AI in Healthcare in 2026: What is Real and What is Hype
In 2026, healthcare artificial intelligence has successfully automated administrative tasks and routine radiological imaging, saving clinicians hours of daily labor and significantly reducing hospital overhead. However, in complex clinical areas like predictive diagnostics and drug discovery, the technology remains stalled in the pilot phase, struggling against biological complexities and workflow friction. The industry is now facing a global regulatory reckoning, forcing a shift away from overhyped generative models toward deeply integrated, locally validated clinical tools.
The Reality Check: Why Do So Many AI Healthcare Pilots Fail?
For the last several years, the healthcare industry has been promised a technological revolution. Investors poured billions of dollars into digital health and artificial intelligence, anticipating that neural networks would seamlessly diagnose rare diseases, discover blockbuster drugs, and slash hospital overhead. But as the calendar turns deep into 2026, the healthcare AI ecosystem has hit a structural inflection point. The market has noticeably bifurcated into two distinct realities.
On one side are the highly successful "AI aristocrats" - companies providing highly integrated, ambient, and background automation tools that are quietly becoming essential hospital infrastructure 1. On the other side is a mass extinction event for non-compliant, clinically unverified startups 1. Despite an estimated $30 billion to $40 billion invested globally in enterprise generative AI, recent reports from institutions like MIT indicate that upwards of 95% of enterprise AI pilot projects fail to deliver a measurable return on investment 13.
The primary cause of this failure is not a lack of technological capability, but profound workflow friction. Healthcare is an industry where every minute matters and clinical burnout is at an all-time high. When an AI tool requires a clinician or auditor to log into a separate dashboard outside of their established Electronic Health Record (EHR) system, it adds to their cognitive load rather than reducing it 1. A rollout that appears successful in a controlled laboratory setting routinely fails in practice because it adds friction instead of reducing it 1.
This dynamic has triggered what industry analysts in 2026 call "death by pilot" 1.
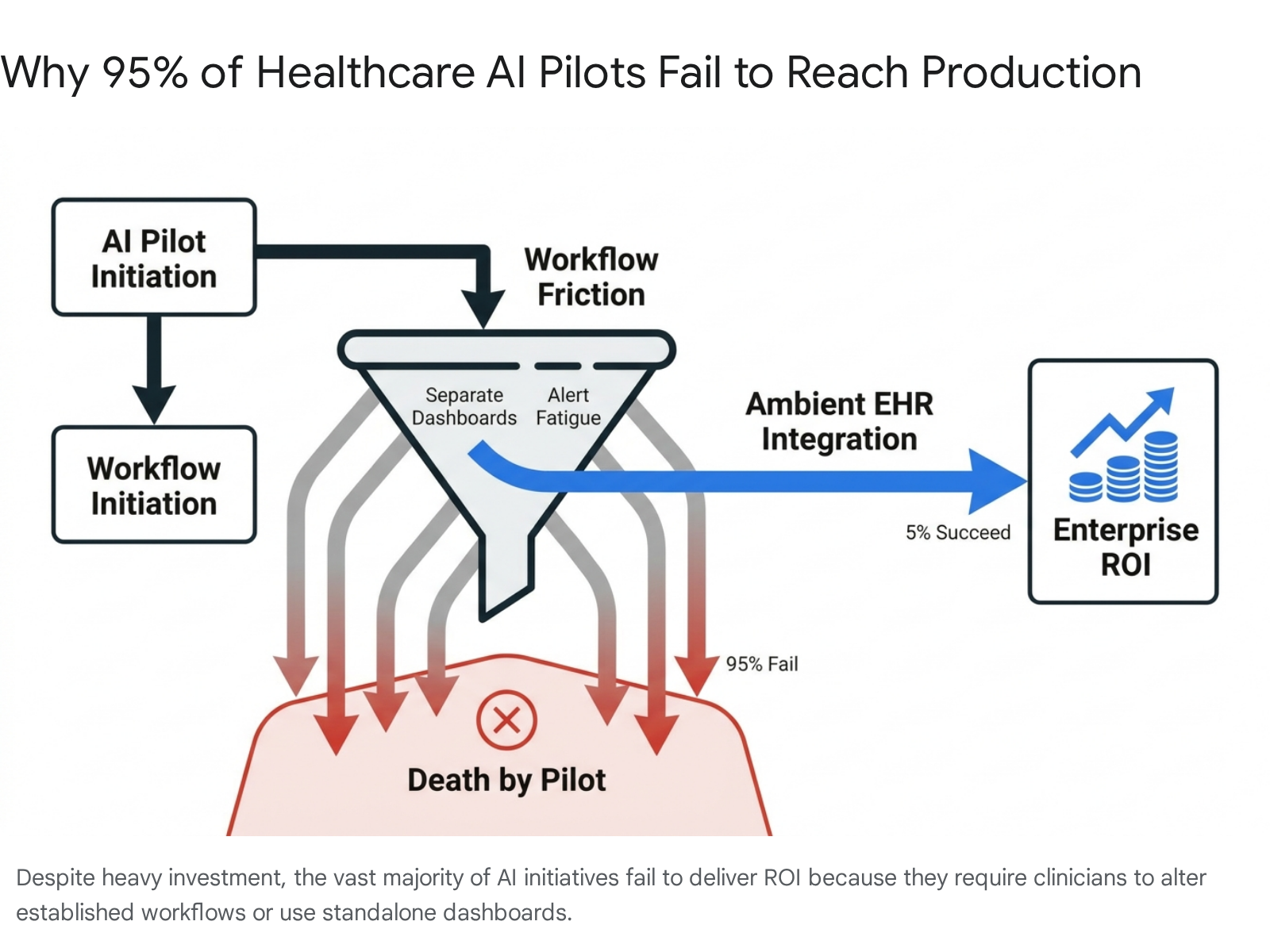
Hospitals enthusiastically test new AI software in controlled, small-scale environments, but refuse to scale them system-wide because the unit economics or workflow integrations fall flat. Consequently, an alarming 35% of digital health startup funding rounds in 2025 were "unlabelled" - a financial maneuver used to hide valuation reality and mask the fact that many early-stage ventures are surviving on bridge financing rather than sustainable, scalable revenue 1. The industry is learning a painful but necessary lesson: technology driven purely by hype solves the wrong problems. To succeed in 2026, AI must meet clinicians where they are, operating invisibly in the background.
What is Approved and Working: The Administrative Revolution
Despite the bursting of the broader AI hype bubble, several specific applications have definitively crossed the chasm into everyday utility. In these domains, AI is no longer an experiment; it is essential infrastructure.
Ambient Scribes and the Evolution of Triage
The most universally celebrated victory for healthcare AI in 2026 is administrative automation. Generative AI "ambient scribes" that securely listen to clinical encounters and automatically draft structured clinical notes have moved from luxury to necessity. These tools are saving clinicians between one and two hours of documentation time per day, resulting in a 20% to 30% reduction in after-hours charting 4. This has had a profound, measurable impact on reducing physician burnout and turnover, which are among the highest hidden costs in modern health systems 2.
The role of the medical administrative assistant is also fundamentally transforming. Instead of performing manual data entry, these professionals are evolving into roles akin to "AI Intake Orchestrators" or "Eligibility Intelligence Leads" 6. By utilizing AI-powered triage chatbots, clinics can deflect low-value phone calls, answer routine patient inquiries 24/7, and automatically route complex cases to the appropriate human staff 673. AI does not replace the judgment and empathy of human assistants; rather, it acts as a highly efficient filter that removes the noise from the system so that human workers can focus on complex patient relationships 9.
Revenue Cycle Management and Medical Billing
Medical billing in the United States is famously labyrinthine, characterized by frequent payer rule changes, coding errors, and rampant claim denials. Nearly 40% of billing errors stem from simple documentation deficiencies, costing the system an estimated $88 billion annually 4.
Artificial intelligence has proven exceptionally adept at managing this complexity. Modern AI billing platforms execute autonomous medical coding, translating patient records into precise ICD-10 and CPT codes with remarkable accuracy and consistency 411. Before a claim is ever sent to an insurance company, predictive AI tools scrub the data against historical denial trends to flag likely rejections, allowing staff to correct the claim proactively 1213.
The results in the real world are striking. For instance, Geisinger Health deployed an autonomous medical coding engine that successfully reduced its coding-related claim denial rate to under 0.1% 4. Auburn Community Hospital in New York reported a 50% reduction in discharged-not-final-billed cases and a 40% increase in coder productivity after integrating AI solutions 14. Furthermore, AI is improving the patient experience by providing transparent, real-time estimates of out-of-pocket costs prior to receiving care, reducing the financial stress associated with surprise medical bills 415.
Comparing Traditional vs. AI-Assisted Medical Billing
| Billing Phase | Traditional Manual Process | AI-Assisted Process (2026) | Primary Benefit |
|---|---|---|---|
| Medical Coding | Human coders manually read charts and assign ICD-10/CPT codes. High error rate (up to 79% in complex specialties). | Natural Language Processing (NLP) extracts data and autonomously assigns codes with high accuracy. | Reduces coding errors by up to 70%, accelerating claim creation. 1114 |
| Claim Scrubbing | Claims are submitted with basic rules-based checks. High risk of missing modifiers or NPIs. | AI cross-checks claims against real-time payer policies and historical denial behaviors before submission. | Prevents avoidable denials; Geisinger reduced coding denials to <0.1%. 413 |
| Insurance Verification | Staff manually call insurers or check portals to verify patient eligibility, consuming hours. | Intelligent platforms perform instant eligibility checks across multiple payers simultaneously. | Reduces administrative labor costs and prevents coverage-related denials. 415 |
| Patient Communication | Patients receive confusing bills weeks after care; staff handle routine phone inquiries manually. | AI chatbots provide real-time updates on balances and coverage; automated systems offer clear cost estimates upfront. | Improves patient satisfaction, reduces confusion, and accelerates patient payments. 415 |
However, revenue cycle management experts warn that AI cannot fix fundamentally broken hospital operations; it simply amplifies the efficiency of the underlying system 12. Highly complex surgical specialties still require the nuanced judgment of experienced human coders to navigate ambiguous clinical documentation 12.
Radiology and Imaging: The Proven Workhorse
Radiology has long been the proving ground for medical AI. By 2026, the U.S. Food and Drug Administration (FDA) tracks more than 1,300 authorized AI-enabled medical devices, with the vast majority serving radiological functions 4.
Computer vision models are now routinely matching, and occasionally exceeding, the diagnostic accuracy of human specialists. In a landmark collaboration between Massachusetts General Hospital and MIT, researchers deployed an AI algorithm that achieved a 94% accuracy rate in detecting lung nodules on CT scans, drastically outperforming the 65% accuracy rate of the human radiologists in the study 16. Real-world data from European screening programs mirror these successes: AI support in routine mammography has been shown to cut radiologist reading times by up to 90% while simultaneously yielding a 17.6% higher cancer detection rate 4.
The Cost-Effectiveness Reality Check
Despite these clinical victories, the economic realities of AI in radiology are heavily nuanced. A systematic review of economic models published in Radiology: Artificial Intelligence in late 2025 revealed that AI does not automatically guarantee cost savings 518. The researchers concluded that current evidence on the cost-effectiveness of AI in radiology is limited, largely model-based, and lacks validation with prospective real-world cost data 67.
The review found that AI is a "selectively powerful enabler" 5. It tends to be highly cost-effective only when deployed in high-volume, resource-intensive workflows - such as national lung cancer or tuberculosis screening programs - where it can replace constrained staff resources or minimize the need for expensive follow-up imaging 518. Cost savings are most likely when the AI automates the evaluation of routine, low-risk scans, freeing up radiologists to focus on complex diagnostic tasks 8. In smaller private practices without the necessary patient volume, purchasing expensive algorithms can quickly become a financial liability 5.
Furthermore, health economists are warning of a severe countervailing effect known as the affordability paradox. While AI drives down the time cost of reading individual scans, its high sensitivity could dramatically increase overall imaging volumes 2. An algorithm might flag thousands of benign, microscopic abnormalities that a human would appropriately ignore, triggering a "care cascade" of unnecessary, expensive, and stressful follow-up biopsies and interventions 2. Thus, while AI improves diagnostic yield, it may paradoxically drive up total systemic healthcare spending through induced demand.
The Piloted Frontier: High Potential, High Friction
Beyond paperwork and pattern recognition in static images, the healthcare industry is attempting to push AI into dynamic, high-stakes clinical decision-making. In these arenas, the technology is highly promising but fraught with biological complexity and implementation hurdles.
Does AI Actually Accelerate Drug Discovery?
Historically, bringing a new molecular entity to market takes 10 to 15 years and costs an average of $2.8 billion, with roughly 90% of candidates that enter Phase I never reaching patients 9. AI promised to shatter this paradigm by simulating molecular binding, predicting toxicology, and optimizing lead compounds entirely in silico (via computer simulation).
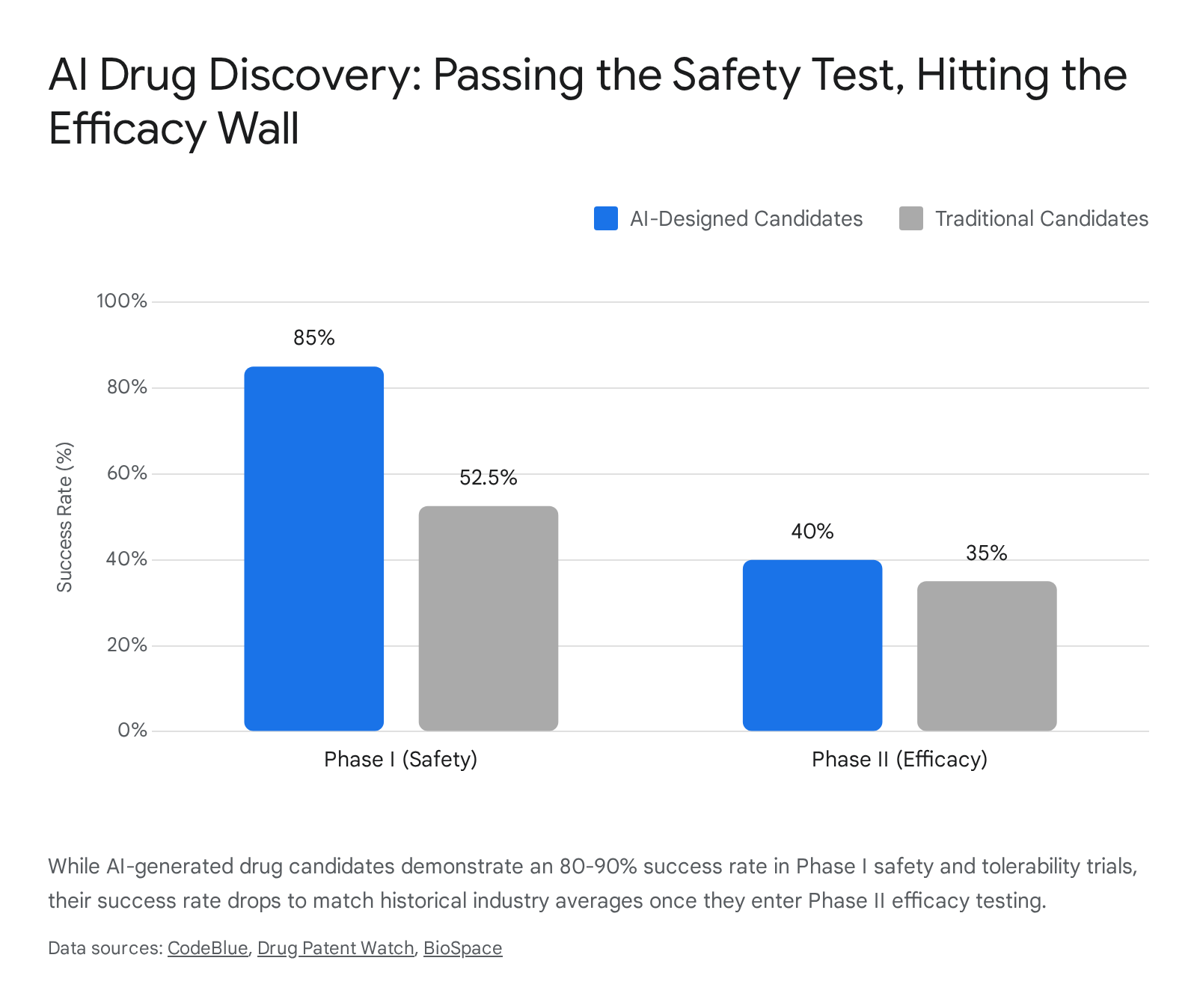
In the earliest stages of the pipeline, AI is delivering on that promise. Generative AI platforms have compressed the traditional target-discovery-to-clinic timeline from several years down to roughly 18 months 1011. Furthermore, AI-native biotech companies are reporting an astonishing 80% to 90% success rate in Phase I clinical trials, compared to the historical industry average of 40% to 65% 2512. By predicting adverse toxicity before a compound is ever synthesized, computational platforms are drastically reducing early-stage failure rates 11.
However, Phase I trials primarily measure safety and human tolerability, not whether the drug actually cures the disease. As these AI-designed molecules advance into Phase II efficacy trials, they are hitting the exact same biological roadblocks as traditional drugs. In Phase II, AI-derived drugs currently exhibit a success rate of about 40% - virtually identical to the historical average for traditionally discovered molecules 2512.
Biology imposes non-negotiable constraints that algorithms cannot bypass 10.
The industry experienced high-profile setbacks in late 2025 and early 2026 that tempered investor exuberance. Verge Genomics' AI-designed ALS drug, VRG50635, failed to show patient benefit in early-stage trials, prompting the company to lay off 90% of its workforce and pivot its business model from drug development to data monetization 13. Similarly, Merck and Eisai's LITESPARK-012 trial missed its primary endpoints in advanced renal cell carcinoma 28.
Conversely, Insilico Medicine made history by advancing Rentosertib (ISM001-055) - the world's first drug entirely discovered and designed by AI - into Phase IIa trials for idiopathic pulmonary fibrosis (IPF), demonstrating encouraging early signs of safety and efficacy 2529. The ultimate verdict on whether AI can fundamentally conquer human biological complexity will arrive between late 2026 and 2027, as a large cohort of over 60 AI-assisted drug candidates produce pivotal Phase II and Phase III readouts 910.
Sepsis Prediction in the ICU
Sepsis - a dysregulated, life-threatening host response to infection - remains one of the leading causes of mortality in Intensive Care Units (ICUs) globally, with in-hospital mortality rates hovering between 20% and 50% 1415. The core challenge in treating sepsis is timing; patients deteriorate rapidly, and every hour of delayed intervention increases the likelihood of death. Traditional diagnostic scoring systems, such as the qSOFA or SIRS criteria, often fail to capture the rapid, heterogeneous physiological decline of critically ill patients 1432.
AI early warning systems leverage continuous streams of electronic health record data, vital signs, and lab results to identify subtle patterns indicative of impending sepsis hours before overt clinical symptoms appear. Multi-center meta-analyses of these Machine Learning (ML) models consistently report high diagnostic performance, with pooled Area Under the Curve (AUC) scores reaching an impressive 0.93 and high pooled sensitivity and specificity 32. Specialized systems, like the TOPSIS-based Classification Fusion (TCF) model and Transformer-based algorithms analyzing hourly data fluctuations, have demonstrated remarkable accuracy in predicting ICU mortality 1516. Tools like Bayesian Health's InSight and the TREWS system have even demonstrated capabilities to reduce mortality and shorten hospital stays in prospective trials 1434.
However, translating these models from the lab to real-world deployment is severely hampered by a phenomenon known as "distribution shift" 35. Deep learning algorithms are notoriously brittle; a model trained on patient data from a high-resource urban hospital may fail catastrophically when deployed in a rural clinic due to differences in patient demographics, baseline health characteristics, and localized clinical workflows 35. Furthermore, highly prevalent tools have faced intense clinical scrutiny. While the widely used Epic Sepsis Model has a sensitivity of approximately 76%, its specificity sits at roughly 67% 34. In practice, this leads to severe alert fatigue, as critical care physicians are bombarded with false positives that disrupt their workflow 34.
Finally, the "black-box" nature of advanced algorithms, such as XGBoost or Long Short-Term Memory (LSTM) networks, creates a crisis of trust 17. If an AI predicts impending septic shock but cannot transparently explain why it reached that conclusion through interpretable variables, physicians are hesitant to act 1718. The holy grail for 2026 is Explainable AI (XAI) paired with Federated Learning - a technique that allows models to train continuously across decentralized hospitals, improving generalizability without requiring the transfer of raw, private patient data 35.
Surgical Robotics: "Google Maps" for Anatomy
Robotic surgery is moving away from simple mechanical assistance toward true computer vision guidance. Accessing the brain for neurosurgery involves drilling and cutting that inherently causes deep-brain anatomy to physically shift and distort 19. Because of this deformation, pre-operative MRI scans quickly become inaccurate representations of the patient's current state.
To solve this, researchers are adapting Simultaneous Localization and Mapping (SLAM) technology - the exact same advanced computer vision algorithms used in self-driving cars - to create real-time, 3D navigational maps of the brain 19. By analyzing live endoscopic video feeds, the SLAM algorithm tracks visual details to determine camera positioning, creating an augmented reality overlay that acts as a dynamic "Google Maps" for the surgeon 1920. This allows surgeons to navigate shifting tissues with submillimeter accuracy without exposing patients to the extra radiation of live intraoperative imaging 19.
Concurrently, AI is mastering the physical execution of surgical tasks. Using imitation learning combined with machine learning architectures similar to those underpinning Large Language Models, researchers have successfully trained da Vinci surgical robots by feeding them hundreds of kinematic videos of seasoned human surgeons 21. These robots have learned to manipulate needles, lift tissue, and suture with the skill of a human doctor 21. Remarkably, the models exhibit emergent behaviors; if the robot drops a needle, it can automatically recognize the error, pick the needle back up, and continue the procedure without requiring a human programmer to hand-code the corrective steps 21.
Systemic Risks and the Integrity Crisis
As AI capabilities expand rapidly, they introduce unprecedented risks. In 2026, the medical community learned exactly how dangerous hallucinated AI data can be to the integrity of global medical knowledge.
The NEJM Fake Image Scandal
In April 2026, The New England Journal of Medicine (NEJM) - widely considered the absolute gold standard of global medical literature - was forced into a highly embarrassing and unprecedented retraction 2223.
The journal had published an "Images in Clinical Medicine" case study featuring an 87-year-old man who had suffered lung injury after inhaling forest fire smoke. The paper included a shocking, pitch-black image of "bronchial casts" pulled from the man's airways, sitting next to a medical measuring tape 2224. The dramatic visual completely bypassed peer review and was published 44. However, internet sleuths quickly noticed something horrifying: the numbers on the measuring tape were jumbled in a nonsensical sequence - a hallmark hallucination of an unsophisticated generative AI image diffusion model 2324.
Following the exposure, the authors requested a retraction, admitting they had used an AI tool to "move the ruler to the top of the image" to make it look neater, claiming ignorance of the journal's strict image manipulation policies 22. The scandal sent shockwaves through the academic community. Generative AI is now capable of creating synthetic, photorealistic medical imagery that can completely fool expert human reviewers 44. If foundational pieces of clinical literature are polluted with exaggerated or fully fabricated baseline data, it directly threatens global standards of care, as diagnostic algorithms and medical students alike train on poisoned datasets. The incident has triggered a desperate, industry-wide scramble to implement automated digital forensics and AI-detection screening across all major medical journals to prevent future fabrications 44.
Global Regulatory Divergence and Infrastructure
In response to the rapid proliferation of both highly effective tools and dangerous hallucinations, 2026 has become the year of regulatory reckoning. Governments worldwide have shifted from issuing vague ethical guidelines to enforcing hard legal mandates on healthcare AI, creating a fractured global landscape.
Comparison of Global Healthcare AI Regulatory Frameworks (2026)
| Country / Region | Key Regulatory Framework & 2026 Status | Primary Impact on Healthcare AI |
|---|---|---|
| Brazil (ANVISA) | RDC 925/2026 (Enacted April 2026) | Mandates local, demographically significant clinical data for Software as a Medical Device (SaMD). Strict data residency (LGPD) forced foreign firms to halt or delay launches. 25 |
| South Korea (MFDS) | Digital Medical Products Act & AI Basic Act (Enacted Jan 2026) | Classifies health AI as "High-Impact." Launched a fast-track cutting market entry from 490 days to 80-140 days for validated tools. 4647 |
| India (CDSCO) | Draft Guidance on SaMD (Operationalizing in 2026) | Introduces an "Algorithm Change Protocol" requiring developers to document, validate, and report continuous AI retraining or model updates. 4849 |
| Indonesia | UU PDP (Personal Data Protection) & SATUSEHAT | Strict data privacy enforcement starting Oct 2026. The SATUSEHAT platform now integrates records for 270M patients, forming the secure data backbone for future AI. 5051 |
| Singapore | AI Verify 2.0 & AIHGle 2.0 Guidelines | Focus on systemic scaling rather than pilots. Heavy integration of AI governance into the national AimSG and HealthHub ecosystems. 262728 |
The Brazilian Shockwave
Perhaps the most aggressive regulatory move came from Brazil's National Regulatory Agency (ANVISA). In April 2026, ANVISA enacted Resolution RDC 925/2026, a surprise regulation that completely blindsided the international MedTech community 25. The rule targets AI diagnostic software and demands that clinical validation data must include a demographically significant subset of the local Brazilian population 25.
Previously, European and American startups relied on a "one-size-fits-all" global strategy, leveraging their FDA clearances or CE marks to fast-track entry into Latin America's largest market. Under the new rule, gold-standard US clinical data is deemed insufficient if it does not prove the algorithm is effective and unbiased against Brazil's diverse genetic and socioeconomic makeup 25. Combined with draconian cybersecurity mandates tied to Brazil's General Data Protection Law (LGPD), the resolution has forced global firms to either invest millions in time-consuming local clinical trials and local data centers, or abandon the market entirely 25.
Asia's Strategic Acceleration
In stark contrast to Brazil's protectionist hurdles, Asian regulators are largely treating AI as a sovereign competitive advantage and are streamlining pathways for innovation. South Korea successfully implemented the second phase of its Digital Medical Products Act (DMPA) alongside its AI Basic Act in January 2026 46. To spur rapid adoption, the Ministry of Food and Drug Safety (MFDS) launched an aggressive fast-track system. For innovative AI medical devices that have already passed internationally recognized clinical evaluations, the time to enter the South Korean healthcare market has been slashed from a sluggish maximum of 490 days down to just 80 to 140 days 47.
India's Central Drugs Standard Control Organization (CDSCO) tackled a uniquely modern problem: AI algorithms are designed to continuously learn and change. Traditional medical device regulations approve a static, unchanging product. To modernize oversight, India introduced the "Algorithm Change Protocol" 4849. This framework requires developers to pre-define and document how their machine learning models will adapt over time. Once the protocol is approved, predefined algorithmic updates - such as model retraining on new patient data - can proceed without requiring a brand-new, lengthy regulatory approval process for every minor tweak, provided safety and post-market surveillance obligations are met 4849.
Meanwhile, Indonesia has taken a highly methodical approach. Rather than rushing comprehensive AI regulations - which were debated and subsequently pushed back to early 2026 - the country focused intensely on building the requisite digital infrastructure 29. The government's national digital health platform, SATUSEHAT, successfully integrated 91% of primary care clinics and 95% of hospitals by January 2026 5130. The platform securely holds interoperable electronic medical records for approximately 270 million patients 51. This unified, standardized data lake positions Indonesia to deploy population-level AI analytics far more efficiently than the highly fragmented health systems of Western nations, provided they successfully navigate the stringent enforcement of their Personal Data Protection (UU PDP) law slated for late 2026 5030.
Africa's Infrastructure Dilemma
In Africa, AI is simultaneously viewed as a leapfrog technology and a castle built on sand 31. South Africa is leading the continent's regulatory push, with regions like the Western Cape issuing policy frameworks aimed at utilizing AI to counteract severe systemic physician shortages 58. With the public sector operating at a practitioner-to-patient ratio of just 0.3 per 1,000 - far below WHO benchmarks - AI decision-support systems and remote triage are seen as essential tools for survival 5832.
Global philanthropy is also stepping in to accelerate deployment. The Gates Foundation and OpenAI recently launched a $50 million pilot initiative to deploy AI capabilities across 1,000 primary healthcare clinics, starting in Rwanda 31. However, local health experts and researchers have heavily criticized the sequence of these investments 31. High-end generative AI is fundamentally useless in a rural clinic that suffers from daily rolling blackouts or lacks basic internet connectivity 31. With internet penetration in some low-income regions sitting at just 23%, deploying San Francisco-designed AI tools in rural East Africa without first establishing stable power grids and basic digital literacy is structurally doomed 31. The consensus among African health researchers in 2026 is that AI must be integrated thoughtfully as the "cherry on top" of a solid infrastructure, and must be governed locally to prevent a new form of digital dependency 3133.
Bottom line
In 2026, artificial intelligence is no longer an emerging concept in healthcare; it is an active participant. Ambient scribes, automated medical billing, and baseline radiological triage algorithms have successfully integrated into everyday workflows, proving their immense value by reducing burnout and saving hospital systems millions in administrative overhead. Conversely, highly complex applications like end-to-end drug discovery and predictive ICU modeling are facing a harsh reality check as they transition from controlled environments to the unpredictable complexities of human biology and real-world hospitals. Ultimately, as global regulators demand localized data and startups face an economic reckoning, the healthcare AI industry is shifting its focus away from raw technological capability and toward frictionless workflow integration and unimpeachable clinical safety.