Why Bright Light Makes Some People Sneeze
The photic sneeze reflex is an inherited neurological anomaly where sudden exposure to bright light triggers an involuntary, rapid succession of sneezes. While the exact biological mechanism remains the subject of ongoing research, scientists hypothesize that it originates from a structural "crossed wire" in the brainstem, wherein the optic nerve's intense electrical response to light accidentally stimulates adjacent nerve pathways responsible for clearing nasal irritation.
What Is the Photic Sneeze Reflex?
For the vast majority of the human population, sneezing is a straightforward, mechanical reflex. An external irritant - such as dust, animal dander, pollen, or pepper - enters the nasal cavity, stimulating the mucosal lining. The body then orchestrates a complex, forceful expulsion of air to clear the airway. However, for a significant and globally distributed minority of people, the simple act of stepping out of a dimly lit space into bright sunlight induces an identical, explosive physiological response 11.
This phenomenon is formally recognized in the medical literature as the photic sneeze reflex (PSR). It is also frequently referred to by the somewhat contrived, humorous acronym ACHOO syndrome, which stands for Autosomal Dominant Compelling Helio-Ophthalmic Outburst 112. Additional clinical terms for the condition include photosneezia and solar sneezing 14.
Unlike an allergic sneeze or a reflex triggered by a cold, a photic sneeze originates entirely within the brain rather than in the nasal mucosa 1. The reflex is uniquely triggered not by the ambient presence of light itself, nor by exposure to specific, isolated wavelengths of the light spectrum, but by a sudden and dramatic change in light intensity 123. For instance, sitting in a brightly lit room or spending hours on a sunlit beach rarely causes continuous, uninterrupted sneezing. The reflex is almost exclusively activated during the sharp transition from relative darkness to blinding light - such as driving out of a long, dark tunnel, exiting a movie theater into the afternoon sun, or having an optometrist suddenly shine a bright examination light into the eyes 247.
When exposed to this sudden stimulus, most photic sneezers experience a distinct "burst" or paroxysm of successive sneezes. Clinical observations indicate that the number of sneezes per episode generally ranges from one to ten 43. Once the sneezing fit concludes, the neurological pathways enter a refractory period. During this temporary window - which can sometimes last for up to 24 hours - subsequent exposure to intense light will not trigger another sneezing episode, suggesting a temporary depletion of the neurotransmitters or a resetting of the specific reflex arc 3.
The Historical Documentation of Sun Sneezing
While modern genomics and neurobiology are only now beginning to unravel the precise mechanisms of the photic sneeze reflex, the phenomenon has been documented by scholars and physicians for millennia. The earliest known reference to light-induced sneezing is widely attributed to the ancient Greek philosopher Aristotle, who observed the curious tendency for individuals to sneeze when looking at the sun 8. For centuries, the observation remained a minor medical curiosity, often misattributed to the sun's heat warming the nose rather than the light entering the eyes.
It was not until the late nineteenth and early twentieth centuries that physicians began to seriously codify the reflex within the framework of modern neurology. In 1875, William Spencer Watson proposed early theories regarding parasympathetic co-activation, and in 1919, Albert Philson Brubaker published "The Physiology of Sneezing" in the Journal of the American Medical Association, laying the groundwork for understanding the cross-talk between facial nerves 56. Decades later, in 1943, Lisgar Bowne Eckhardt formally introduced the optical-trigeminal summation theory, suggesting that the anatomical proximity of the optic and trigeminal nerves was responsible for the phenomenon 5.
Subsequent clinical testing further established the reflex's physiological complexity. In 1989, researchers measured the latency of the photic sneeze reflex - the time between light exposure and the resulting sneeze - at an average of 9.9 seconds. This delayed response time clearly indicated that photic sneezing is a highly complex, polysynaptic phenomenon involving multiple relay stations in the brain, rather than a simple, direct neural loop 5.
Global Prevalence and Demographic Distribution
Historically, the photic sneeze reflex was considered a curious but highly prevalent quirk. Early literature broadly estimated that it affected between 18% and 35% of the general human population, leading many to believe that up to one in three people carried the trait 123. However, large-scale modern epidemiological surveys and genome-wide association studies (GWAS) have revealed that the prevalence of this reflex is not uniform; it varies drastically depending on the specific population and geographic region being studied.
An influential 1995 survey conducted in an academic optometry clinic in Alabama found that 33% of patients self-identified as photic sneezers. However, in this specific clinic cohort, the trait appeared to be highly skewed by demographic factors: an overwhelming 94.3% of the identified sneezers were Caucasian, and 67% were female 437. For a time, this isolated data set led to the generalized assumption that white women were at the absolute highest risk for developing ACHOO syndrome.
More recent, highly rigorous genetic and epidemiological studies have challenged this notion, proving that the trait is pan-ethnic, though it manifests at wildly different rates across different regions of the world 8.
| Population / Study Region | Estimated Prevalence | Key Demographic and Methodological Notes |
|---|---|---|
| Germany (Hospital Cohort) | 57.0% | A 2017 cross-sectional study of 1,042 otolaryngology patients found an unusually high prevalence among regular light-induced sneezers, far exceeding global averages 6910. |
| United States (Clinic Survey) | 33.0% | A 1995 optometry clinic study heavily skewed toward Caucasian (94.3%) and female (67%) respondents 7. |
| United States (General Estimate) | 18.0% - 35.0% | Broad, baseline population estimates frequently cited in western medical literature and neurobiology textbooks 123. |
| China (GWAS Population) | 25.6% | A 2019 GWAS of 3,417 individuals found a higher prevalence in males (30.1%) than females (21.1%), contradicting earlier Western gender demographic assumptions 8. |
| Japan (GWAS Population) | 3.2% | A vast genomic study of 11,409 individuals showed a remarkably low prevalence compared to Western and Chinese populations, indicating strong regional genetic variance 815. |
Interestingly, absolute uniformity in the photic sneezing response is exceedingly rare, even among those who possess the trait. The 1995 clinical study noted that only 12.3% of self-identified sneezers responded consistently to sunlight exposure every single time they encountered it 47. Furthermore, a recent review of literature from 2020 to 2024 evaluating the specific stimulus conditions of the reflex noted that while bright light reliably induces sneezing in susceptible individuals, there is a total lack of standardized research defining the exact parametric relationship between light intensity, wavelength, and the sneeze response 16. This suggests that there is a specific, highly individualized threshold of light intensity or spatial configuration required to trigger the reflex, which varies substantially from person to person 716.
The Genetic Architecture of ACHOO Syndrome
The "Autosomal Dominant" portion of the ACHOO acronym explains the historical understanding of how the trait is inherited. If a biological parent possesses the photic sneeze reflex, their offspring has a 50% chance of inheriting the condition 29.
For many years, clinical geneticists assumed that because the inheritance pattern was so predictably dominant within family trees, ACHOO syndrome was a Mendelian trait - meaning it was controlled by a single, isolated genetic mutation 817. This assumption has been entirely overturned by the advent of modern, high-throughput genetic sequencing.
Current scientific consensus confirms that the photic sneeze reflex is a complex, polygenic trait. This means that the phenotype is governed not by a single master gene, but by the collective, cumulative effect of numerous genetic variants (polymorphisms) scattered across multiple chromosomes throughout the human genome 8917. Researchers analyzing vast repositories of data from direct-to-consumer DNA testing companies, which included over 110,000 consenting customers primarily of European descent, have identified at least 54 different genetic markers associated with the expression of the reflex 1718.
Key Genetic Loci: ZEB2 and CADM2
Large-scale genetic research, most notably a massive 2019 Genome-Wide Association Study (GWAS) conducted on a Chinese population, has successfully isolated several specific Single Nucleotide Polymorphisms (SNPs) that are robustly associated with the reflex across different ethnicities 8.
The most prominent genetic marker is rs10427255, located on chromosome 2 at the 2q22.3 locus. This SNP is situated near the ZEB2 (Zinc Finger E-Box Binding Homeobox 2) gene 148. The ZEB2 gene is highly significant because it plays a critical foundational role in neurogenesis; it is responsible for producing proteins that orchestrate the formation of nerve cells and vital neural architecture before birth 4. In both the United States and Chinese populations, specific variations (minor alleles) at this locus significantly increase the statistical risk of developing ACHOO syndrome (with an odds ratio of 1.68 in the Chinese cohort) 8.
A second independent locus, rs1032507, was discovered on chromosome 3 (3p12.1) during the Chinese GWAS 8. This marker is located near the CADM2 gene, which is involved in synapse adhesion - the process by which neurons physically connect and communicate with one another 8. Interestingly, possessing the minor allele at this specific locus actually reduces the risk of experiencing the photic sneeze reflex (with an odds ratio of 0.65) 8. This locus is also physically adjacent to other genetic markers (rs1691483 and rs1694933) that were independently identified in the Japanese population studies 8.
Other candidate SNPs have been identified, including rs11856995 on chromosome 15 (15q26.2), though its significance varies by population 8. Ultimately, the discovery that the primary genes associated with photic sneezing govern general neural development (ZEB2) and synaptic adhesion (CADM2) heavily supports the prevailing neurological theory: that the photic sneeze reflex is the result of a structural, anatomical quirk in how the brain's neural networks are wired together during embryonic development.
Neurological Mechanisms: Uncrossing the Wires
To comprehend why sunlight causes a person to sneeze, it is necessary to first understand the complex neurology of a standard, pathogen-induced sneeze.
A normal sneeze is initiated when a noxious stimulus irritates the receptors in the nasal mucous membranes. This sensory information is gathered and transmitted predominantly via the naso-palatine nerve, which is a branch of the maxillary nerve (Cranial Nerve V2, part of the broader trigeminal nerve network) 35. The trigeminal nerve carries this signal directly to the trigeminal nerve nuclei in the brainstem - specifically to a putative "sneezing center" located in the medulla oblongata 35.
Once the medulla processes this irritation, it triggers a massive, systemic efferent response. It activates parasympathetic fibers running to the superior salivatory nucleus, and initiates a complex motor pattern: a deep inspiration of air, the tilting back of the head, involuntary eye closure, and the tight closure of the naso-pharynx and glottis. This total airway closure allows immense intrathoracic pressure to build up in the lungs, followed instantly by the opening of the glottis and an explosive expulsion of air through the nose and mouth, designed to dislodge the irritant 5.
In individuals with the photic sneeze reflex, this exact same complex motor pattern is executed perfectly. However, the inciting trigger does not originate in the nose. Instead, the signal comes from the eyes, traveling via the optic nerve (Cranial Nerve II) 5. Researchers have proposed three primary neuroanatomical theories to explain this biological crossover.
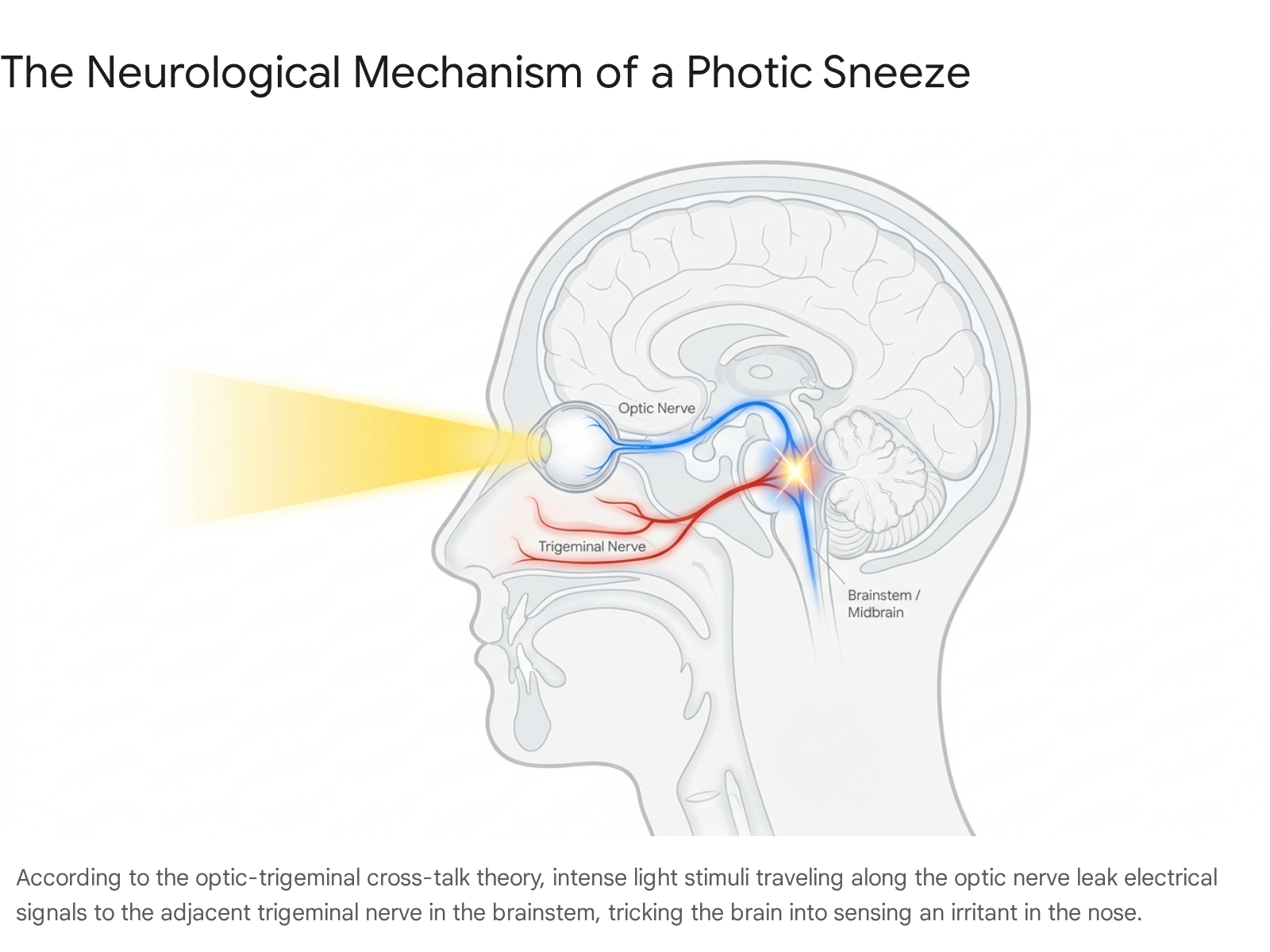
The Optic-Trigeminal Summation (Cross-Talk) Theory
The most widely accepted explanation among neurologists is the "optic-trigeminal summation" or "cross-talk" theory. The human nervous system transmits electrical signals at incredibly high speeds, and in the densely packed anatomy of the brainstem, sensory pathways frequently run in close physical proximity to one another 311.
When an individual steps into intense sunlight, the sudden burst of light hits the retina, prompting the optic nerve to rapidly fire massive volleys of electrical signals into the midbrain (mesencephalon) to process the light and constrict the pupils 611. The neural pathways for the optic nerve and the trigeminal nerve are located very close together in this region of the brainstem 5611.
In people with ACHOO syndrome, it is hypothesized that the intense burst of electrical activity from the optic nerve essentially "leaks" or induces a signal over into the adjacent trigeminal nerve 1311. The brain misinterprets this errant, leaked electrical signal as a genuine, intense tickle in the nasal cavity. Reacting exactly as it was programmed to do, the brain immediately triggers the full sneeze reflex arc 1311.
The Parasympathetic Generalization Theory
A secondary, highly detailed physiological theory focuses not on the direct sensory nerves, but on the parasympathetic nervous system, which controls the body's unconscious, resting functions.
When bright light enters the eyes, the optical data is transmitted to the pretectal olivary nucleus in the midbrain, which relays the signal directly to the Edinger-Westphal (EW) nucleus 20. The primary job of the EW nucleus in this context is to immediately send parasympathetic preganglionic fibers down the oculomotor nerve (Cranial Nerve III) to the ciliary ganglion, instructing the pupil to violently constrict to protect the retina from light damage (the pupillary light reflex) 20.
However, the parasympathetic nervous system is highly interconnected, with neighboring fibers responding to drastically different stimuli. The "parasympathetic generalization" theory suggests that when the EW nucleus fires to constrict the pupil, the intense neural activation accidentally spills over, co-activating adjacent parasympathetic branches 356. Anatomical studies have demonstrated that nerves passing through the ciliary ganglion also travel to the rostral part of the pterygopalatine ganglion 20.
The pterygopalatine ganglion is a critical cluster of nerves that controls the sphenopalatine nerve, which distributes to the nasal mucosa and palate. When stimulated, it induces profound vasodilation (the widening of blood vessels) and rapid mucus secretion in the nose 20. Under this theory, the sudden exposure to bright light causes an instantaneous, micro-dilation of blood vessels and a burst of mucus in the nasal cavity. This sudden, purely physical change in the nasal tissue creates a very real physiological tickle, which then naturally triggers the standard sneeze reflex 320.
The Trigeminocardiac Reflex (TCR) Connection
Recent neurobiological literature has drawn fascinating conceptual and anatomical parallels between the photic sneeze reflex and a much more severe brainstem reaction known as the trigeminocardiac reflex (TCR).
The TCR is a well-documented clinical reflex where the stimulation of any of the sensory branches of the trigeminal nerve causes a sudden, dangerous drop in heart rate (parasympathetic dysrhythmia), low blood pressure (sympathetic hypotension), apnea, and gastric hypermotility 69. It has been linked to severe clinical events, including sudden infant death syndrome (SIDS), sleep disorders, and stroke 69.
Researchers note that both the photic sneeze reflex and the TCR share common anatomical origins. Both phenomena are initiated by the fifth cranial nerve, both can be triggered by temperature and light, and both involve interconnected brainstem pathways linking cranial nerves V, VII, IX, XI, and XII with vagal (tenth cranial nerve) outflow 6. Crucially, both reflexes are accompanied by extreme parasympathetic over-activity 6.
Given these structural similarities, some researchers hypothesize that ACHOO syndrome may actually be a highly specific, low-risk variant or subtype of the broader trigeminocardiac reflex. Investigating this connection could yield a deeper understanding of brainstem functionality and potentially open new avenues for treating severe dysautonomic conditions 46.
Anatomical Quirks and Alternative Triggers
While an individual's underlying genetic code dictates the baseline presence of the photic sneeze reflex, specific physical anatomical anomalies can significantly exacerbate the likelihood and severity of the condition.
Multiple epidemiological studies have found a statistically significant correlation between the photic sneeze reflex and a deviated nasal septum - a condition where the bone and cartilage that divide the nasal cavity are displaced or off-center, often due to injury 243715. The exact reason for this association remains unproven, but a deviated septum may increase the baseline physical sensitivity of the trigeminal nerve endings in the asymmetric nasal passage.
Ocular anatomy also plays a surprising role. A small-scale study comprising a family from Spain revealed that individuals with prominent corneal nerves in their eyes were vastly more likely to experience photic sneezing (with 67% of those with prominent nerves exhibiting the reflex) 43. Furthermore, a clinical study noted that 26% of patients suffering from nephropathic cystinosis - a metabolic disease characterized by the deposition of crystals in the cornea - exhibited photic-induced sneezes during routine ophthalmoscopic examinations 8.
Iatrogenic Triggers: Anesthesia and Eye Injections
Because the trigeminal nerve provides sensory data for the entire face, individuals with ACHOO syndrome often find that their reflex can be triggered by stimuli entirely unrelated to light. Clinical environments, particularly those involving facial anesthesia, are a primary trigger zone.
A notable, highly specific trigger is the administration of periocular injections - local anesthesia injected directly around the eyeball prior to delicate eye surgery 243. Because this needle insertion directly and intensely stimulates the ophthalmic branch of the trigeminal nerve, patients with a genetic predisposition for ACHOO syndrome frequently experience immediate, uncontrollable sneezing while the needle is resting near their eye. Studies indicate that up to 23.8% of susceptible patients develop sneezing following periocular injections, compared to only 4.5% after retrobulbar injections 21.
Certain intravenous sedatives routinely used in operating rooms can also induce violent sneezing fits. The administration of propofol is a known trigger, and deep sedation generally triples the risk of a sneezing event 21. Midazolam has been shown to double the risk of sneezing. Conversely, researchers have found that the administration of opioid derivatives, dexmedetomidine, and antihistamines serve as a highly effective, protective suppressant against reflex sneezing during surgery 82122.
Related Parasympathetic Phenomena
The cross-wiring of the parasympathetic nervous system that enables photic sneezing may also explain other unusual, non-nasal triggers for sneezing. Clinical reports exist documenting individuals who sneeze uncontrollably in response to a heavily full stomach following a large meal, or, more unusually, in response to sexual ideation and orgasm 212.
Researchers theorize that all of these phenomena share parasympathetic outflow as a common denominator. Much like the pupillary constriction in the photic sneeze reflex, gastric peristalsis (triggered by a full stomach) and venous dilation (triggered by sexual arousal) are heavily mediated by parasympathetic activity. The "parasympathetic summation" theory suggests that in genetically susceptible individuals, massive parasympathetic spikes in the digestive or reproductive systems can leak into the respiratory centers, triggering an identical sneeze response 12.
Safety Hazards in the Modern World
In isolation, the act of sneezing is an entirely harmless, universally experienced biological function. However, because the photic sneeze reflex is triggered instantaneously by intense visual stimuli, it frequently occurs in environments where sudden, involuntary eye closure (a mandatory physiological component of a sneeze) and a momentary loss of bodily control are exceptionally dangerous 2.
Motor Vehicle Operation
The most common and immediate hazard for photic sneezers is operating a motor vehicle, specifically due to what researchers call the "tunnel effect." Exiting a dark, shaded tunnel or a deeply forested road directly into bright, blinding sunlight is the perfect environmental catalyst for a photic sneeze 29.
Because a standard sneeze forces a human to involuntarily close their eyes for a second or more, a burst of three to five successive sneezes while traveling at highway speeds leaves a driver completely blind to the road and surrounding traffic for hundreds of feet 2. This is not a purely theoretical risk. Medical case studies have documented the severe reality of this issue, including a clinical report detailing a 26-year-old individual who was involved in three separate motor vehicle crashes directly linked to sudden, sunlight-induced sneezing fits 1.
Aviation and Combat Risks
The physical danger of the reflex is drastically magnified in the realm of aviation, where split-second reaction times and spatial awareness are critical. A landmark 1993 study published in Military Medicine explicitly investigated the photic sneeze reflex, ultimately classifying it as an "unrecognized and previously unreported danger to fixed-wing and rotary aircraft pilots" 13.
During aerial combat, high-speed low-altitude flying, or complex flight maneuvers, a pilot banking their aircraft and suddenly facing into the bright sun could be completely incapacitated by a sneezing fit during a highly critical window of operation 714. To investigate exactly how to mitigate this risk, military researchers tested susceptible subjects using specific wavelengths of light through narrow-band interference filters (at 430, 532, and 560 nm) 13.
The clinical testing confirmed that the sneezes were triggered purely by the sudden, overwhelming change in overall light intensity, and not by any specific light colors or wavelengths. Consequently, standard, wavelength-blocking colored aviation goggles and sunglasses were deemed insufficient to reliably stop the reflex if the ambient light shift was bright enough 1326.
Surgical and Medical Risks
For patients undergoing intricate dental, oral, or ophthalmic operations, the blindingly bright surgical lights that are routinely directed at their faces can easily trigger the reflex 3. Sneezing violently while a surgeon is operating with sharp instruments inside the mouth or directly on the eye poses a severe physical risk to the patient and the physician 1.
Consequently, medical experts strongly advise that patients who are aware of their photic sneeze reflex explicitly inform their healthcare providers prior to surgery. This allows the anesthesiology and surgical teams to physically stabilize the patient's head, avoid specific triggers like midazolam, or administer preventative protective suppressants (such as opioids or antihistamines) prior to activating the surgical lamps or performing periocular injections 1222.
Mitigation and Management Strategies
Because ACHOO syndrome is deeply written into an individual's genetic code and fundamentally tied to the anatomical structure of the brainstem, there is no pharmaceutical cure or surgical procedure to permanently eliminate the reflex 112. Management of the condition primarily relies on simple environmental mitigation and specific physical interruption techniques.
- Anticipatory Shielding: The single most effective management technique is preventing the sudden, stark change in light intensity before it hits the retina. Wearing heavily polarized, dark sunglasses or wide-brimmed hats before stepping out of a dark building or exiting a tunnel limits the optical shock, effectively bypassing the reflex altogether 112.
- The Transverse Philtral Pressure Technique: If a photic sneezer is caught off guard and feels the distinct, pre-sneeze tickle emerging in their nasal cavity, they can often abort the reflex by applying firm, physical pressure to the philtrum - the small, vertical divot between the upper lip and the base of the nose. By pressing a finger horizontally under the nose (resembling a finger mustache), the mechanical pressure effectively overrides the trigeminal nerve's delicate irritation signals, short-circuiting the motor reflex before it can execute 1.
- Allergy Management: While photic sneezing is entirely distinct in its origin from allergic rhinitis, allergists note that preexisting, chronic nasal inflammation can make the trigeminal nerve endings hyper-sensitive to any stimulus. Patients with untreated hay fever or seasonal allergies are often much more prone to violent, extended photic sneezing fits. Taking regular over-the-counter antihistamines to reduce the baseline inflammation in the nasal cavity can raise the overall neurological threshold required to trigger a sun sneeze, making the reflex less frequent and less severe 12.
Bottom line
The photic sneeze reflex, colloquially known as ACHOO syndrome, is a common, genetically inherited polygenic trait that causes individuals to experience a rapid burst of sneezes upon sudden exposure to bright light. While the precise biological mechanism is still the subject of ongoing neurobiological study, the prevailing scientific consensus points to crossed electrical pathways in the densely packed brainstem, where optic nerve signals inadvertently "leak" into and trigger the trigeminal nerve. Though generally considered a mild, harmless physiological quirk, the reflex can pose genuine, documented safety hazards for individuals operating motor vehicles, piloting high-speed aircraft, or undergoing delicate facial surgeries.