Why Do We Get Hiccups and What Actually Stops Them
Hiccups are involuntary spasms of the diaphragm followed by the sudden, noisy closure of the vocal cords, a reflex that serves no physiological purpose in human adults. While most everyday hiccups can be stopped by physical maneuvers that increase carbon dioxide in the blood or distract the vagus nerve, episodes that persist for more than 48 hours often point to underlying medical conditions that require specialized pharmacological treatments.
The Anatomy of a Hiccup: What Is Actually Happening?
To understand how to stop a hiccup, it is necessary to examine exactly what is happening inside the body when one occurs. The clinical term for hiccups is singultus, which is derived from the Latin word singult, translating roughly to "the act of catching one's breath while sobbing" 12. This centuries-old translation remains a remarkably accurate description of the physiological event.
A hiccup is not a simple, isolated muscle twitch. It is a complex, highly coordinated event governed by a specific neurological circuit known as the hiccup reflex arc 23. This circuit operates entirely independently from the brain's normal, rhythmic breathing centers, which is why we cannot simply decide to stop hiccuping using our conscious will 4.
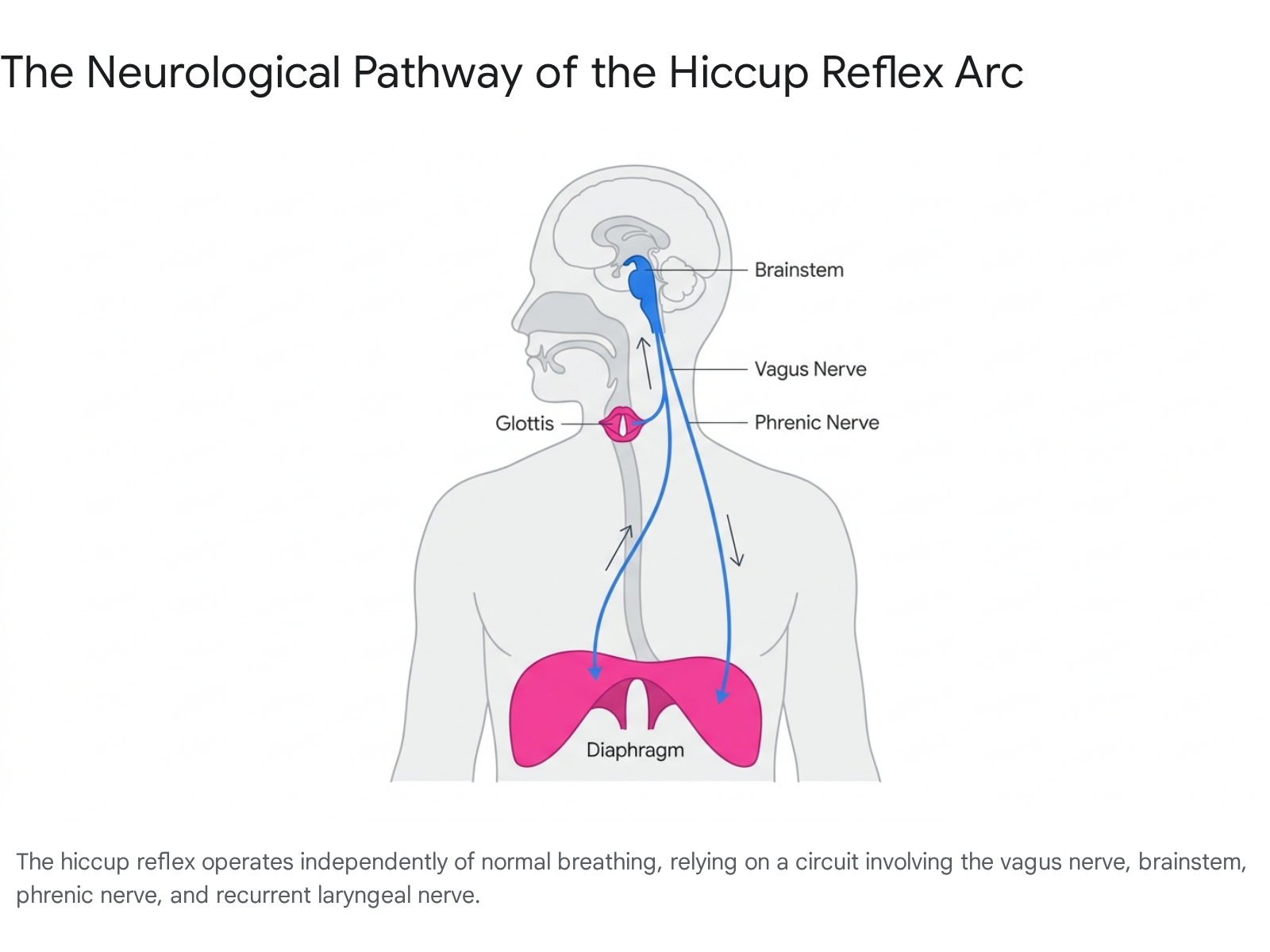
The reflex arc consists of three primary components that must fire in sequence.
The first component is the afferent limb, which acts as the sensory messenger system. Sensory signals travel from the stomach, the esophagus, the throat, and the chest up to the brain. These signals are carried primarily by the vagus nerve, the phrenic nerve, and branches of the sympathetic nervous system spanning the T6 to T12 vertebrae 24.
The second component is the central processing unit, which serves as the command center. The sensory signals reach a diffuse "hiccup center" located deep within the brainstem, specifically involving the medulla oblongata and the reticular formation 46. This processing center relies heavily on specific neurotransmitters - primarily dopamine, serotonin, and gamma-aminobutyric acid (GABA) - to modulate the incoming signals and decide whether to trigger the reflex 35.
The final component is the efferent limb, which executes the physical action. Once the brainstem determines that a hiccup is warranted, it fires motor impulses back down the body. These electrical signals travel rapidly down the phrenic nerves to the diaphragm, the large, dome-shaped muscle that separates the chest cavity from the abdomen 25. Simultaneous signals are sent via the accessory nerves to the intercostal muscles located between the ribs 23.
The Sequence of the Spasm
When the efferent signals arrive, the diaphragm and chest muscles contract violently and erratically. This spasm forces a rapid, massive intake of air into the lungs 35. However, the defining characteristic of a hiccup occurs a fraction of a second later.
Approximately 35 milliseconds after the sudden inhalation begins, a secondary neurological signal travels down the recurrent laryngeal nerve to the throat 46. This signal commands the glottis - the flap of cartilage that protects the vocal cords and airway - to snap completely shut 45.
The rushing column of inhaled air slams abruptly into the closed glottis. This physical collision between air and tissue is exactly what produces the distinct, audible "hic" sound 78. Without the closure of the glottis, a hiccup would simply be a deep, sudden gasp. The combination of the spasm and the glottic closure causes a sharp drop in intra-thoracic pressure, violently altering the physical dynamics of the chest cavity 4.
The Inner Tadpole: Why Did We Evolve to Hiccup?
Hiccups are a universal human experience. In fact, they begin long before we are even born. Ultrasound imaging reveals that human fetuses begin hiccuping in the womb as early as nine weeks into gestation 29. Because fetuses do not breathe air and are surrounded by amniotic fluid, some pediatricians theorize that in-utero hiccups serve as a vital training mechanism. The spasms help strengthen the diaphragm and breathing apparatus, while the glottic closure prevents amniotic fluid from flooding the developing lungs 910.
However, once humans are born and successfully transition to breathing air, the hiccup reflex appears to offer absolutely no physiological advantage 79. This presents a fascinating biological puzzle. If hiccups are fundamentally useless to adult humans - and occasionally harmful or exhausting - why hasn't natural selection engineered this vulnerability out of our anatomy over millions of years?
Evolutionary biologists and paleontologists argue that we cannot understand the human hiccup without looking deep into our evolutionary past. The most prominent consensus is that hiccups are a vestigial remnant, a trait inherited from ancient aquatic and amphibian ancestors 111213.
The Amphibian Gill-Ventilation Hypothesis
The phylogenetic hypothesis, popularized by evolutionary biologist Neil Shubin and detailed in extensive clinical bioassays, argues that the neurological pattern of a human hiccup is not a mistake, but rather an ancient, perfectly preserved breathing program 111217.
Researchers point to the respiratory mechanics of modern amphibians, such as tadpoles. At a specific, transitional stage in their development, tadpoles possess both lungs for breathing air and gills for breathing water 911. When a tadpole is submerged and needs to pump water across its gills, it faces a mechanical problem: it must force water through its mouth and out its gills while simultaneously ensuring that water does not enter its delicate, developing lungs 911.
To achieve this, the tadpole executes a very specific maneuver. It sharply contracts its inspiratory muscles to pull fluid inward, while simultaneously snapping its glottis shut to seal off the airway to the lungs 81113. Neurologically and muscularly, this gill-ventilation pattern is virtually indistinguishable from a human hiccup. It is essentially an extended, rhythmic hiccup utilized for survival 1317.
The evolutionary parallels extend beyond mere physical resemblance, supported by several striking pharmacological and neurological fingerprints: * The Shared Brainstem: The electrical signals that trigger a human hiccup originate in the exact same region of the brainstem that controls gill ventilation in amphibians. In an evolutionary sense, our human brainstems are still running the hardware of our amphibian ancestors 1112. * Carbon Dioxide Sensitivity: In tadpoles, gill breathing is instinctively blocked by elevated concentrations of carbon dioxide, prompting the animal to switch to lung breathing. Similarly, human hiccups can often be suppressed by increasing blood carbon dioxide levels, which is why holding one's breath frequently stops a hiccup attack 1113. * GABA Receptor Activation: Both human hiccups and tadpole gill-breathing are effectively abolished by the administration of baclofen, a muscle-relaxant drug that acts on GABA-B receptors. This shared inhibitory mechanism strongly suggests that both behaviors are governed by the same ancient neural circuitry 1114.
The Mammalian "Burping" Reflex
A second evolutionary theory does not replace the amphibian hypothesis but builds upon it. It suggests that while the biological wiring for the hiccup originated in amphibians, early mammals co-opted and adapted this reflex for an entirely different purpose: facilitating feeding in infants 411.
Gastroenterologists propose that the hiccup reflex is highly advantageous for suckling mammals. When human babies and other infant mammals nurse, they inadvertently swallow significant amounts of air alongside milk 411. The presence of a large air bubble in the stomach triggers mechanoreceptors that fire signals up the afferent limb of the hiccup reflex arc 4.
When the subsequent hiccup occurs, the rapid contraction of the respiratory muscles against a closed glottis causes a massive, sharp drop in intra-thoracic pressure 4. Simultaneously, the reflex temporarily relaxes the lower esophageal sphincter. This creates a vacuum effect that pulls the trapped air bubble from the stomach up into the esophagus, allowing it to easily escape out the mouth as a burp 411.
This mammalian adaptation theory elegantly explains why human newborns spend a staggering 2.5% of their time hiccuping, and why the frequency of hiccups decreases dramatically as children grow older, transition to solid foods, and develop more sophisticated digestive control 11. The hiccup is a primitive, automated gas-venting program that we eventually outgrow, though the neurological wiring remains dormant in our chests for the rest of our lives.
Categorizing the Hiccup: Benign Annoyance or Medical Warning?
For the modern adult, waking up the inner tadpole is usually an accident. The ancient hiccup reflex is highly sensitive, and the long, convoluted paths of the vagus and phrenic nerves make them vulnerable to irritation.
The phrenic nerve, which controls the diaphragm, originally evolved in fish to service gills located in the neck. In humans, because our "gills" migrated downward to become lungs, the phrenic nerve must take an absurdly long and winding route from the base of the skull, down through the chest cavity, and past the heart to reach the diaphragm 1317. This excessive length means there are numerous places where the nerve can be bumped, compressed, or chemically irritated.
When diagnosing hiccups, medical professionals do not focus primarily on the sound or the severity of the spasm. Instead, they categorize hiccups strictly by their duration. The length of an episode is the single most important clinical indicator of whether a hiccup is a benign physiological quirk or a warning sign of serious, underlying systemic pathology 215.
| Clinical Classification | Duration of Episode | Typical Etiology (Causes) | Standard Action Required |
|---|---|---|---|
| Acute / Transient | Less than 48 hours | Rapid eating, gastric distension, alcohol, capsaicin, sudden temperature shifts, emotional stress. | None. Usually resolves spontaneously; non-pharmacological home remedies can expedite relief 215. |
| Persistent | 48 hours to 1 month | Gastroesophageal reflux disease (GERD), moderate nerve irritation, post-surgical complications, medication side effects. | Medical evaluation recommended to identify and treat the underlying physiological or pharmacological cause 151617. |
| Intractable | Longer than 1 month | Central nervous system lesions (stroke, tumors), advanced malignancy, organ failure, severe metabolic imbalances. | Immediate medical intervention, extensive diagnostic workup, and targeted pharmacological or surgical therapy 101518. |
The Triggers of Acute Hiccups
The vast majority of hiccups are acute, resolving within a few minutes to a few hours. These episodes are generally harmless and are most commonly triggered by physical irritation of the nerves in the reflex arc or distension of the stomach, which sits just beneath the diaphragm 15.
When the stomach expands too rapidly, it pushes upward, mechanically agitating the diaphragm and the phrenic nerve branches that innervate it 8. This is why eating a large meal too quickly is one of the most reliable ways to trigger a hiccup 19. Swallowing excess air - a condition known as aerophagia - has the exact same effect. Drinking carbonated beverages, chewing gum, smoking, or even laughing excessively all introduce unwanted air into the stomach, triggering the reflex 101517.
Chemical irritation is also a major culprit. Spicy foods rich in capsaicin directly irritate the stomach lining, causing the attached diaphragm to jiggle and spasm 8. Excessive alcohol consumption is a notorious trigger, as alcohol relaxes the esophageal sphincter, irritates the gastrointestinal tract, and disrupts normal neurological signaling 17.
Even simple environmental changes can set off the reflex. Experiencing a sudden temperature shift, such as drinking a steaming cup of coffee followed immediately by a glass of ice water, can shock the local nerve endings in the esophagus 11516. Furthermore, high-stress situations, anxiety, or sudden excitement can alter breathing patterns and stimulate the sympathetic nervous system, accidentally initiating the sequence 11017.
The Dangers of Persistent and Intractable Hiccups
When hiccups cross the 48-hour threshold, they cease to be a laughing matter. Having the diaphragm violently contract round-the-clock severely impacts a patient's quality of life. Persistent hiccups disrupt normal eating and drinking, leading to rapid weight loss, dehydration, and malnutrition 21517. They prevent restful sleep, resulting in profound exhaustion, depression, and social isolation 2615. In historical extremes, a man named Charles Osborne famously suffered from intractable hiccups for 68 years, from 1922 to 1990, after a farming accident 20.
At the persistent and intractable stages, hiccups are no longer considered a standalone issue. They are viewed as a red flag indicating a more severe underlying disease 101819.
Gastrointestinal Disorders: Gastroesophageal Reflux Disease (GERD) is by far the most common underlying cause of chronic hiccups 1015. Chronic acid reflux continuously bathes the lower esophagus in stomach acid, severely irritating the vagus nerve endings 1019. Recent advancements in high-resolution manometry have even identified a specific "Hiccup-Induced Esophagogastric Waveform." During a hiccup crisis, the esophagogastric junction undergoes sustained, high-pressure contractions, suggesting that chronic hiccups can severely exacerbate swallowing difficulties and chest pain in gastrointestinal patients 2526.
Central Nervous System Lesions: If the brainstem itself is damaged, the hiccup command center can misfire endlessly. Brain tumors, aneurysms, multiple sclerosis, and traumatic brain injuries are well-documented causes of intractable hiccups 21819. A specific type of stroke known as Wallenberg syndrome, which damages the lateral medulla, is particularly notorious for causing relentless hiccups by directly destroying the regulatory pathways of the reflex arc 18.
Metabolic and Systemic Issues: Hiccups can be triggered by severe blood chemistry imbalances. Patients with advanced kidney disease, uncontrolled diabetes, or severe electrolyte imbalances (such as abnormal potassium or sodium levels) frequently develop chronic hiccups 1017. Furthermore, persistent hiccups have recently been identified as a lingering symptom in the post-acute phase of COVID-19 2728.
Medication-Induced Hiccups: Ironically, medical treatments intended to cure other diseases frequently trigger hiccups. Corticosteroids, particularly dexamethasone, are strongly associated with intractable hiccups because steroid receptors are heavily present within the efferent limbs of the hiccup reflex 1721. Chemotherapy drugs, specifically cisplatin, are known triggers 1021. Furthermore, dopamine agonists used to treat Parkinson's disease, as well as various sedatives and anesthesia drugs, regularly disrupt the delicate neurotransmitter balance required to keep the hiccup reflex suppressed 21017.
Folklore and Global Traditions: How We Have Tried to Stop Them
Because the hiccup reflex is built into the human genome, every civilization throughout history has been forced to contend with it. Without an understanding of phrenic nerves and brainstems, ancient cultures understandably attributed the sudden, violent bodily takeover to supernatural forces.
The English word "hiccup" was preceded by the Old English term ælfsogoða, which translates literally to "elf hiccup" 3031. This term arose from the medieval belief that the spasms were the result of invisible elves or demons playing pranks on the victim, an affliction that required herbal exorcisms, Latin verses, and the drawing of crosses to banish the evil spirits 3031. In ancient Greece, prolonged hiccups were interpreted as a sign that someone was actively complaining about the sufferer. A related superstition evolved in Hungary, where hiccups indicated you were the subject of malicious gossip, and in Russia, where they meant a loved one was deeply missing you - a condition that would only resolve when the afflicted person spoke the name of the one longing for them 3031.
The historical remedies devised to cure these supernatural spasms are incredibly diverse. In 16th-century Scotland, sufferers were advised to hold their chin with their right hand while a religious gospel was sung aloud 3031. In Norse traditions, Vikings were instructed to tightly grasp a cloth over their mouth and silently count to one hundred 31. A traditional Norwegian remedy requires the sufferer to take three sips of water from a glass containing a sharp, downward-facing knife while holding their breath 30. In the west of Ireland, a popular folk remedy involves forcing the mind to vividly visualize a green cow grazing peacefully in a blue field 30.
Indigenous and Traditional Medical Systems
In Latin America, the expansive holistic healing tradition of curanderismo - a system that blends ancient Mayan and Aztec herbal lore with Greek humoral medicine and modern Catholicism - views hiccups through a spiritual and energetic lens 32. To cure a hiccuping infant, a curandero or a parent will often place a red string (hilo rojo) directly on the baby's forehead. The color red is believed to absorb negative energy and redirect the spiritual disruption causing the spasm 30. A variation of this remedy is found among the Romani Sinti people, who tie a key to a red string, place it around the neck, and then throw the key over the left shoulder 30.
Similar physical interventions are prominent in traditional African practices. In Nigeria, the cultural treatment for adult hiccups involves specific water-drinking rituals, but for infants, traditional wisdom dictates placing a tiny thread of clothing directly on the child's fontanelle - the soft spot on the skull where the bones have not yet fused 33. In the traditional Yoruba healing system, known as Ogun fún Esuke, mild hiccups are viewed as natural, but prolonged hiccups indicate a systemic imbalance. Yoruba healers utilize warm herbal infusions, direct chewing of bitter roots to "shock" the body, and the application of herbal pastes to the throat and chest to relax the spasms 22.
Traditional Chinese Medicine (TCM) categorizes hiccups (e ni, meaning "rebellious counterflow") as a disruption of the Stomach's natural downward energy. When Stomach Qi rebels and rises upward, it causes belching and hiccups 35. TCM practitioners treat persistent hiccups with targeted acupuncture, specifically utilizing the PC 6 (Neiguan) point on the wrist, the CV 12 (Zhongwan) point on the stomach, and the ST 36 (Zusanli) point on the leg to tonify the stomach and force the Qi to descend 35. This is heavily supported by ancient herbal formulas, such as Ju Pi Zhu Ru Tang (Tangerine Peel and Bamboo Shaving Decoction), which dates back centuries and is still prescribed for post-illness or post-surgical hiccups 35.
Ayurvedic medicine, the traditional healing system of India, links hiccups to an imbalance of the Vata dosha, the energetic force governing movement and the nervous system 2337. Ayurvedic remedies focus on calming the nervous system through warmth and digestion. Common treatments include drinking warm water infused with ginger or tulsi leaves, inhaling the vapors of crushed cardamom or clove, and consuming roasted asafoetida (heeng) mixed with ghee and buttermilk to relieve abdominal distension 2337. Additionally, Ayurvedic practitioners utilize a specific yogic breathing technique, a pranayama called pratiloma, specifically designed to strengthen the diaphragm and regulate breath flow 38.
The Science of Physical Cures: Why Folk Remedies Actually Work
While visualizing a green cow will not alter the contraction of the diaphragm, a surprising number of traditional, physical home remedies are highly effective. When subjected to scientific scrutiny, it becomes clear that these seemingly bizarre rituals succeed because they successfully hack the body's neurology. The vast majority of physical hiccup cures operate by attacking the hiccup reflex arc through two distinct physiological mechanisms: vagal stimulation or hypercapnia 2440.
Mechanism 1: Vagus Nerve Stimulation (Vagal Maneuvers)
The vagus nerve is a massive, wandering neural network that connects the brainstem to the abdomen, regulating the throat, the vocal cords, the heart rate, and the digestive system 841. Because the vagus nerve is a primary sensory highway for the hiccup reflex, overwhelming it with a sudden, intense distraction can force the brainstem to abort the hiccup cycle to process the new sensory input 2543.
Many classic remedies are, in medical terms, covert vagal maneuvers: * Drinking water upside down or gargling ice water: Bending over to drink water from the far side of a glass forces the throat muscles into awkward, highly coordinated contractions. Combined with the intense shock of cold ice water, this heavily stimulates the vagus nerve branches in the pharynx, breaking the reflex cycle 1544. * Swallowing dry sugar or peanut butter: A 1971 study in The New England Journal of Medicine validated the folk cure of swallowing a spoonful of dry, granulated sugar. The granular irritation of the sugar, or the extreme stickiness of peanut butter, forces the esophagus to work unusually hard to swallow, engaging the vagus nerve and overriding the diaphragmatic spasms 234526. * Biting a lemon or tasting vinegar: The intense, sharp acidic shock of pure lemon juice or vinegar activates powerful sensory receptors on the tongue and throat, sending a massive alert signal up the vagus nerve that distracts the brainstem 1545. * Applying physical pressure: Gently pulling outward on the tongue, gently pressing on the eyeballs (the oculocardiac reflex), or applying firm pressure between the jawbone and the mastoid process behind the ear all mechanically stimulate the vagus nerve 152447.
The "Scare" Tactic: Having a friend suddenly jump out and shout "Boo!" is perhaps the most famous hiccup cure. While often dismissed as a childhood game, it has a firm physiological basis. A sudden, genuine fright activates the sympathetic nervous system - the body's "fight or flight" response 25. This adrenaline-fueled state prepares the body for immediate survival, altering breathing patterns and effectively overriding the lower-level autonomous spasms of the hiccup center 2527. However, the scare must be genuine to work, and attempting it in dangerous environments can end in tragedy, as was the case in a fatal 2012 incident at Fort Hood where a soldier was accidentally shot and killed by a peer attempting to startle his hiccups away 25.
Mechanism 2: Increasing Carbon Dioxide (Hypercapnia)
As demonstrated by the tadpole's gill-ventilation mechanism, the brainstem's hiccup center is highly sensitive to carbon dioxide. Raising the concentration of CO2 in the blood - a state known as hypercapnia - acts as a chemical off-switch for the reflex, forcing the brain to prioritize deep, oxygen-seeking respiration over the useless hiccup spasms 114044.
- Holding your breath: This is the most universal and accessible cure. By simply sealing the airway and refusing to exhale, CO2 rapidly builds up in the bloodstream. Eventually, the brain detects the rising toxicity, inhibits the hiccup reflex, and demands a normal breath 4144.
- Breathing into a paper bag: Rapidly rebreathing your own exhaled air quickly cycles carbon dioxide back into the lungs and bloodstream. This elevates CO2 levels faster than breath-holding while still allowing the physical motion of the chest, though it must be done carefully to avoid dizziness or blackout 182344.
Modern Interventions for Acute Hiccups
For acute hiccups that stubbornly resist a spoonful of sugar or a held breath, medical researchers have formalized these physiological principles into highly reliable, structured physical interventions.
The HAPI Technique
Published in 2024, the "Hiccup relief using Active Prolonged Inspiration" (HAPI) technique is a simple, clinically validated method designed to simultaneously hit the reflex arc with vagal stimulation, phrenic stimulation, and hypercapnia 254028. In clinical trials, it demonstrated a 100% immediate success rate for self-limited hiccups 2829.
To perform the HAPI technique correctly: 1. Inhale maximally, taking in as much air as the lungs can possibly hold. 2. Once at the absolute peak of inspiration, do not simply hold your breath (which closes the glottis). Instead, keep the airway open and continue attempting to inhale against the full lungs for a total of 30 seconds 4028. 3. After 30 seconds of active inspiratory effort, slowly exhale and resume normal breathing 28.
The genius of the HAPI method lies in the active effort. Standard breath-holding allows the diaphragm to relax against a closed throat. By constantly attempting to pull air in, the diaphragm is locked into a state of maximum, unyielding contraction. This provides a continuous, overwhelming stimulus to the phrenic nerve while simultaneously driving up carbon dioxide levels, effectively short-circuiting the hiccup mechanism 40.
Specialized Inspiratory Devices
Innovations in biomedical design have resulted in the "forced inspiratory suction and swallowing tool" (FISST), most widely marketed to consumers as the HiccAway straw 3827.
The device is a rigid plastic tube featuring a highly restrictive pressure valve at the bottom. The user places the straw in a glass of water and attempts to drink. Because the valve is incredibly tight, it requires immense suction force to draw the water upward. This intense suction forces the diaphragm to contract deeply and forcefully, which heavily stimulates the phrenic nerve 838. Once the water reaches the mouth, the act of swallowing it engages the vagus nerve and forces the glottis to close normally.
By forcing the phrenic nerve and the vagus nerve to simultaneously perform intense, coordinated work, the device completely occupies the neural pathways required for a hiccup. In a sweeping 2021 study published in JAMA Network Open, the device demonstrated a 92% efficacy rate in stopping hiccups across a diverse patient population 83827.
Treating Persistent and Intractable Hiccups
When hiccups bypass the 48-hour mark, physical interventions like holding your breath or drinking upside down are almost universally ineffective. Treating persistent and intractable hiccups requires a thorough clinical investigation to identify and treat the root pathology, followed by aggressive pharmacological intervention if the cause cannot be resolved 2430.
Because GERD is the most common hidden cause, the initial medical response is often to prescribe a vigorous 4-to-8-week course of proton pump inhibitors (PPIs) like omeprazole, taken daily before meals. By drastically reducing stomach acid, the irritation to the esophageal vagus nerve endings is eliminated, which frequently cures the hiccups 283153.
If the patient is undergoing chemotherapy or taking high doses of corticosteroids (like dexamethasone), physicians may attempt "steroid rotation" - swapping the dexamethasone for an alternative like methylprednisolone, which has been shown to successfully halt medication-induced hiccups without interrupting cancer treatments 272832.
If the root cause is untreatable - such as advanced cancer, permanent brainstem damage from a stroke, or severe organ failure - physicians must turn to systemic medications that cross the blood-brain barrier. These drugs do not fix the underlying disease; rather, they chemically dampen the neurotransmitters in the brainstem's hiccup center to force the reflex into submission 314.
Pharmacological Guidelines
Current medical guidelines recommend a stepwise approach to prescribing, prioritizing newer drugs with safer side-effect profiles before resorting to heavy antipsychotics 3053.
| Medication | Clinical Role & Evidence | Mechanism of Action | Notable Risks & Side Effects |
|---|---|---|---|
| Baclofen | First-line therapy. Supported by multiple randomized controlled trials. Highly effective for chronic/intractable hiccups 283031. | A GABA-B receptor agonist. It mimics inhibitory neurotransmitters, creating a perceptual blockage in synaptic transmission within the reflex arc 31. | Sedation, dizziness, ataxia, and confusion. Must be used carefully in older adults or those with renal impairment 31. |
| Gabapentin | First-line alternative. Often used as monotherapy or added to baclofen. Safe for long-term use 283053. | An anticonvulsant that modulates peripheral and central nerve signaling, particularly useful when hiccups stem from CNS lesions 30. | Generally well-tolerated; mild somnolence, dizziness, and fatigue 53. |
| Metoclopramide | Second-line therapy. Recommended when gastric motility issues are suspected 2830. | A dopamine antagonist and prokinetic agent. It speeds up stomach emptying and tightens the esophageal sphincter, reducing acid reflux 2830. | High risk of extrapyramidal symptoms and tardive dyskinesia (involuntary muscle movements) with long-term use 30. |
| Chlorpromazine | Last resort (Refractory cases). Historically the drug of choice; the only medication officially FDA-approved for hiccups 273155. | A phenothiazine antipsychotic. It acts centrally via heavy dopamine antagonism in the hypothalamus 31. | Severe risks: hypotension, urinary retention, delirium, glaucoma, and severe cardiac toxicity (arrhythmias) 2731. |
Surgical and Neuromodulation Interventions
In the most extreme cases, where intractable hiccups ruin a patient's life and all pharmacological options fail, invasive procedures become necessary.
Clinicians may utilize a continuous positive airway pressure (CPAP) machine to forcefully keep the airway open and alter thoracic pressure 18. Anesthesiologists can perform nerve blocks, injecting numbing agents directly into the phrenic or vagus nerves to temporarily paralyze the signal pathways 1821. The ultimate surgical intervention involves the implantation of a Vagus Nerve Stimulator (VNS). This pacemaker-like device is surgically embedded in the chest and wired directly to the vagus nerve in the neck, delivering rhythmic electrical pulses to constantly override the erratic hiccup signals, though success rates vary wildly depending on the root cause of the spasms 643.
Bottom line
Hiccups are a complex, automated neurological sequence involving a sudden spasm of the diaphragm followed by the violent closure of the vocal cords. Evolutionary evidence strongly suggests this useless human reflex is a vestigial trait inherited from ancient amphibians, utilizing the exact same brainstem wiring that allows tadpoles to breathe through their gills. While everyday hiccups are easily triggered by a full stomach or spicy foods and can be swiftly cured by remedies that stimulate the vagus nerve or elevate carbon dioxide, hiccups lasting beyond 48 hours are no longer benign. Chronic episodes demand immediate medical investigation, as they frequently signal severe acid reflux, central nervous system damage, or metabolic failure, requiring targeted pharmacological interventions like baclofen or gabapentin to silence the misfiring circuitry.