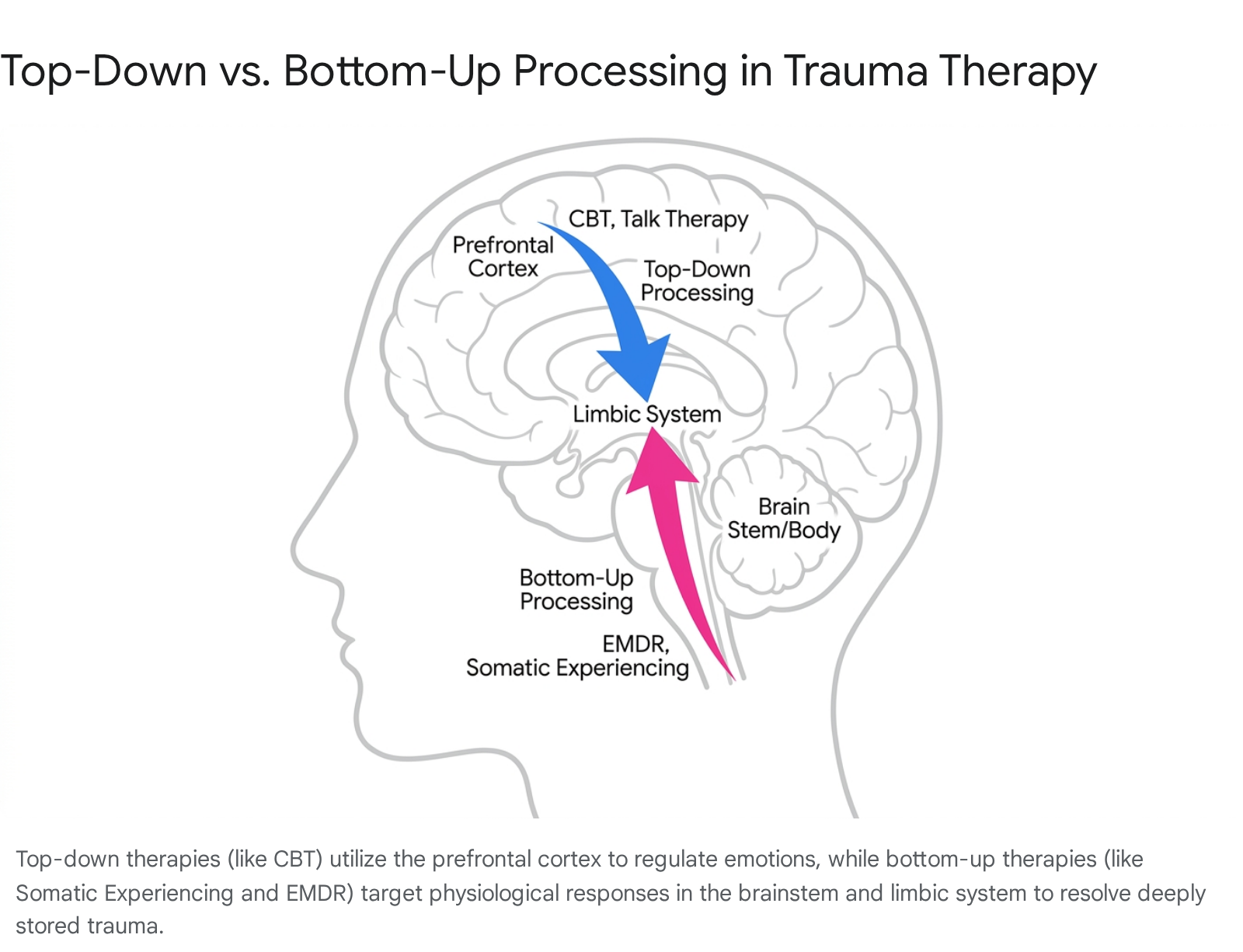
Top-down therapies engage the higher cortical regions of the brain, utilizing the prefrontal cortex to influence the limbic system and regulate emotional states 2225. The primary mechanism involves identifying negative thought patterns, creating coherent narratives, and restructuring conscious beliefs 2225. Standard Cognitive Behavioral Therapy (CBT), the frontline treatment for unipolar depression, is a quintessential top-down approach. It operates on the premise that thoughts drive feelings and behaviors; therefore, altering distorted thoughts will alleviate emotional distress 222629.
While top-down therapy is highly effective for standard depression and general anxiety, it is often inadequate for complex trauma. When a physiological trauma trigger occurs, attempting to rationalize the fear through cognitive reframing is ineffective because the survival response operates subcortically, reacting faster than conscious thought 222126.
Bottom-up processing centers on the body's physiological responses and the subconscious holding of trauma 2222. These methods target the brain stem and limbic system directly, aiming to regulate the autonomic nervous system before engaging the conscious, reasoning mind 22. Bottom-up approaches operate on the principle that the body must achieve physiological safety before the mind can process a traumatic memory. Techniques include noticing physical sensations, tracking nervous system states, and utilizing movement to release trapped survival energy 1627. Modalities utilizing bottom-up mechanisms include Somatic Experiencing, Sensorimotor Psychotherapy, and Eye Movement Desensitization and Reprocessing (EMDR) 222527. Integrating bottom-up regulation with top-down cognitive processing is considered the optimal clinical strategy for achieving comprehensive trauma resolution 162225.
Evidence-Based Modalities for Trauma Recovery
When an individual presents with trauma-induced depression or CPTSD, clinicians rely on specific, empirically validated therapeutic modalities. The American Psychological Association (APA) 2025 Clinical Practice Guideline for the Treatment of PTSD identifies several top-tier interventions, moving beyond simple symptom management to target the deep neurobiological roots of trauma 28. The selection of a specific modality depends on the patient's capacity for emotional regulation, the complexity of the trauma history, and the presence of dissociative symptomatology.
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) is an extensively researched, highly structured intervention originally developed for children and adolescents, though its principles are successfully adapted for adult populations 29333035. Recognized as a first-line treatment by the APA, TF-CBT is a blended approach that combines top-down cognitive restructuring with gradual exposure techniques 2836.
The TF-CBT protocol requires the patient to construct a trauma narrative, systematically confronting trauma-related memories and avoidance behaviors 303531. Concurrently, the therapist aids the patient in identifying and correcting maladaptive cognitive appraisals related to the trauma, such as generalized fears or unfounded self-blame 3031. The efficacy of TF-CBT is robustly supported by clinical literature; a study analyzing 85 patients in routine clinical care in Germany demonstrated massive treatment effects (Cohen's d > 2.0) for self-reported and clinician-administered PTSD scales, with effects remaining stable over long-term follow-up 32. Further studies in low- and middle-income countries, such as those evaluating abbreviated TF-CBT in South African adolescents, confirm its capacity to significantly reduce both PTSD severity and comorbid depression 29.
Despite its strong empirical backing, TF-CBT possesses specific clinical limitations. The gradual exposure component can temporarily exacerbate distress and is frequently contraindicated for patients presenting with active suicidality, severe parasuicidal behaviors, or significant externalizing conduct disorders 36. Furthermore, patients exhibiting severe dissociation or psychosis may be unable to engage with the exposure components without significant prior stabilization 3631.
Eye Movement Desensitization and Reprocessing (EMDR)
Eye Movement Desensitization and Reprocessing (EMDR) is a prominent trauma-focused therapy grounded in the Adaptive Information Processing (AIP) model. The AIP model posits that traumatic memories are stored dysfunctionally in isolated neural networks, preventing their integration with adaptive, functional memory systems 33. EMDR facilitates memory reconsolidation through bilateral stimulation - typically horizontal eye movements, tactile taps, or auditory tones - while the patient briefly focuses on the traumatic memory and its corresponding negative somatic and cognitive sensations 33.
The bilateral stimulation is hypothesized to tax working memory and facilitate interhemispheric communication, mirroring the memory processing mechanisms inherent to Rapid Eye Movement (REM) sleep 1633. This dual-attention mechanism desensitizes the emotional charge of the memory, allowing the brain to spontaneously reprocess and integrate the trauma into a cohesive narrative 33.
While designated as a highly effective second-line treatment in the 2025 APA guidelines, EMDR carries stringent contraindications 28. Successful EMDR requires the patient to maintain dual awareness - the cognitive capacity to remain anchored in the present physical environment while simultaneously accessing highly distressing past material 4034. Consequently, standard EMDR is heavily contraindicated for individuals with active psychosis, unmanaged substance use disorders, unstable medical conditions, or severe dissociative conditions, such as Dissociative Identity Disorder 40344235. Administering EMDR to patients lacking sufficient emotional regulation skills can result in severe emotional flooding, between-session destabilization, and re-traumatization 3442.
Internal Family Systems (IFS)
Internal Family Systems (IFS) is an exploratory, systemic approach that conceptualizes the human psyche as a naturally multiple system composed of relatively discrete subpersonalities or "parts," overseen by an undamaged, core "Self" 263637. In the context of trauma recovery, IFS views symptoms not as pathological deficits, but as extreme protective strategies developed by the internal system to ensure survival and prevent emotional overwhelm 3638.
The IFS model categorizes internal parts into three primary archetypes: * Exiles: Vulnerable, frequently child-like parts that carry the raw emotional pain, terror, and shame of the original traumatic events. They are banished from conscious awareness to protect the individual from psychological collapse 373839. * Managers: Proactive protective parts that attempt to control the individual's environment, relationships, and internal state to ensure the Exiles are never triggered. Common Manager strategies include perfectionism, hyper-intellectualization, emotional detachment, and chronic avoidance 373839. * Firefighters: Reactive protective parts that emerge when Manager strategies fail and an Exile's pain breaks through to consciousness. Firefighters employ extreme, impulsive tactics - such as substance abuse, binge eating, self-harm, or severe dissociation - to extinguish the psychological pain immediately, regardless of the collateral damage to the individual's life 3738.
IFS therapy aims to help the client access their core Self, characterized by intrinsic compassion, curiosity, and calm. From this state of Self-leadership, the client builds trusting, non-judgmental relationships with their protective parts (Managers and Firefighters). Once the protectors trust the Self, they grant permission to access, witness, and eventually "unburden" the traumatized Exiles, allowing the internal system to return to a state of harmony 363840.
IFS is particularly highly regarded for treating CPTSD, chronic shame, and attachment trauma, as it fundamentally reduces internal polarization and fosters profound self-compassion 26293940. However, IFS has structural and empirical limitations. It is an open-ended, fluid modality that lacks the rigid, goal-oriented structure of CBT, which may frustrate patients seeking immediate, practical symptom management 2649. Furthermore, the empirical evidence base for IFS, while demonstrating significant efficacy in pilot trials for PTSD and depression, lacks the massive volume of randomized controlled trials (RCTs) supporting CBT and EMDR 294041. Clinically, IFS requires significant specialized training; an inexperienced practitioner attempting to bypass protective parts too quickly to access Exiles risks severely destabilizing the patient 37.
| Therapy Modality | Core Mechanism | Primary Indications | Key Limitations & Contraindications |
|---|---|---|---|
| Trauma-Focused CBT (TF-CBT) | Top-down cognitive restructuring paired with structured, gradual exposure to trauma narratives 3035. | PTSD, trauma-induced depression, anxiety in youth and adults 293335. | May be contraindicated for active suicidality or severe externalizing conduct disorders without prior stabilization 36. |
| EMDR | Bilateral stimulation facilitating adaptive information processing and memory reconsolidation 1633. | Single-incident PTSD, specific phobias, targeted complex trauma processing 33. | Contraindicated for active psychosis, unmanaged substance abuse, and severe, unmanaged dissociative disorders 403442. |
| Internal Family Systems (IFS) | Systems-based parts work focusing on unburdening Exiles and establishing internal Self-leadership 3637. | CPTSD, chronic shame, severe inner conflict, deep attachment trauma 3940. | Requires long-term commitment; limited massive RCT data; significant risk of destabilization if protective parts are bypassed forcefully 293741. |
Phased Treatment and Stabilization Protocols
The most defining characteristic of trauma-specific therapy, and the primary factor distinguishing it from standard depression counseling, is the strict adherence to a phased treatment model. The International Society for Traumatic Stress Studies (ISTSS), the World Health Organization (WHO), and the APA 2024 Professional Practice Guidelines for Working with Adults with Complex Trauma Histories all explicitly recommend a sequential, triphasic approach 2842434445.
The standard triphasic model consists of three distinct stages: 1. Phase 1: Safety and Stabilization 2. Phase 2: Trauma Processing and Remembering 3. Phase 3: Integration and Reconnection 424446.
A pervasive and dangerous misconception among patients and novice clinicians is that trauma therapy begins by immediately discussing and processing the traumatic events 4656. In clinical reality, plunging prematurely into trauma narratives without an adequate psychological foundation is highly contraindicated and can precipitate severe emotional flooding, psychiatric crises, and clinical re-traumatization 42465647. The APA emphasizes this through the "HISTORY" framework, where the "S" dictates that sequencing must prioritize stabilization and skill-building prior to any direct trauma exposure 2843.
Phase 1: Establishing Safety and Coping Mechanisms
Phase 1 (Stabilization) is entirely focused on the present. The clinical objective is not to explore the past, but to equip the patient's nervous system to handle distress 4658. Stabilization protocols routinely involve extensive psychoeducation, teaching the patient about the neurobiology of trauma, polyvagal theory, and the concept of the "window of tolerance" to systematically reduce the shame associated with their autonomic symptoms 165658.
Clinicians guide patients in developing robust grounding techniques, sensory regulation skills, and containment strategies to actively manage emotional flashbacks and dissociative episodes 4647. This phase also requires addressing acute ongoing external crises, establishing safety plans for self-harm, managing substance abuse, and securing stable living situations 3558. The duration of the stabilization phase varies dramatically based on clinical presentation; for single-incident trauma, it may last only a few sessions, while for severe CPTSD or highly dissociative patients, stabilization can require months or years of dedicated psychotherapeutic work before Phase 2 processing is medically appropriate 4558.
Assessing Readiness for Trauma Processing
Transitioning to Phase 2 (Trauma Processing) requires meticulous clinical assessment. Indicators of successful stabilization include a demonstrable reduction in the frequency and intensity of symptom crises, the verified ability to maintain dual awareness during distress, the consistent and autonomous use of self-soothing strategies outside of sessions, and the establishment of a strong, secure therapeutic alliance 47. Only when these clinical criteria are definitively met do therapists employ processing modalities like EMDR, TF-CBT, or deep IFS exile work to safely reconsolidate the traumatic memories without overwhelming the patient's regulatory capacity 464758.
Practitioner Competency and Clinical Standards
When seeking care for suspected trauma-induced depression, individuals and referring practitioners must navigate a mental health landscape where marketing terminology can be opaque. A critical ethical and practical distinction exists between a clinician who is "trauma-informed" and one who is "trauma-trained" 596061.
Trauma-Informed Practice (TIP) is a foundational paradigm rather than a specific clinical intervention. A trauma-informed professional operates with the baseline understanding that trauma is pervasive and fundamentally shapes behavior, shifting the operational question from "What is wrong with you?" to "What happened to you?" 596062. The core principles of a trauma-informed approach involve creating physical and emotional safety, ensuring transparency, empowering the client through choice, and actively avoiding systemic practices that might inadvertently re-traumatize the individual 6048. While every modern therapeutic and medical setting should operate from a trauma-informed baseline, this framework alone does not provide the clinical mechanisms necessary to actively treat and resolve complex trauma 596048.
Trauma-Trained Therapy, conversely, refers to active clinical intervention administered by a licensed mental health professional who has undergone specialized, post-graduate education in specific, evidence-based trauma processing modalities 596061. Trauma-trained clinicians possess a deep, structural understanding of trauma neurobiology, dissociation metrics, and the rigorous application of phased treatment protocols 5961. They are specifically qualified to execute targeted processing therapies such as EMDR, TF-CBT, or Somatic Experiencing 596048.
If a patient presents with trauma-induced depression, regular talk therapy with a trauma-informed counselor may provide a validating and supportive environment for temporary symptom management. However, fully resolving the root neurological and psychological injury requires the precise expertise of a trauma-trained specialist executing structured, phased trauma processing 59606248. Ethical guidelines suggest that clinicians who are only trauma-informed have a professional responsibility to refer patients exhibiting severe trauma pathology to specialists to ensure the patient's well-being and to avoid practicing outside their clinical scope 59.
Conclusion
Determining whether an individual requires specialized trauma therapy or standard therapy for depression relies on a comprehensive clinical evaluation of symptom etiology, specific diagnostic presentation, and autonomic nervous system regulation. While standard major depressive disorder frequently responds favorably to top-down cognitive restructuring and traditional pharmacotherapy, trauma-induced depression represents a fundamentally distinct neurobiological phenomenon. It is characterized by severe autonomic dysregulation, alternating states of hyperarousal and dorsal vagal shutdown, profound trauma-linked shame, and persistent dissociation.
For individuals suffering from the complex sequelae of acute or developmental trauma, standard depression therapy is rarely sufficient and can occasionally prove invalidating. Recovery necessitates a sequence of specialized care that respects the biological reality of the traumatized brain. By engaging with trauma-trained specialists who strictly adhere to a phase-oriented clinical model - prioritizing physical safety and somatic stabilization before applying targeted, evidence-based processing modalities like TF-CBT, EMDR, or IFS - patients can move decisively beyond the mere management of depressive symptoms toward the authentic neurobiological resolution and integration of traumatic stress.