Will Centanafadine Be Approved for ADHD by July 2026
Direct Answer: Centanafadine is highly likely to receive FDA approval as a new non-stimulant ADHD treatment by its confirmed Prescription Drug User Fee Act (PDUFA) target action date of July 24, 2026. Granted Priority Review following robust Phase 3 clinical trial data, the drug demonstrates significant symptom reduction with a highly favorable safety profile. If approved, it will offer a critical first-in-class alternative for patients amid ongoing, systemic stimulant shortages.
The landscape of attention-deficit/hyperactivity disorder (ADHD) treatment in the United States has been fundamentally destabilized over the past several years. As of mid-2026, the nation remains gripped by an unprecedented and systemic shortage of stimulant medications, leaving millions of patients unable to consistently access foundational treatments like mixed amphetamine salts (Adderall) and lisdexamfetamine (Vyvanse) 11. Finding that an essential medication is suddenly unavailable is deeply unsettling, disrupting the stability of daily routines, academic performance, and occupational functioning 11. While public discourse frequently attributes these shortages to increased telehealth prescribing during the pandemic or stringent Drug Enforcement Administration (DEA) production quotas, recent epidemiological and economic analyses reveal a much more complex, and troubling, etiology.
According to a landmark study published in JAMA Health Forum, the crisis is rooted in profound vulnerabilities within the global pharmaceutical supply chain 23. Researchers identified that a 36.7% decline in raw amphetamine imports to the U.S. and a 17.1% decline in phenylacetone (a key stimulant precursor) in 2022 created an environment where manufacturers were physically incapable of meeting demand, fulfilling only 70% of their allotted DEA quotas 23. This supply chain failure has had devastating ripple effects. With an estimated 15.5 million adults and 7 million children diagnosed with ADHD in the U.S., over 70% of patients reported difficulty filling their prescriptions during the height of the shortage, leading to fragmented care, abrupt withdrawal symptoms, and severe cognitive impairment 134. For patients and clinicians alike, this volatile landscape underscores an urgent necessity: the market desperately requires highly effective therapeutic options that completely bypass the fragile, highly regulated stimulant supply chain. The anticipated approval of centanafadine offers precisely this lifeline - a novel, once-daily therapeutic option that provides robust symptom control without the severe side effects or supply chain vulnerabilities typical of traditional stimulants.
What is centanafadine?
Centanafadine is an investigational, first-in-class non-stimulant medication developed by Otsuka Pharmaceutical for the treatment of ADHD in children, adolescents, and adults 56. Originally developed under the developmental code name EB-1020 by Euthymics Bioscience (and later spun off to Neurovance before being acquired by Otsuka in 2017 for up to $250 million), the drug represents an entirely new pharmacological approach to managing neurodevelopmental attention deficits 78. Pharmacologically, it is classified as a norepinephrine, dopamine, and serotonin reuptake inhibitor (NDSRI), establishing a unique mechanism of action in the ADHD therapeutic landscape 489.
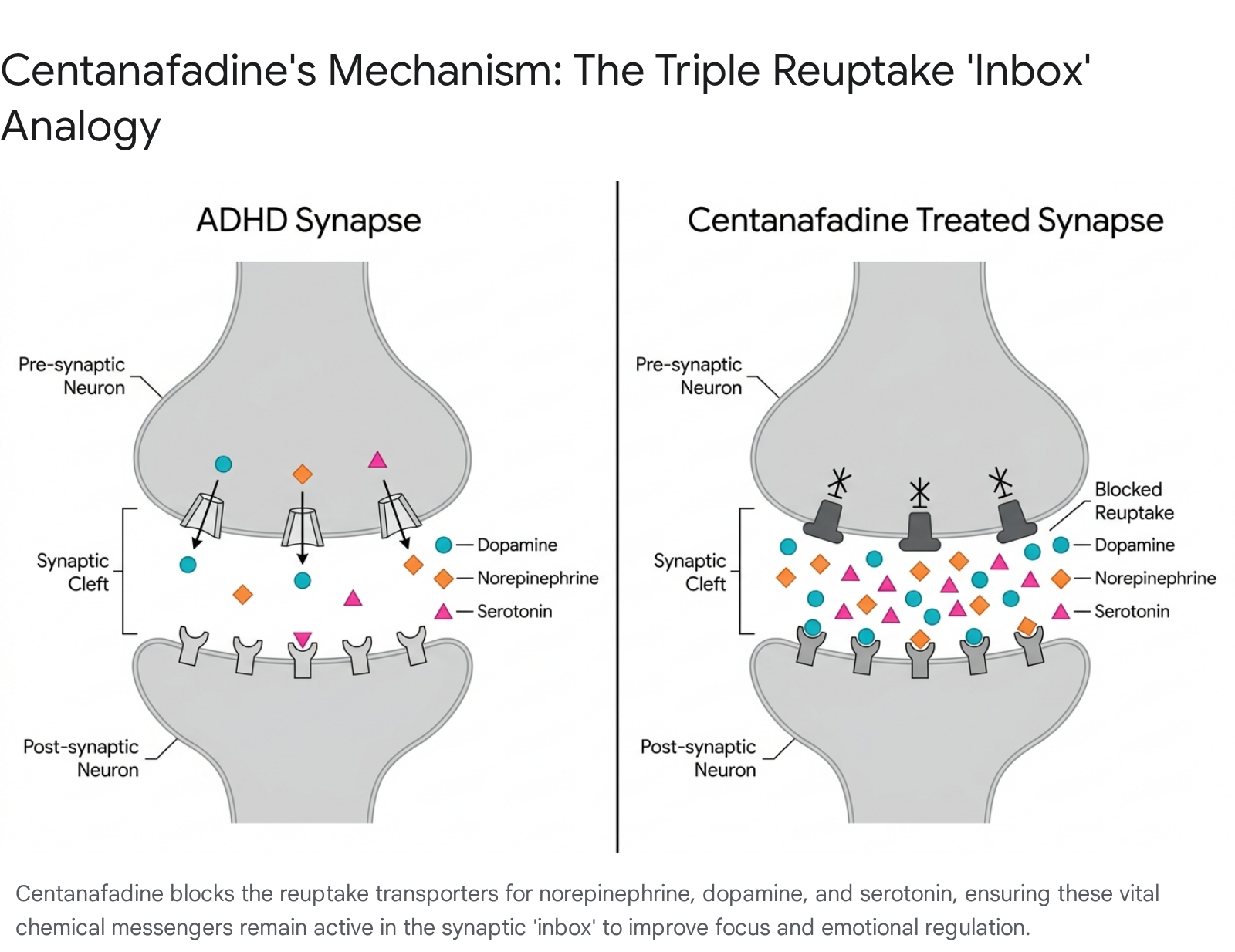
To fully grasp the mechanism of centanafadine, it is helpful to use an accessible real-world analogy: the brain's synaptic "inbox." In the human nervous system, neurons communicate by releasing chemical messengers (neurotransmitters) into a microscopic gap between cells known as the synapse. This gap functions much like an email inbox. In an individual with ADHD, the transporters responsible for clearing these chemicals act like an overly aggressive "auto-delete" function, reabsorbing the messengers back into the sender's outbox too quickly. Because the messages are deleted before the receiving cell has a chance to fully read and process the information, the brain experiences chronic deficits in focus, sustained attention, and impulse control. Centanafadine acts as a specialized, highly calibrated blocker on this outbox mechanism. Specifically, it prevents the rapid reuptake of three distinct messengers - norepinephrine, dopamine, and serotonin - at an optimized inhibitory ratio of 1:6:14 4710. By keeping these critical neurotransmitters in the synaptic inbox longer, the receiving neurons can properly register and process the signals, resulting in sustained improvements in attention and behavioral regulation 410.
A pervasive misconception in modern psychiatric care is that non-stimulant medications are simply "weaker" versions of stimulants, utilized only when a patient cannot tolerate first-line therapies. This fundamental misunderstanding conflates clinical efficacy with pharmacological mechanism. Stimulants like amphetamines act primarily as powerful releasing agents; they force a rapid, massive expulsion of dopamine and norepinephrine into the synapse. While this creates a sharp, immediate onset of profound focus, it also triggers the severe physiological "spikes and crashes" associated with euphoria, cardiovascular stress, and debilitating late-day crash fatigue 121114. Centanafadine does not force the unnatural release of these chemicals. Instead, it gently remodels the ambient neurotransmitter environment by inhibiting their reabsorption 7.
Furthermore, unlike any current ADHD medication, centanafadine's unique inclusion of serotonin modulation offers broader therapeutic benefits. In post-hoc exploratory analyses presented at the May 2026 American Society of Clinical Psychopharmacology (ASCP) Annual Meeting, researchers evaluated 744 adults using the Executive Functioning subscale of the Adult ADHD Self-Report Scale (ASRS) Expanded Version 121317. The data demonstrated that beyond improving core ADHD symptoms (inattention, hyperactivity), centanafadine was strongly associated with statistically significant improvements in patient-reported executive function and emotional dysregulation 1213. These are highly nuanced, functionally impairing symptoms that traditional dopamine-heavy stimulants frequently fail to adequately address. Therefore, centanafadine is not a "weaker stimulant," but rather a structurally distinct neuromodulator purposefully designed for steady, broad-spectrum symptom management without the physiological exhaustion of forced dopamine release.
How does it differ from Adderall or Strattera?
Because centanafadine belongs to a completely novel drug class, evaluating its place in the therapeutic hierarchy requires examining how it performs against established standards of care. In the absence of direct head-to-head clinical trials comparing centanafadine to other approved agents, researchers rely on matching-adjusted indirect comparisons (MAIC) to evaluate its relative clinical utility 141915. In these analyses, patient-level data from centanafadine trials is statistically weighted to match the aggregate baseline characteristics (such as age, sex, race, baseline severity scores, and BMI) of patients from historical trials of comparator drugs 141916. This rigorous methodology allows for highly accurate indirect comparisons against popular stimulants like lisdexamfetamine (Vyvanse) and established non-stimulants like atomoxetine (Strattera) and viloxazine ER (Qelbree).
The data from these MAIC analyses - extensively detailed in the Journal of Managed Care & Specialty Pharmacy in 2024 - reveals a distinct and highly relevant trade-off paradigm for clinicians 1617. When compared directly to the high-potency stimulant lisdexamfetamine, centanafadine exhibited a slightly lower magnitude of raw symptom reduction, scoring approximately 6.15 to 6.58 points less in symptom improvement on the Adult ADHD Investigator Symptom Rating Scale (AISRS) 191623. However, this mild reduction in raw, absolute efficacy was offset by an overwhelming superiority in safety and tolerability over the course of 52 weeks of treatment 1624. Patients taking centanafadine experienced a staggering 23.4 percentage-point lower risk of appetite loss, a 19.2 percentage-point lower risk of dry mouth, and a 15.3 percentage-point lower risk of insomnia compared to those treated with lisdexamfetamine 141923.
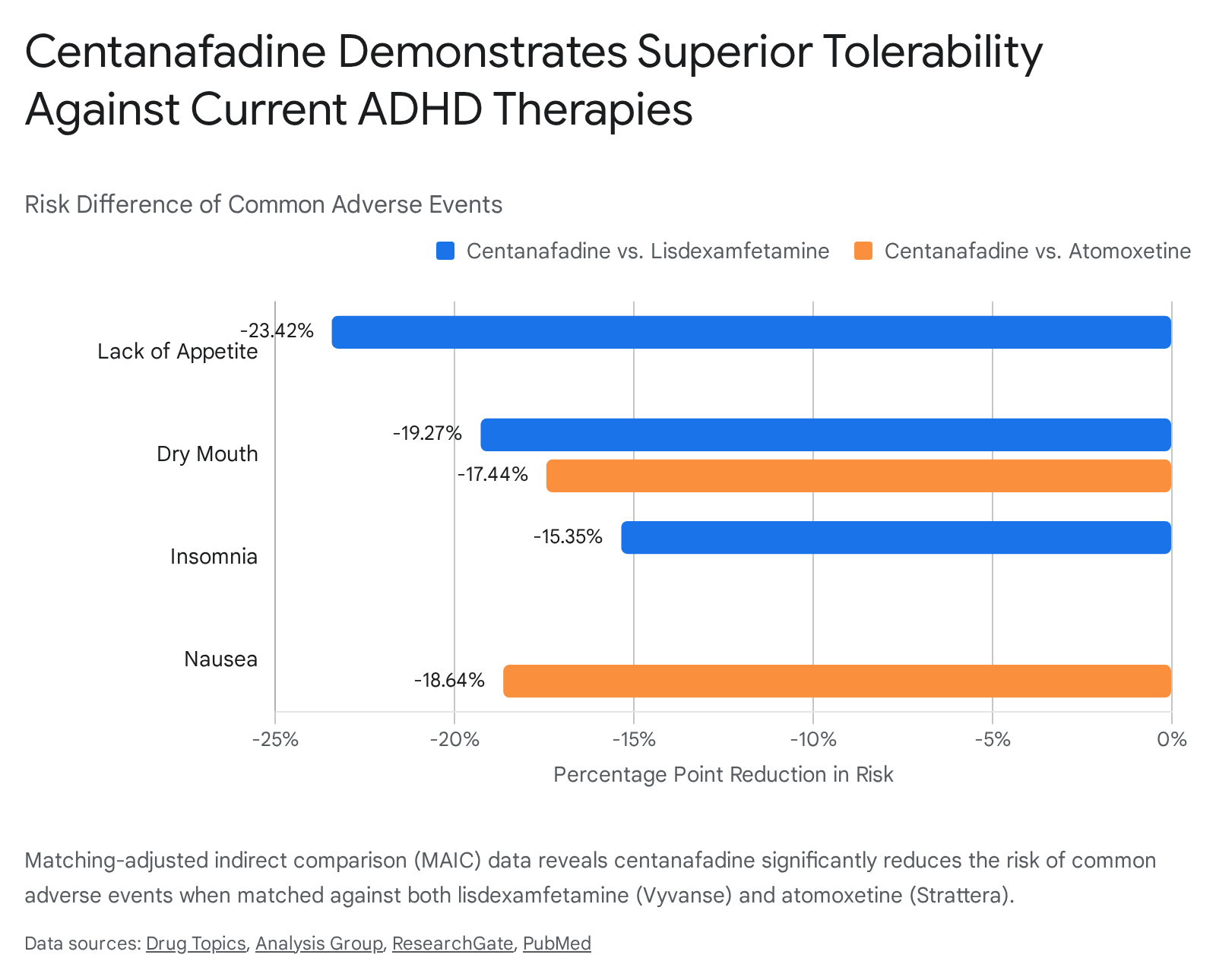
When the analysis pivots to compare centanafadine against its direct competitors in the non-stimulant space, its clinical advantages become even more pronounced. The 2024 MAIC analyses indicate that centanafadine's core efficacy in reducing ADHD symptoms is statistically comparable (non-different) to both atomoxetine and viloxazine ER 191718. Where centanafadine decisively pulls ahead is in its tolerability profile and its rapid onset of action. Against atomoxetine, centanafadine was associated with an 18.6 percentage-point lower risk of nausea, a 17.4 percentage-point lower risk of dry mouth, and significantly lower rates of fatigue and erectile dysfunction 1919. When matched against the newer viloxazine ER formulation, centanafadine demonstrated an 11 percentage-point lower risk of fatigue and a 10.6 percentage-point lower risk of insomnia 141917.
Perhaps most critically for long-term patient adherence, centanafadine operates on a highly accelerated clinical timeline. Traditional non-stimulants require extensive titration periods; atomoxetine can take anywhere from four to eight weeks to reach full clinical efficacy, while viloxazine generally requires between one and four weeks 272829. In stark contrast, multiple Phase 3 trials have documented that high-dose centanafadine visibly separates from placebo, providing statistically significant and clinically meaningful symptom relief as early as week one of treatment 61130.
| Feature | Centanafadine (Investigational) | Viloxazine ER (Qelbree) | Atomoxetine (Strattera) | Lisdexamfetamine (Vyvanse) / Mixed Amphetamine Salts (Adderall) |
|---|---|---|---|---|
| Mechanism of Action | NDSRI (Triple reuptake inhibitor of NE, DA, 5-HT) | NRI (Selective NE reuptake inhibitor) with mild 5-HT activity | NRI (Selective NE reuptake inhibitor) | CNS Stimulant (Releases DA and NE; blocks reuptake) |
| Efficacy Onset Timeline | Significant improvement as early as Week 1 | Initial effects in 1-2 weeks; full effects in 4-6 weeks | Initial effects in 1-2 weeks; full effects in 4-8 weeks | Immediate (within 30-60 minutes) |
| Controlled Substance Status | Expected to be Non-Scheduled (low abuse liability) | Non-Scheduled (Not a controlled substance) | Non-Scheduled (Not a controlled substance) | Schedule II Controlled Substance (High abuse potential) |
| Key Differentiating Side Effects | Mild decreased appetite, headache; significantly lower rates of insomnia and nausea than peers | Somnolence, fatigue, insomnia (lower rates than Strattera) | Severe fatigue, nausea, dry mouth, erectile dysfunction | Severe insomnia, profound appetite loss, cardiovascular stress, anxiety, crash fatigue |
| FDA Status | Under Priority Review (PDUFA: July 24, 2026) | FDA Approved | FDA Approved (Generic available) | FDA Approved (Generic available, subject to profound shortages) |
What are the known side effects?
While centanafadine boasts a superior tolerability profile compared to existing pharmacological agents, it is not entirely free of adverse effects. Extensive safety data has been gathered from four massive, pivotal Phase 3 clinical trials that enrolled pediatric, adolescent, and adult cohorts. Across all demographics, investigators categorized the vast majority of treatment-emergent adverse events (TEAEs) as mild or moderate in severity 5630.
In the pediatric study (NCT05428033), which evaluated children aged 6 to 12 years, patients were randomized to weight-based low-dose centanafadine, high-dose centanafadine, or placebo over six weeks 630. While the low-dose group failed to reach statistical significance regarding symptom reduction, the high-dose group demonstrated robust efficacy 630. In this young population, TEAEs occurred in 39% of the high-dose cohort compared to 25% of the placebo group, with the most frequent complaints being decreased appetite (5%), transient rash (3%), and vomiting (3%) 630. Similar safety profiles were observed in the adolescent trial (NCT05257265, ages 13 to 17), which evaluated fixed doses of 164.4 mg and 328.8 mg 620. Here, common side effects included mild nausea, abdominal pain, fatigue, and isolated incidents of somnolence 4521. In adult populations (ages 18 to 55, evaluated across trials NCT03605680 and NCT03605836 at doses of 200mg and 400mg), the side effect profile was even more concentrated, with the primary clinical complaints limited almost exclusively to decreased appetite and headache 561213.
A critical, defining component of centanafadine's safety profile is its negligible potential for drug abuse and diversion - a severe liability for all Schedule II stimulant medications. Early preclinical studies, followed by a dedicated Phase 1 exploratory human abuse liability trial (NCT02144415), rigorously evaluated the drug's vulnerability to misuse by utilizing an immediate-release formulation in populations with a known history of stimulant abuse 11. The results were unequivocal: the drug was found to be initially aversive and completely unlikely to be abused, demonstrating significantly less abuse liability than either lisdexamfetamine or d-amphetamine 11. Across the subsequent Phase 3 clinical program, incidences of abuse potential-related adverse events remained exceptionally low, confirming that centanafadine provides steady symptom relief without triggering the rapid dopaminergic reward pathways that lead to physical dependence and addiction 112234.
When will it actually be available?
The regulatory trajectory for centanafadine has advanced on a highly accelerated timeline. In November 2025, Otsuka Pharmaceutical officially submitted a comprehensive New Drug Application (NDA) to the FDA, backed by the aforementioned Phase 3 clinical data across all age cohorts 202223. Acknowledging both the robust clinical efficacy of the drug and the urgent, systemic unmet medical need generated by national stimulant shortages, the FDA formally accepted the NDA for Priority Review on January 27, 2026 568. This prestigious designation is reserved for drugs that the FDA believes will provide a significant advancement in the diagnosis, treatment, or prevention of a serious condition, and it actively shortens the agency's standard, year-long review timeline 410.
Crucially, the FDA's acceptance of the NDA officially locked in a Prescription Drug User Fee Act (PDUFA) target action date of July 24, 2026 5912. It is vital for clinicians and investors to understand that this date is not a speculative industry projection or a flexible estimate; it is the strict statutory deadline by which the FDA intends to issue its final regulatory approval decision 524.
If the FDA grants full approval in late July 2026, the timeline for actual patient access and availability in community pharmacies will hinge on the DEA's scheduling process. Historically, when a newly approved drug affects the central nervous system and demonstrates any abuse potential, it must undergo a lengthy secondary review by the DEA to be placed into a specific regulatory schedule (e.g., Schedule II for Adderall or Vyvanse), which can delay market launch by several months. However, because extensive preclinical and human abuse liability data have proven that centanafadine possesses virtually no abuse potential, the consensus among pharmaceutical analysts is that the compound is highly likely to be classified as an unscheduled, non-controlled medication - identical to the regulatory status of atomoxetine and viloxazine 121125. Bypassing the DEA scheduling bottleneck means Otsuka could theoretically commence distribution to regional pharmaceutical wholesalers almost immediately following the FDA's July approval. Consequently, the medication could be accessible to patients by the late summer or early fall of 2026, perfectly timed for the back-to-school season when ADHD medication demand traditionally spikes.
Is centanafadine being reviewed globally?
Despite being developed by Otsuka Pharmaceutical Co., Ltd. - a globally dominant Japanese healthcare corporation with a market capitalization exceeding $31 billion (TYO: 4578) - the immediate commercialization strategy for centanafadine is aggressively and exclusively concentrated on the United States market 38. This prioritization aligns with profound economic realities: the U.S. represents the most lucrative ADHD market globally and is currently the epicenter of the stimulant shortage crisis. Otsuka projects that centanafadine could rapidly scale into a JPY 100 billion ($650 million) peak product in the U.S. alone 8.
As of May 2026, centanafadine does not appear to be under active regulatory review in other major international markets, indicating a phased global rollout strategy. Within the European Union, the European Medicines Agency (EMA) publishes exhaustive monthly logs of medicines under evaluation by the Committee for Medicinal Products for Human Use (CHMP), as well as mandatory lists of products under additional regulatory monitoring. A thorough review of EMA regulatory filings, CHMP evaluation lists, and submission predictability reports through May 2026 yields no evidence of an active marketing authorization application (MAA) for centanafadine in Europe 262728.
Similarly, a review of Otsuka's domestic clinical pipeline and recent regulatory submissions to Japan's Pharmaceuticals and Medical Devices Agency (PMDA) and the Ministry of Health, Labour and Welfare (MHLW) indicates that while the company is aggressively advancing other neurological and oncological drugs in Japan (such as a March 2026 application for Iclusig), centanafadine is exclusively highlighted in corporate communications regarding its U.S. FDA Priority Review status 513. Otsuka is currently enjoying significant pipeline momentum, having recently secured U.S. approvals for the immunoglobulin A nephropathy therapy Voyxact and the hereditary angioedema therapy Dawnzera 842. It is highly probable that Otsuka intends to secure the U.S. FDA approval as an anchor validation, subsequently utilizing the robust U.S. Phase 3 data as the foundational dossier for future international filings in Japan and the European Union post-2026.
Bottom line
The anticipated FDA approval of centanafadine by July 24, 2026, represents a pivotal, paradigm-shifting advancement in ADHD pharmacotherapy. Driven by an innovative triple-reuptake inhibition mechanism that uniquely modulates norepinephrine, dopamine, and serotonin at an optimized ratio, centanafadine actively challenges the outdated clinical assumption that non-stimulants are merely secondary, less effective options to amphetamines. Extensive Phase 3 clinical trials and rigorous matching-adjusted comparative data confirm that while centanafadine may fall slightly short of the raw symptom reduction seen with maximum-dose stimulants, it more than compensates by dramatically lowering the incidence of severe side effects like profound insomnia, appetite loss, and nausea. Crucially, its ability to separate from placebo and provide meaningful symptom relief within the very first week of treatment resolves the primary limitation of older non-stimulants like atomoxetine. For the millions of patients currently navigating the chaotic supply chain shortages of traditional stimulants, centanafadine's rapid onset of action, highly favorable safety profile, expanded efficacy in treating emotional dysregulation, and non-controlled regulatory status position it not just as an alternative therapy, but as a potential new standard of care in comprehensive, broad-spectrum ADHD management.